
Abstract
Background:
Pickleball has emerged as the fastest-growing sport in the United States, with participation increasing nearly 1000% since 2019 and now surpassing 36 million players. Within the same period, tennis participation has risen by 33%. Pickleball’s rapid rise, accelerated by the COVID-19 pandemic, has paralleled anecdotal reports of musculoskeletal injury, yet little is known regarding Achilles tendon rupture (ATR) risk in this population. Tennis, a sport with similar biomechanics, has long been studied in relation to ATR, but comparative data for pickleball is lacking. The purpose of this study is to compare ATR proportional frequency sustained during pickleball, tennis, and all other sports to identify patterns of risk and inform athlete counseling.
Methods:
A retrospective review was conducted from January 2018 through December 2022 to identify patients who underwent Achilles tendon repairs within a large, independent orthopaedic group (>100 surgeons). Procedures were identified through the Current Procedural Terminology (CPT) code 27650. Patients aged 18-75 years with acute ATR who were treated operatively were included. Exclusion criteria were chronic tears requiring graft augmentation, revision procedures, failed nonoperative management, <2 months of follow-up, or incomplete clinical documentation. Mechanism of injury was recorded and categorized as pickleball, tennis, or other sports. A total of 1035 ATRs were identified and reviewed, with 1028 patients undergoing operative repair of an acute ATR. This included 942 other sports, 46 tennis, and 40 pickleball injuries. The primary outcome was the percentage of surgical volume of pickleball-related ATRs compared with tennis and other sports, stratified by age and year of injury. Secondary outcomes included major complications and minor complications. Data were analyzed using χ2/Fisher exact tests and Wilcoxon rank-sum tests.
Results:
Pickleball ATRs occurred in significantly older patients (median 60 years) compared with tennis (45 years) and other sports (37 years) (P < .0001). The sex distribution and comorbidities were similar across groups. BMI was lower in tennis and pickleball vs other sports (P = .0004). Age distribution demonstrated that 82.5% of pickleball ruptures occurred in patients >50 years vs 32.6% in tennis and 18.9% in other sports. Pickleball-related ATRs increased from 0.5% in 2018 to 6.7% in 2021. There was no difference in complication rates between patients with pickleball-related ATRs and all other sports (15.0% vs 15.7%).
Conclusion:
Pickleball-associated Achilles tendon ruptures represent a distinct demographic pattern, predominantly affecting adults >50 years of age, with a marked increase in cases following 2020, suggesting a correlation with the start of the COVID-19 pandemic. With the numbers available, no significant difference in postoperative complication rates was detected; however, the relatively small number of pickleball injuries limits statistical power and precludes definitive conclusions regarding comparative safety or injury patterns compared with tennis or other sports.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
Pickleball has emerged as the fastest-growing sport in the United States, with participation increasing nearly 1000% since 2019 and reaching approximately 36.5 million players by 2023. 1 Unlike most emerging sports, pickleball has attracted a predominantly older demographic, with an estimated 90% of emergency department visits for pickleball-related injuries occurring in players aged >50 years. 2 This rapid growth was accelerated by the COVID-19 pandemic, which led to a 158% increase in participation from 2020 to 2022—far exceeding the 33% growth rate observed in tennis during the same period. 3 Although musculoskeletal injuries associated with pickleball have been anecdotally reported, little is known about Achilles tendon rupture (ATR) patterns in this population.
Achilles tendon ruptures have an annual incidence of 5 to 50 per 100 000 persons and have typically been described in patients who are 30-40 years old, male, and involved in higher frequency of athletic activity. 4 Over the past 7 decades, the epidemiology of ATR has shifted, with a significant rise in mean patient age and a gradual increase in the proportion of female patients. 5 These demographic changes reflect broader trends in recreational sports participation across aging populations, yet the specific injury patterns associated with newer sports like pickleball remain poorly characterized.
