
Abstract
Background:
Historically, Lisfranc injuries have most commonly been managed by open reduction and internal fixation (ORIF). Over the past 2 decades, literature has suggested that arthrodesis, an alternative option, may be the superior surgical treatment. It is unclear, however, how much orthopaedic clinical practice has responded to the new evidence.
Methods:
We performed a retrospective review of the Part II Oral Examination Case List American Board of Orthopaedic Surgery (ABOS) database to identify Lisfranc injuries treated with ORIF or arthrodesis from 1999 to 2022. Cases performed by early-career orthopaedic surgeons were selected using relevant Current Procedural Terminology, International Classification of Diseases, Ninth (ICD-9) and Tenth Revision (ICD-10), codes corresponding to treatment with either arthrodesis or ORIF. Treatment trends were analyzed over time and stratified by surgeon fellowship training, patient age, and patient sex. Injury chronicity and specific timing from injury to surgery were not available.
Results:
A total of 3068 surgically managed Lisfranc injuries were identified. Of these, 574 (18.7%) were managed with arthrodesis and 2494 (81.3%) with ORIF. The rate of arthrodesis increased over time: from 7.7% (95% CI 6.3-9.3) in 1999-2009 to 20.7% (95% CI 18.5-23.1) in 2010-2017 (P < .0001) and to 37.0% in 2018-2022 (95% CI 33.3-40.9) (P < .0001). The rate of arthrodesis was higher among cases performed by foot and ankle–trained orthopaedists (30.3% vs 7.9% of all other sub-specialties), in female patients (22.4% vs 15.9% in males), and in older patients (27.8% of patients >50 years vs 15.4% of patients ≤50 years).
Conclusion:
Although still the less utilized approach, arthrodesis for Lisfranc injuries has increased substantially among early-career orthopaedic surgeons in parallel to emerging evidence. This trend is more apparent among foot and ankle specialists.
Level of Evidence:
Level III, therapeutic.
Keywords
Introduction
Unstable traumatic ligamentous injuries at the tarsometatarsal joints with or without bony or intertarsal involvement are referred to as Lisfranc injuries. Lisfranc injuries are uncommon, occurring in 9.2-22.4 per 100 000 person-years, although they are frequently missed on initial evaluation.1,2 These injuries typically arise from an axial load and rotational force to the plantar-flexed foot and, if left untreated, can lead to midfoot instability, early degeneration, and arch collapse, resulting in significant functional consequences, especially in young, active patients. 3 As such, surgical management is often indicated for unstable injuries.
There is no consensus on surgical strategy, especially regarding arthrodesis vs open reduction internal fixation (ORIF). Some consider arthrodesis as a salvage procedure after failed ORIF, whereas others favor it as a primary treatment because of the limited ligamentous healing potential. 4 Historically, the standard of care was ORIF for most cases; however, patient outcomes are limited by high rates of post-traumatic arthritis, reoperation, and decreased function. 5 Arthrodesis may in turn be complicated by nonunion and additional functional limitations. 6
In 2006, a randomized controlled trial (RCT) by Ly and Coetzee 7 demonstrated superior outcomes after arthrodesis for primary treatment of ligamentous Lisfranc injuries. Subsequent studies showed similar8 -12 or superior13 -16 results with validated pain and functional outcome measurements in both ligamentous injuries and fracture-dislocations. However, it remains unclear how this evidence has influenced clinical management. This study utilized the American Board of Orthopaedic Surgery (ABOS) Part II Oral Examination Case List Database, which has previously been used to study trends among early-career surgeons.17 -24
The primary objective of this study was to compare the incidence of arthrodesis and ORIF treatment for Lisfranc injuries performed during surgeons’ ABOS Part II Board Certification case collection period. Arthrodesis rates were also examined based on subspecialty training and patient sex and age. The hypothesis was that the rate of arthrodesis would increase over the study period, with higher adoption among foot and ankle specialists, where practice patterns are more likely to reflect emerging foot and ankle literature.
Methods
The ABOS Part II Oral Examination Case List Database was queried for surgically managed Lisfranc injuries from 1999 to 2022. This database includes all cases submitted to the ABOS by early-career orthopaedic surgeons as part of the ABOS Part II Oral Examination Case List, which includes a 6-month collection of consecutive surgical cases.
