
Abstract
Background:
Hindfoot varus deformity is often corrected using lateral sliding calcaneal osteotomies, which may compress the tarsal tunnel and risk tibial nerve entrapment. Minimally invasive surgery (MIS) techniques may mitigate soft tissue disruption, but their impact on tarsal tunnel biomechanics remains unclear. Purpose is to evaluate the effect of calcaneal lateralization using a 3-mm MIS burr on tarsal tunnel volume and pressure in a cadaveric model.
Methods:
Ten matched pairs of fresh frozen cadaveric lower limbs underwent lateral-to-medial calcaneal osteotomy using a 3-mm MIS burr. Computed tomography (CT) scans measured tarsal tunnel volume pre- and post-osteotomy. Intra-compartmental pressure within the tarsal tunnel was assessed using an ultrasound-guided pressure monitor. Volumes were calculated using CT-derived cross-sectional reconstructions, and pressures were compared before and after lateralization.
Results:
Calcaneal lateralization led to significantly decreased tarsal tunnel volume (mean Δ = −3.06 ± 1.50 cm³, P < .0001) and significantly increased tunnel pressure (mean Δ = +11.18 ± 6.19 mm Hg, P < .0001). There was a significant inverse relationship between lateralization distance and volume change (R2 = 0.184, P < .0001), and a direct relationship between lateralization and pressure increase (R2 = 0.129, P = .026). Percentage volume change was negatively correlated with percentage pressure change (R2 = 0.042, P = .009). The average lateralization achieved was 6.33 mm.
Conclusion:
MIS calcaneal lateralization significantly reduces tarsal tunnel volume and increases intratunnel pressure, which may theoretically contribute to tibial nerve compression. However, the magnitude of pressure increase observed was generally below levels associated with neural dysfunction. Although MIS approaches offer soft tissue advantages, this study suggests that tarsal tunnel decompression and flexor retinaculum release may still be warranted if symptoms develop postoperatively. In cases where greater lateralization is required, the flexor retinaculum release performed during a tarsal tunnel decompression allows for greater translation without the concomitant rise in tarsal tunnel pressure.
Clinical Relevance:
This model demonstrates the volume and pressure changes and lateralization distance that occur during an MIS lateral slide calcaneal osteotomy.
Introduction
Hindfoot varus deformity is a common anatomical deformity associated with muscular imbalance due to neurologic, traumatic, congenital, or idiopathic origin. Patients may present with pain, instability, lateral column overload, and recurrent sprains. Symptoms can progress if left untreated. 1 The current treatment for hindfoot varus deformity correction is the open lateral sliding calcaneus osteotomy or variations used to move the posterior tuberosity laterally. However, complications associated with open techniques for hindfoot varus correction include sural nerve damage, wound complications, and non-union. 2 Additionally, the process of the lateral slide tightens the flexor retinaculum, and contents in the tarsal tunnel including the tibial nerve, posterior tibial artery, and posterior tibial vein may become compressed. 2 Whether or not the compression leads to symptomatic damage to the contents of the tarsal tunnel is a controversial topic. Some surgeons believe that excessive lateralization can lead to overtightening of the tarsal tunnel and compression of the tibial nerve, leading to tarsal tunnel syndrome. Symptoms include numbness and tingling in the lateral and medial plantar nerve distribution. These have been reported to occur with 30.0 mm Hg of pressure; however, it is also dependent on the location of compression and duration of compression. 3 Although the literature on tarsal tunnel syndrome after lateral sliding calcaneal osteotomies is sparse, studies have reported incidences anywhere between 0% and 34% and can vary based on surgical approach, osteotomy technique, and amount of lateralization achieved.4 -6
Some surgeons advocate for prophylactic tarsal tunnel release before performing lateral slide osteotomies with a standard saw. 7 However, this is not a benign procedure and is not the current standard of care no matter the size of the translation. Previous cadaver studies have investigated tarsal tunnel volume changes with standard saw calcaneal osteotomies. 8 There exists no such recommendations for similar osteotomies performed with a 3-mm minimally invasive (MIS) burr. Advocates against performing a prophylactic tarsal tunnel decompression state that the burr removes more bone than a saw and, therefore, the pressure does not increase enough to lead to a tarsal tunnel syndrome. 9 Further understanding of how tarsal tunnel pressure and volume are affected by MIS burr lateral sliding calcaneal osteotomies is necessary in order to determine if tarsal tunnel decompression is necessary with this technique.