Tennis, a racquet sport with biomechanical demands similar to pickleball, has been extensively studied in relation to ATR. Tennis-related ruptures account for 6.9% to 9.0% of all ATRs in some series, 6 typically occurring during explosive acceleration and sudden directional changes. However, comparative data examining whether pickleball produces similar or distinct injury patterns are lacking. Similar lower extremity biomechanical demands between these sports—both requiring rapid starts, stops, and lateral movements—suggest potential parallels in injury mechanisms. Yet, pickleball’s smaller court dimensions, underhand serve, and marketing appeal to older, less conditioned athletes may result in a fundamentally different risk profile.
The temporal correlation between the COVID-19 pandemic and both the surge in pickleball participation and observed increases in ATR percentage of surgical volume presents a unique opportunity to document this evolving injury pattern. Previous studies have demonstrated increased injury rates among elite athletes following the pandemic, 7 and preliminary evidence suggests similar trends in the general population. 8 However, no studies have specifically examined the intersection of pandemic-related activity changes, pickleball growth, and ATR relative case burden in older recreational athletes.
The purpose of this study was to compare demographic and temporal patterns of ATRs sustained during pickleball, tennis, and other sports activities within a large orthopaedic practice. We hypothesized that pickleball-related ATRs would occur in an older patient population compared with tennis and other sports, and that the proportional frequency of pickleball-related ATRs would increase significantly during the post-COVID period (2020-2022) compared with the pre-COVID baseline (2018-2019). Understanding these patterns is important for developing targeted prevention strategies and providing evidence-based counseling to the growing population of older athletes participating in pickleball.
Methods
A retrospective review was conducted within a large, independent orthopaedic group (>100 surgeons) for Achilles tendon repair from January 2018 through December 2022 using a query including the Current Procedural Terminology (CPT) code 27650 for the primary repair of Achilles tendon rupture. All patients aged 18-75 years who were diagnosed with an acute Achilles tendon rupture and underwent operative repair within the orthopaedic group were screened for inclusion. Patients were excluded from the study if they had chronic tears that required reconstruction with autograft or allograft augmentation, revision procedures, had attempted nonoperative management and failed, had less than 2 months of follow-up, or were missing important clinical documentation.
The primary outcome variable assessed was the percentage of surgical volume of Achilles tendon injury due to pickleball. The data regarding the mechanism of injury and age at the time of surgery were then stratified to determine the prevalence of pickleball-associated Achilles repairs based on patient age and its longitudinal association over the 5 years studied.
Secondary outcomes assessed included the development of major and minor complications. Major complications were defined as deep infection, rerupture, heel pain needing repeat operation, or other reoperation. Minor complications were defined as superficial infection, sural neuritis, delayed wound healing, heel pain, painful repair site, and repair laxity not requiring reoperation. A detailed analysis of overall complications was reported in a separate manuscript. 9
Data was collected and stored in an electronic research database (REDCap).10,11 Standard descriptive statistics were calculated and reported, including measures of central tendency (mean/median), variance (SD/IQR), as well as frequencies and proportions. Normality testing was performed for continuous variables via histograms and quantile-quantile plots. All continuous variables violated the normality assumptions, so medians and IQRs are presented. For bivariate analyses, χ2 or Fisher exact tests were used for categorical data (eg, complications between groups) to determine statistical differences. For continuous variables (eg, age), a Wilcoxon rank sum test was used to compare differences between groups. All data were analyzed using SAS, version 9.4 (SAS Institute). Funding for the study was internal and without commercial or industry support. No data safety monitoring was necessary given the retrospective nature of the study.
Results
A total of 1132 Achilles tendon procedures were identified using CPT code 27650 during the study period. After applying exclusion criteria, 1035 acute Achilles tendon ruptures in 1028 patients were included in the final analysis (Figure 1). Ninety-seven cases were excluded for the following reasons: age outside the 18-75-year range (n = 5), prior ipsilateral Achilles tendon rupture (n = 32), injury occurring outside the study dates (n = 44), and other reasons including incomplete documentation (n = 16). The median follow-up duration was 106 days (IQR, 77-176 days).