Surgically managed Lisfranc injuries were identified by a combination of Current Procedural Terminology (CPT) and International Classification of Diseases (ICD) codes. Arthrodesis was identified by CPT codes 28730, 28735, and 28740. ORIF was identified by CPT codes 28606, 28615, 28465, and 28485. In situations where CPT codes for arthrodesis and ORIF were concomitantly used, cases were classified as arthrodesis because a fusion was involved in the ultimate construct as opposed to fixation alone. Lisfranc injuries were identified by ICD-9 codes 838.02, 838.03, 838.04, 838.12, 838.13, 838.14, and 845.11 and ICD-10 codes s93.321, s93.322, s93.323, s93.324, s93.325, s93.326, and s93.622. All CPT and ICD codes included are detailed in Appendix A. Timing between injury and surgery were not available and thus unable to be incorporated into the analyses. Both open and closed injuries were included in the analyses.
Two analyses were performed: one with a broad definition of Lisfranc injury and a subgroup analysis with a narrower definition to examine ligamentous-only injuries. In the subgroup analysis, CPT and ICD codes indicating a tarsal or metatarsal fracture were excluded (Appendices A and B).
Three key time periods were identified after review of the literature. Data from 1999 to 2009 represent surgeons who finished training before the first study in 2006 suggesting superior outcomes with arthrodesis over ORIF. 7 Data from 2009 to a large extent represent surgeons who finished residency in 2006, fellowship in 2007, collected cases in 2008, and submitted cases in 2009. Data from 2010-2017 represent surgeons who trained during the introduction and possible adoption of this first evidence and change in practice. Data from 2018-2022 represent surgeons who trained during and after a larger emergence of literature favoring arthrodesis over ORIF.13,14,25
Patient age and sex were included. All patients aged <18 years were excluded. Patient race and ethnicity data were not available. Surgeon fellowship was self-reported. Surgeons reporting multiple subspecialties were categorized as “foot and ankle” if any reported subspecialties included foot and ankle, “sports medicine” if any included sports medicine but not foot and ankle, “trauma” if any included trauma but not foot and ankle or sports medicine, and “other” for all others.
Statistical Analysis
The rates of arthrodesis and ORIF were reported overall, by time range, by fellowship training, sex, and patient age, and by subgroups within each time range. Chi-square tests were used to compare the rates of arthrodesis across these subgroups. Generalized linear models with a binomial distribution and logit link function were used to estimate the rate of arthrodesis and its 95% CI within each time range and by fellowship training, patient sex, and patient age. Post hoc pairwise comparisons across the time ranges were conducted within the model via orthogonal contrasts. The Holm test was used to adjust P values for multiple comparisons to maintain a 2-tailed familywise alpha of .05. Segmented or bent stick regression was used to test whether the rate of growth differed within each time range, overall and by subgroup. A P value <.05 was used to determine statistical significance. Data were analyzed using SAS version 9.4 (SAS Institute Inc, Cary, NC).
Results
From 1999 to 2022, a total of 3068 surgically managed Lisfranc injuries were identified in the ABOS Part II Oral Examination Case List Database. There were 574 injuries managed with arthrodesis (18.7%) and 2494 managed with ORIF (81.3%) (Table 1). The rate of arthrodesis was higher among cases performed by foot and ankle–trained orthopaedists (30.3% [449/1483], compared with 7.9% of all other subspecialties [125/1585]), female patients (22.4% [299/1337] vs 15.9% male [275/1731]), and older patients (27.8% of patients >50 [226/814] vs 15.4% of patients ≤50 [348/2254]) (Table 1). Similar trends were observed in the ligamentous-only subgroup (Appendix B1). A total of 270 patients (8.8%) had CPT codes for both ORIF and arthrodesis and were classified in the arthrodesis group.
Rates of ORIF and Arthrodesis Performed by Early-Career Orthopaedic Surgeons, 1999-2022.