CONSORT Flow Diagram.
Of the 1035 ATRs, 40 (3.9%) were sustained during pickleball, 46 (4.4%) during tennis, and 949 (91.7%) during other activities. Basketball was the most common mechanism of injury overall, representing 355 cases (34.3%), followed by trip/fall (141 cases, 13.6%), and soccer (76 cases, 7.3%) (Table 2). When all racquet sports were combined, they represented the third leading mechanism for surgically treated ATRs, accounting for 93 cases (9.0%).
Demographics and Patient Characteristics
Patient age differed significantly across injury mechanisms (Table 1). The median age of patients with pickleball-related ATRs was 60 years (IQR, 51.5-65), which was significantly higher than patients with tennis-related ATRs (44.5 years; IQR, 39-54) and patients with all other injury mechanisms (37 years; IQR, 30-47) (P < .0001).
Demographic Data.

Abbreviations: BMI, body mass index; IS, immunosuppressants; RA, rheumatoid arthritis.
Mechanism of Injury.

The sex distribution was similar across groups, with 83% of patients being male overall. Males represented 77.5% of pickleball injuries, 71.7% of tennis injuries, and 83.8% of other sport injuries (P = .0683). Body mass index (BMI) was lower in both racquet sport groups compared to other sports. The median BMI for pickleball patients was 26.1 (IQR, 24.6-28.7), for tennis patients was 25.8 (IQR, 24.2-29.3), and for other sports was 28.2 (IQR, 25.3-32.1) (P = .0004).
There were no significant differences in rates of diabetes, autoimmune disease, or smoking status between pickleball and non-pickleball cohorts (Table 1).
Age Distribution Analysis
The age distribution of ATRs demonstrated markedly different patterns by injury mechanism (Figure 2, Table 3). Among pickleball-related ruptures, 82.5% occurred in patients older than 50 years, with the highest percentage of surgical volume in the ≥60-year age group (45.0%, 18/40) and the 51-60-year age group (37.5%, 15/40). Only 5.0% (2/40) of pickleball injuries occurred in patients aged 40 years or younger. Notably there is a monotonic increase in ATR relative case burden with age in the oldest 4 cohorts (Figure 2).

Percent Achilles Injuiries by Age
Mechanisms of Achilles Rupture by Age Stratification.

Abbreviation: HIIT, High-Intensity Interval Training.
In contrast, tennis-related ATRs showed a distribution with peak percentage of surgical volume in the 31-40-year age group (23.9%, 11/46) and 41-50-year age group (34.8%, 16/46). Overall, 58.7% of tennis injuries occurred in patients aged 31-50 years, whereas 32.6% occurred in patients older than 50 years.
Other sport-related ATRs occurred predominantly in younger patients, with 61.2% occurring in patients aged 18-40 years. Basketball, the most common injury mechanism overall, demonstrated 47.2% of injuries in the 18-30 age group and 46.2% in the 31-40 age group, with only 3.1% occurring in patients over 60 years.
Temporal Trends
The proportion of pickleball-related ATRs increased significantly over the study period (P = .0012, Figure 3). In 2018, pickleball accounted for 0.5% of all Achilles repairs (1 case). This increased to 1.9% in 2019 (4 cases), 6.5% in 2020 (10 cases), and peaked at 6.7% in 2021 (15 cases), before declining slightly to 4.0% in 2022 (10 cases).
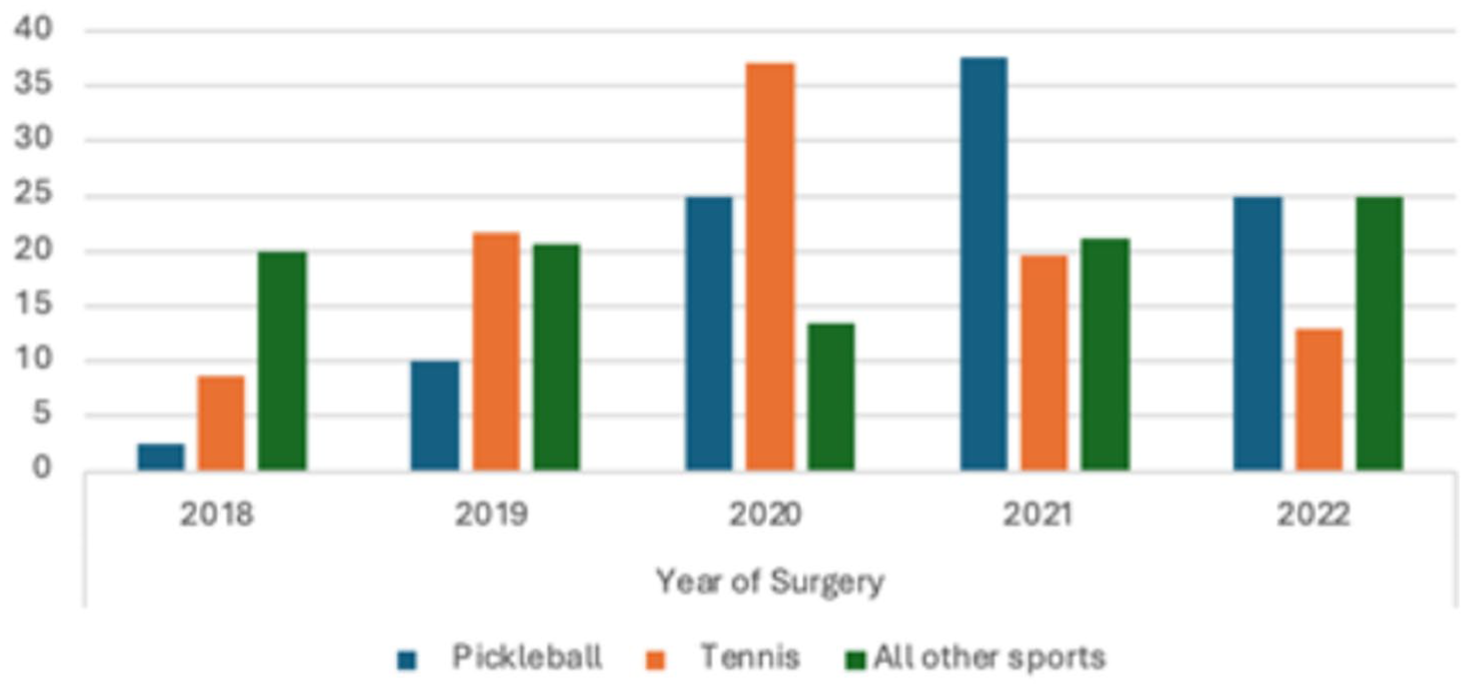
Percent Achilles Ruptures due to Pickleball vs Tennis vs All Other Sports by Year
When comparing pre-COVID (2018-2019) to post-COVID (2020-2022) periods, pickleball-related ATRs increased significantly from 1.2% (5/404) to 5.5% (35/631) of all cases (P = .0005). During this same period, tennis-related ATRs remained relatively stable, accounting for 4.4% (14/404) pre-COVID and 4.5% (32/631) post-COVID (P = .2213).
Surgical Treatment
The distribution of surgical techniques did not differ significantly between pickleball and non-pickleball injuries. Among pickleball cases, 57.5% underwent open repair, 37.5% underwent percutaneous repair (PARS), and 5.0% underwent suture anchor augmentation. This was comparable to the non-pickleball cohort: 55.8% open, 33.0% percutaneous, and 11.3% suture anchor (P = .4436).