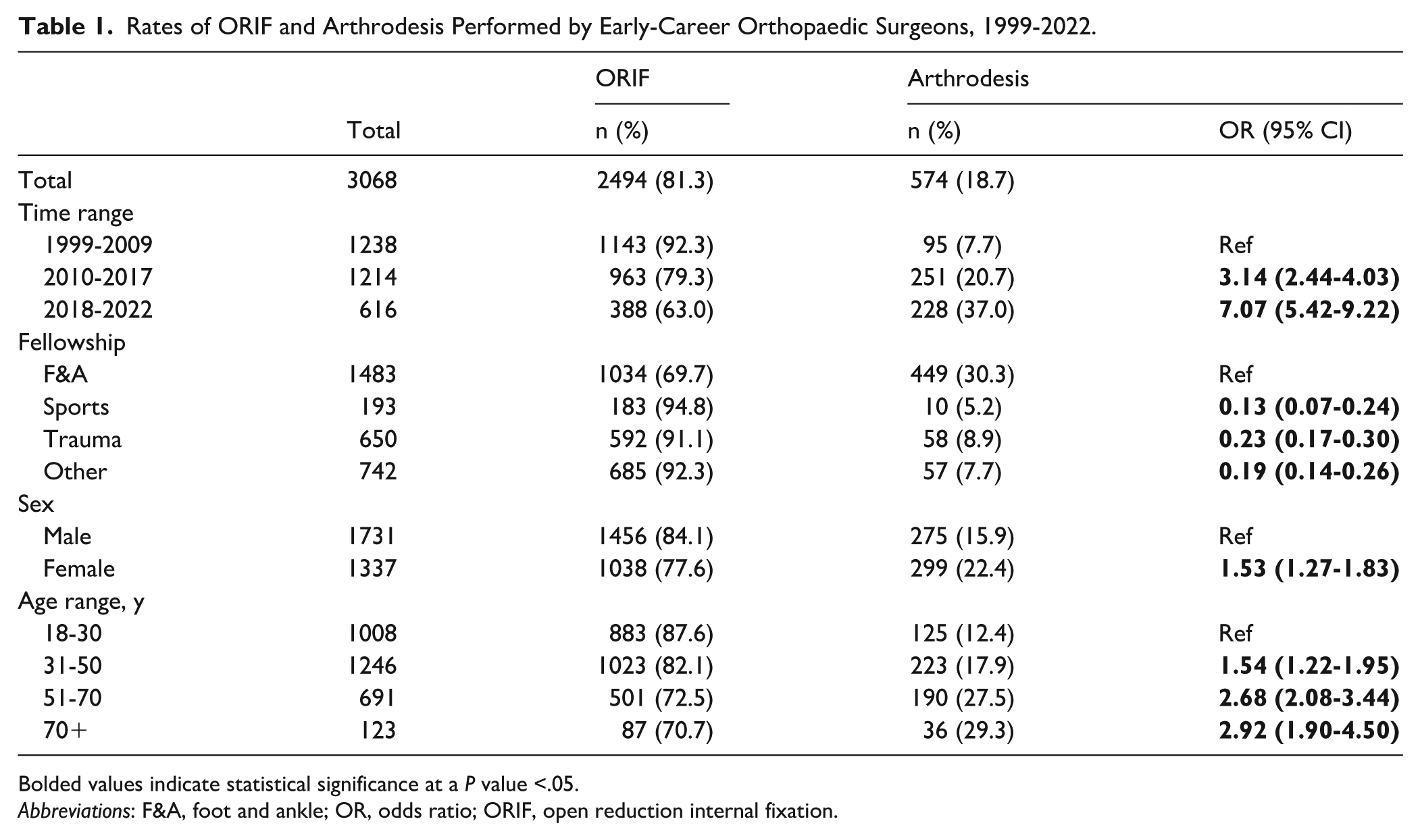
Bolded values indicate statistical significance at a P value <.05.
Abbreviations: F&A, foot and ankle; OR, odds ratio; ORIF, open reduction internal fixation.
There was an overall increasing rate in arthrodesis across this period (Figure 1). Beginning with 8.1% in 1999 (8/99), the rate dropped to 4.3% in 2002 (4/94) before reaching 42.8% in 2022 (62/145). On average, the likelihood of arthrodesis increased by a factor of 1.13, or 13%, each year between 1999 and 2022 (95% CI 1.11-1.15).