Discussion
This study represents the largest series examining mechanism-specific ATR patterns and the first to characterize pickleball-related Achilles ruptures in detail. By analyzing more than 1000 consecutive ATR repairs across a large, heterogeneous surgical practice, it provides robust insights on real-world injury patterns. The study period captures a unique moment, where the exponential growth of the sport of pickleball correlates with the COVID-19 pandemic.
Our findings document the emergence of pickleball as a significant cause of Achilles tendon ruptures in older recreational athletes, with an increased proportional frequency by age decile. Prior literature has reported an epidemiologic shift toward older age and higher proportion of female patients sustaining ATRs. 5 Erickson et al 12 described the increasing prevalence of ATRs in the United States Medicare population, from 0.67 per 10 000 in 2005 to 1.08 per 10 000 in 2011 (P < .01). Current data confirm that older patients are engaging in high-impact activities. Forrester 2 showed an 800% growth in annual incidence of pickleball-related injuries between 2013 and 2017; additionally in 2020, 90% of emergency department visits for these injuries occurred in players older than 50 years. The present study supports these trends, demonstrating that patients who sustained an ATR and underwent subsequent repair secondary to playing pickleball were significantly older (60 vs 37 years, P < .0001) than the general cohort. The 13-fold increase in pickleball-related ATRs from 2018 to 2021 parallels the sport’s rapid growth and suggests an emerging public health concern as millions of older Americans adopt the game.
Three key findings emerged. Pickleball-related ATRs occurred in a significantly older population (median age 60 years) compared with tennis (median 44.5 years) and all other sports (median 37 years). Additionally, the age distribution was strikingly different: 82.5% of pickleball ruptures occurring in patients older than 50 years, compared with 32.6% for tennis and 18.9% for all other sports. Furthermore, the relative case burden of ATR repair increased by decade, suggesting a graded risk of injury. Pickleball-related ATRs rose sharply after COVID, increasing from 1.2% of all cases prepandemic to 5.0% postpandemic. Despite the older age of pickleball patients, complication rates were similar to younger cohorts (15.0% vs 15.7%, P = .91), suggesting that age alone should not preclude surgical management in appropriately selected patients.
Larsson et al 6 previously described the prevalence of acute Achilles ruptures related to other racquet sports including tennis (6.9%-9.0%) and badminton (3.0%-8.7%). Despite tennis and pickleball sharing similar biomechanical demands, their ATR age patterns differ sharply, with pickleball ruptures occurring nearly 2 decades later. Pickleball’s accessibility attracts a different demographic: players who may perceive the sport as “easier than tennis” because of its smaller court and lighter paddle. This allows individuals whose tendons have undergone age-related degenerative changes—including decreased collagen crosslinking, reduced vascularity, and diminished tensile strength 13 —to engage in high-intensity explosive activity without recognizing their increased injury risk. The smaller court may also enable play despite reduced fitness levels, inadvertently exposing aging tendons to loads they cannot safely tolerate.
Participation patterns further highlight these demographic differences. Tennis players often reduce or cease high-intensity play as physical limitations emerge, reflected by the younger distribution of tennis-related ATRs (58.7% in patients aged 31-50 years; 32.6% aged >50 years). In contrast, pickleball attracts individuals who have aged out of traditional high-risk sports but still seek competitive activity. The peak percentage of surgical volume of pickleball ATRs in patients older than 50 years (82.5%) represents a novel injury pattern in sports medicine—a cohort sustaining explosive movement injuries at an age when most athletes have transitioned to lower-impact activities. This sporadic high-intensity activity pattern, combined with age-related tendon changes, creates conducive conditions for rupture. The “weekend warrior” phenomenon may be particularly pronounced in the older group, which represent 52% of pickleball players compared with other age cohorts. 14
The temporal correlation between COVID-19 and the rise in pickleball-related ATRs is striking and likely multifactorial. Social distancing requirements shifted recreational activity toward outdoor, low-equipment sports such as pickleball, and its suitability for socially distanced doubles increased participation. Simultaneously, prolonged inactivity during lockdowns may have led to widespread deconditioning, particularly among older adults who experienced the longest periods of restricted activity. When these deconditioned individuals resumed or initiated high-intensity recreational activity, injury rates increased.