The rate of arthrodesis for Lisfranc injuries performed by early career orthopaedic surgeons relative to total cases by year, 1999-2022.
Among all patients, regardless of subspecialty, patient sex, and patient age, the rate of arthrodesis increased over time (Table 2, Figure 2). The rate of arthrodesis significantly increased across time periods, increasing from 7.7% in 1999-2009 (95/1238) to 20.7% in 2010-2017 (251/1214; P < .0001) and to 37.0% in 2018-2022 (228/616; P < .0001) (Table 3). The rate of arthrodesis significantly increased during the study period among foot and ankle, sports medicine, and trauma specialists. However, it did not increase in the “other” fellowship category. Similarly, the rate of arthrodesis significantly increased among both males and females and all age ranges during the study period (Table 3). A similar trend was observed in the ligamentous-only subgroup (Appendix B2 and B3). The rate of arthrodesis by patient sex did not differ across patient ages (P = .39).
Rates of ORIF and Arthrodesis within Time Periods.
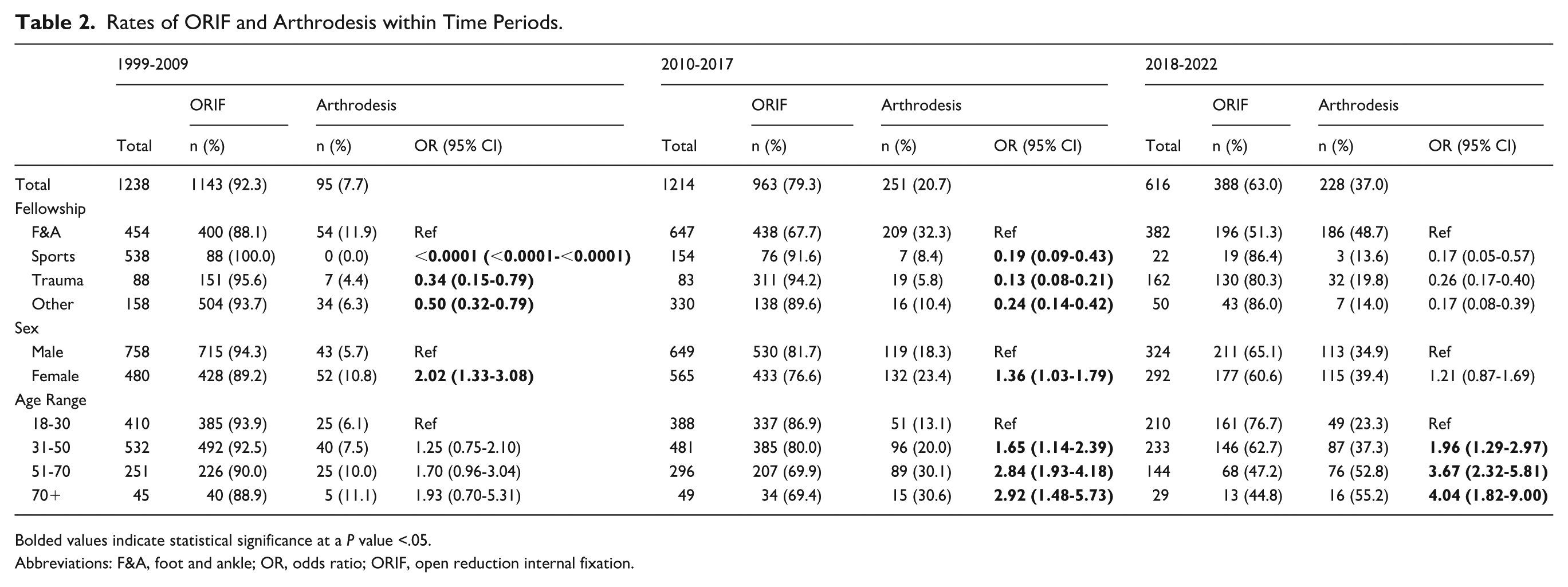
Bolded values indicate statistical significance at a P value <.05.
Abbreviations: F&A, foot and ankle; OR, odds ratio; ORIF, open reduction internal fixation.

Rates of arthrodesis performed by early career orthpaedic surgeons in total and by patient sex, age, and subspecialty across time periods. Bars denote 95% CIs. F&A, foot and ankle.
The Rate of Arthrodesis and 95% CIs in Total and by Fellowship, Patient Sex, and Age Range by Time Period.

Bolded values indicate statistical significance at a P value <.05.
Abbreviations: F&A, foot and ankle; OR: odds ratio.
Odds ratio of arthrodesis in 2010-2017 with 1999-2009 as reference.
Odds ratio of arthrodesis in 2018-2022 with 1999-2009 as reference.
Odds ratio of arthrodesis in 2018-2022 with 2010-2017 as reference.
Discussion
This study demonstrates a widespread shift toward arthrodesis for Lisfranc injuries among ABOS candidates, particularly among foot and ankle subspecialists. Despite this overall increase in arthrodesis, important differences persist across subspecialties, potentially reflecting varying interpretations of the supporting literature.
Analysis of the Shift in Literature Regarding Arthrodesis and ORIF
Since the Ly and Coetzee 7 RCT in 2006, several studies have compared arthrodesis and ORIF, incorporating additional strengths such as validated outcome scores and longer-term follow-up. A 32-patient RCT by Henning et al 26 found no difference in patient satisfaction or functional outcomes, although the study was underpowered. Hawkinson et al 9 found no difference in return to duty in military patients, but did not stratify based on injury pattern, fixation method, or reduction quality. Buda et al 10 found that, excluding planned hardware removal for ORIF, there were no differences in the reoperation rate or restoration of anatomic alignment in 217 patients.
Meanwhile, several studies have favored arthrodesis over ORIF. Factors hypothesized to contribute to this include high rates of symptomatic hardware, loss of reduction, and secondary arthrodesis following ORIF. Finite element analysis has demonstrated that arthrodesis provides more mechanical stability to the midfoot than ORIF. 27 Qiao et al 13 found that the American Orthopaedic Foot & Ankle Society hindfoot score was better in patients treated with arthrodesis in a retrospective cohort of 25 patients. Other studies have reported improved patient-reported outcomes with arthrodesis and high rates of symptomatic hardware and loss of reduction (28.5%-47%) with ORIF.14,15 Although many studies focused on purely ligamentous injuries, Sun et al 16 found that median arthrodesis outcome scores were also better in dislocations or fracture. Further, a systematic review determined that studies favoring arthrodesis were more statistically robust than those demonstrating equivalence between arthrodesis and ORIF outcomes. 25
Despite the growing evidence suggesting similar or superior outcomes of arthrodesis, few studies have assessed its influence on clinical practice. A previous study used ABOS Part II data and found no change in arthrodesis rate among only 2 CPT codes over a shorter study period, 2004-2017. 28 Since then, more studies have emerged showing favorable outcomes from arthrodesis. Thus, it is likely the full impact of this trend in literature had not yet been elucidated by 2017. Additionally, only 2 CPT codes were included: 28740 (single joint midtarsal or tarsometatarsal arthrodesis) and 28615 (open treatment, including fixation, of tarsometatarsal joint dislocation), while excluding all instances in which both were used. This likely undercounted the surgeries during the study and did not capture cases with multijoint fusions. The presented study captured a broader timeline of data (1999-2022) and included a more comprehensive list of CPT and ICD codes. This study observed a substantial increase in arthrodesis from 7.7% between 1999 and 2009 (95/1238) to 37% between 2018 and 2022 (228/616).
Lisfranc Treatment Variations by Fellowship Training, Patient Characteristics, Type of Injury, and Year
Despite an overall increase in arthrodesis among all subspecialties, there were important differences noted in the analysis. Foot and ankle specialists used arthrodesis significantly more than other subspecialists across all 3 time periods. By the third period, nearly half of all Lisfranc injuries managed by foot and ankle specialists were arthrodesis (186/382), compared with 19.8% by traumatologists (32/162) and 13.6% by sports medicine surgeons (3/22). This may reflect differences in training—including experience with arthrodesis techniques and exposure to current foot and ankle literature—as well as differences in patient populations and referral patterns, including more complex injuries that require arthrodesis being preferentially referred to foot and ankle specialists. It is unlikely that this trend was driven by a change in referral pattern alone, given the higher increase in arthrodesis rate for foot and ankle specialists over time. Additionally, given the historical preference for ORIF, more senior surgeons may favor this approach, influencing the practice patterns of residency graduates. Finally, not all residency programs offer dedicated foot and ankle rotations. A survey of orthopaedic residency graduates revealed that only 47.5% are comfortable independently performing arthrodesis of the foot.29,30 This may reflect the lack of fusion case minimums during residency. These findings may indicate a need for greater exposure to foot and ankle arthrodesis in orthopaedics training and dissemination of existing literature on arthrodesis vs ORIF in Lisfranc injuries.