The predominance of pickleball ATRs in patients >60 years old highlights the biological vulnerability of aging tendons. Freedman et al 13 demonstrated that aging significantly affects tendon viscoelasticity, collagen organization, and cellular function, with measurable changes accelerating after age 50 years. These structural changes reduce the tendon’s ability to absorb energy during eccentric loading, increasing rupture susceptibility during the explosive movements required in pickleball. Furthermore, older athletes may face compounding risk factors, such as reduced proprioception, slower reaction times, and medication use.15-17 The combination of intrinsic tissue degeneration and extrinsic risk factors creates a particularly vulnerable population.
These findings have important clinical implications. The 60-year-old pickleball player represents a new injury archetype requiring age-specific counseling and prevention strategies. Orthopaedic surgeons should be aware that pickleball is increasingly attracting older athletes who may not have the conditioning or tendon resilience of younger populations. Counseling patients on the risks of ATR, as well as emphasizing preventive strategies such as structured warm-ups, eccentric calf strengthening, and appropriate footwear, may help mitigate the risks. For surgeons, anticipating that pickleball will remain a contributor to ATR in the coming years can help prepare practices for a shift in the age distribution of operative Achilles rupture cases.
Several limitations warrant consideration. The retrospective design limits causal inference and introduces potential for selection bias. In addition, possible indication bias should be acknowledged. The pickleball demographic analyzed in this study is clinically filtered in pursuit of operative management; therefore, the patient cohort may be healthier, more active, or have higher functional demands than the broader population of older adults who sustain similar injuries but are managed nonoperatively. Another limitation was the nonstandard duration of follow-up and the short minimum follow-up (2 months). Patient-reported outcomes scores were inconsistently collected and thus not reported, preventing analysis of functional recovery or return to sport. It is, therefore, challenging to correlate outcome scores with long-term function outcomes comparing patients within the pickleball cohort to the general cohort. This study raises important questions for future investigation. Prospective cohort studies should track pickleball participants over time to calculate accurate injury rates and identify modifiable risk factors. Additionally, collaboration with pickleball governing bodies (USA Pickleball) could facilitate large-scale injury surveillance and implementation of evidence-based safety guidelines for older players.
Conclusion
Pickleball-associated Achilles tendon ruptures represent a distinct demographic pattern, predominantly affecting adults aged >50 years. The dramatic increase in cases mirrors the sport’s growth during COVID and underscores the vulnerability of aging tendons. However, no significant difference in postoperative complications of Achilles tendon repairs following pickleball injuries was detected compared to ruptures sustained in other sports. The small pickleball sample size (n = 40) limits statistical power to confirm significant differences in postoperative complication rates when compared with Achilles tendon ruptures sustained during other sports. Consequently, these findings should be interpreted cautiously and should not be construed as definitive evidence of equivalent surgical safety. Larger prospective studies are needed to more accurately characterize outcomes and inform evidence-based counseling and prevention strategies for older pickleball players.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261425665 – Supplemental material for Pickleball-Associated Achilles Tendon Ruptures: Shifting Achilles Repair Demographics
Supplemental material, sj-pdf-1-fao-10.1177_24730114261425665 for Pickleball-Associated Achilles Tendon Ruptures: Shifting Achilles Repair Demographics by James H. Padley, Benjamin Averkamp, Madeline Rieker, Tyler Kalbac, Christopher D. Murawski, James A. Lendrum, Justin Rennard, Andrew Rees, Kayla Hietpas, Carroll P. Jones, Todd A. Irwin, Scott B. Shawen, J. Kent Ellington and Samuel E. Ford in Foot & Ankle Orthopaedics
Footnotes
ORCID iDs
Ethical Considerations
Ethical approval for this study was obtained from the Wake Forest Institutional Review Board (IRB00103568).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.