This study observed significant growth in arthrodesis across patient sex and age groups. This is consistent with the literature suggesting favorable outcomes with arthrodesis across demographics. The higher rate of arthrodesis observed in female patients may be related to differences in bone density or injury pattern. Women have higher rates of osteoporosis and have been reported to sustain a greater proportion of lower-energy, ligamentous injuries; however, causality cannot be inferred from these data.31,32 Similar increases in arthrodesis were seen in both the narrow and broad cohorts. This suggests that both isolated ligamentous injuries and fracture-dislocations are increasingly treated with arthrodesis, aligning with RCT data for both types of injury. 16 With the emergence of additional literature supporting arthrodesis since the end of the study period,6,15,16,25,33 the rate of arthrodesis may continue to rise but will likely reach a plateau, as certain patients and injury patterns remain better treated with ORIF.
Notably, arthrodesis rates declined from 43% in 2019 (40/94) to 25% in 2020 (32/126), then rebounded to 37% in 2021 (53/145). However, the number of total cases remained stable over this period. In 2020, more Lisfranc injuries were managed by non–foot and ankle trained specialists than in adjacent years. It is possible that the overall decrease in elective case volume during the COVID-19 pandemic and disruption of referral patterns resulted in a lower arthrodesis rate, although it should be noted that many ABOS candidates deferred certification to the following year, which may also account for this anomaly.
Although this study demonstrates an increase in arthrodesis rate across 3 time periods corresponding with publication trends in the literature, additional factors may have contributed to this rise. One plausible explanation is the introduction and marketing of midfoot-specific compression systems and fusion plates, which have made fusion technically easier and more accessible, thereby lowering the threshold for adoption of arthrodesis. As such, although the data demonstrate a temporal association, a causal relationship between the literature and the increased use of arthrodesis cannot be definitively established.
Strengths and Weaknesses of this Study
Despite growing evidence favoring arthrodesis over ORIF, to the knowledge of the authors, no prior studies have shown a change in arthrodesis rate in clinical practice. The study analyzed 3068 surgically managed Lisfranc injuries in early-career orthopaedic surgeons over a 24-year period, demonstrating a consistent increase in arthrodesis rates across subspecialties, patient characteristics, and injury types. A key strength of the study is the use of data that are collected by the ABOS during the Board Examination Case List collection period. The findings add to the literature by providing epidemiologic evidence that arthrodesis is becoming a more common surgical management.
This study is not without limitations. The ABOS data are dependent on the accuracy and completeness of the recorded ICD and CPT codes to capture injury patterns and fixation methods. The chronicity of the injuries is not recorded. Delayed treatment or missed injuries may be more likely treated with arthrodesis than acute injuries, thus skewing the results. 34 Beyond the narrow and broad definitions of Lisfranc injury in the subgroup analysis, the Lisfranc injuries were unable to be additionally classified, although it has been shown that Myerson types A and C2 tend to have worse functional outcomes and may benefit from arthrodesis over ORIF. 15 Further, subspecialty data were not reported until 2002, which could bias the subspecialty data from the first time period (nearly all cases from 1999-2001 are categorized as “other”). Moreover, data from early-career orthopaedic surgeons likely do not generalize to all practicing surgeons. Data on patient race and ethnicity were not available, which may also affect the generalizability of the findings.
Finally, despite the growing evidence in favor of arthrodesis, long-term comparative outcomes remain limited. The ABOS database lacks long-term follow-up, limiting outcome analysis. These analyses also did not include data on complications and reoperation rates. Campbell et al 35 found worse outcomes after secondary arthrodesis for failed ORIF than after arthrodesis at 2-year follow-up. As such, there is a role for arthrodesis in the initial management of Lisfranc injuries in appropriately identified patients and injury patterns, whereas ORIF may be more suitable in other cases.
Conclusions and Implications
Although ORIF remains the more commonly performed fixation method for Lisfranc injuries among early-career orthopaedic surgeons, the use of arthrodesis increased over the 24-year study period. Among foot and ankle fellowship–trained surgeons, arthrodesis utilization has nearly equaled that of ORIF. Further investigation is warranted to assess long-term outcomes, complications, appropriate indications, and to better understand the underlying factors driving variation in arthrodesis adoption across subspecialties.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261433594 – Supplemental material for Trends in Surgical Management of Lisfranc Injuries: An Analysis of American Board of Orthopaedic Surgery Part II Candidates
Supplemental material, sj-pdf-1-fao-10.1177_24730114261433594 for Trends in Surgical Management of Lisfranc Injuries: An Analysis of American Board of Orthopaedic Surgery Part II Candidates by Kathryn R. Segal, Phillip Schmitt, Janine Molino, Amanda Galambas, Jonathan Liu, Brad Blankenhorn and Raymond Y. Hsu in Foot & Ankle Orthopaedics
Footnotes
Appendix A
Appendix B. Sub-group analyses using purely ligamentous Lisfranc injuries
The Rate of Arthrodesis for Ligamentous Lisfranc Injuries and 95% CIs in Total and by Fellowship, Patient Sex, and Age Range by Time Period.

| 1999-2009 | 2010-2017 | 2018-2022 | 2010-2017 vs |
2018-2022 vs |
2018-2022 vs |
|
|---|---|---|---|---|---|---|
| Rate (95% CI) | Rate (95% CI) | Rate (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Total | 7.0 (5.5-9.0) | 20.1 (17.5-22.9) | 37.2 (33.4-41.2) | |||
| Fellowship | ||||||
| F&A | 11.3 (7.2-17.3) | 32.4 (27.5-37.7) | 48.7 (42.7-54.7) |
|
|
|
| Sports | 0 (0-0) | 7.5 (3.2-16.4) | 13.6 (4.5-34.7) |
|
|
1.96 (0.42-9.07) |
| Trauma | 4.9 (1.8-12.3) | 5.4 (3.2-8.8) | 20.5 (14.9-27.6) | 1.10 (0.35-3.54) |
|
|
| Other | 5.4 (3.5-8.4) | 10.9 (6.7-17.3) | 14.0 (6.9-26.3) |
|
|
1.33 (0.50-3.51) |
| Sex | ||||||
| Male | 5.5 (3.8-7.9) | 16.7 (13.5-20.5) | 34.8 (29.8-40.2) |
|
|
|
| Female | 9.4 (6.7-13.2) | 23.5 (19.7-27.8) | 39.9 (34.3-45.7) |
|
|
|
| Age range | ||||||
| 18-30 | 4.2 (2.3-7.5) | 12.3 (8.9-16.7) | 23.7 (18.4-29.9) |
|
|
|
| 31-50 | 7.6 (5.3-10.9) | 19.9 (16.0-24.5) | 38.5 (32.4-45.0) |
|
|
|
| 51-70 | 9.3 (5.7-14.8) | 28.6 (22.8-35.3) | 51.8 (43.6-59.9) |
|
|
|
| 70+ | 11.8 (4.5-27.5) | 34.3 (20.6-51.2) | 53.6 (35.4-70.8) |
|
|
2.21 (0.79-6.21) |
Bolded values indicate statistical significance at a P value <.05.
Abbreviations: F&A, foot and ankle; OR, odds ratio.
Odds ratio of arthrodesis in 2010-2017 with 1999-2009 as reference.
Odds ratio of arthrodesis in 2018-2022 with 1999-2009 as reference.
Odds ratio of arthrodesis in 2018-2022 with 2010-2017 as reference.
Ethical Considerations
IRB approval was not required for this study as this project used deidentified, aggregate case-level data from the ABOS Part II Oral Examination Case List Database. The investigators had no means to reidentify individuals, and no interaction or intervention with human subjects occurred.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data Availability Statement
The data sets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.