The objective of this study was to assess the effect of the lateral sliding calcaneal osteotomy on the change in tarsal tunnel volume and pressure produced via lateral sliding osteotomy using MIS burr. We hypothesize that lateralization of the calcaneus will decrease the volumes in the tarsal tunnel and increase the pressures in the tarsal tunnel. Secondarily, we hypothesize that there will be an inverse relationship between distance of lateralization and volume decrease and a direct relationship between distance of lateralization and pressure increase. This will provide insight into the risk of tarsal tunnel syndrome posed when performing a lateral sliding osteotomy using MIS burr.
Methods
Ten pairs of fresh frozen cadaver below-knee specimens (minimum 6 inches proximal to the ankle) were obtained and thawed to room-temperature overnight. IRB approval and informed consent was neither necessary nor obtained for this study given its cadaveric in nature. The lateral-slide osteotomies were performed by 2 Foot and Ankle fellowship–trained orthopaedic surgeons. Ultrasound-guided tarsal tunnel pressure values were measured by a single fellowship-trained Sports Medicine physician, who has significant experience in bedside ultrasound-guided procedures.
Single-plane, lateral-to-medial MIS burr calcaneal osteotomies were performed using a 1-cm lateral approach. A 3 × 20-mm saline cooled, Shannon burr was used for all procedures. A new burr was used for each cadaver. The osteotomies were performed under fluoroscopic guidance in the safe zone as described by Ramsingh et al 10 (Figure 1A). After the osteotomy was completed, the posterior tuberosity was translated laterally by placing a joker elevator into the posterior tuberosity from the lateral incision and pushing the tuberosity laterally. As much force as possible was used to move the tuberosity as far as possible. This is the technique that both attendings perform in clinical practice. Two guidewires were used to maintain lateralization, and then two 6.5-mm cannulated screws were inserted from posterior to anterior along the guidewire trajectories for definitive fixation. Following completion of this procedure, the postoperative tarsal tunnel volumes were subsequently recorded as described above at maximum calcaneal lateralization.

(A) Experimental photo of the calcaneal lateralization osteotomy being performed on cadaver feet. (B) Ultrasonographic image of the pressure probe being placed in the tarsal tunnel.
Tarsal tunnel pressures were measured before and after the osteotomy using a single-needle barometer commonly used by orthopaedic surgeons in practice to evaluate musculoskeletal compartment pressures (STIC Pressure Monitor; C2Dx). The barometer was connected to an 18-gauge needle that was placed into the tarsal tunnel and inserted under ultrasound guidance similar to the technique developed by Trepman et al. 11 The barometer was calibrated to 0 mm Hg at room pressure in close proximity to the foot before each separate series of volume measurements. The tip of the needle was placed 2-3 cm distal to the anterior edge of the flexor retinaculum and confirmed to be in the tarsal tunnel via ultrasound (Figure 1B). The needle was then sutured in place to record the pressures in the same relative location within the tarsal tunnel following the osteotomy. In instances where the needle slightly migrated from the target position, the needle was repositioned under ultrasound guidance. The pressure was measured postoperatively at a single time point immediately after osteotomy and screw placement. All pressure measurements were taken with the foot and ankle in a neutral position, as this position was deemed the most clinically significant because postoperative protocol involved splinting the foot and ankle in a neutral position in a short leg splint immediately after surgery. The barometer takes approximately 1 minute for the pressures to stabilize and provide a final reading. Tarsal tunnel pressures were obtained as an average of 3 separate readings with each specimen.
A standard CT scan without contrast was performed on each cadaver pre- and post-osteotomy to evaluate for the change in tarsal tunnel volume and measuring the amount of lateralization. The CT protocol used a slice thickness and interval thickness of 1 mm. All images were taken with the feet in neutral position and the ankles dorsiflexed to 90 degrees, simulating the position the extremities would be splinted in immediately postoperatively. Lateralization was measured on axial CT, as this plane is most similar to the fluoroscopy plane used to measure lateralization intraoperatively. The slice with the largest magnitude of lateralization was used for analysis (Figure 2).
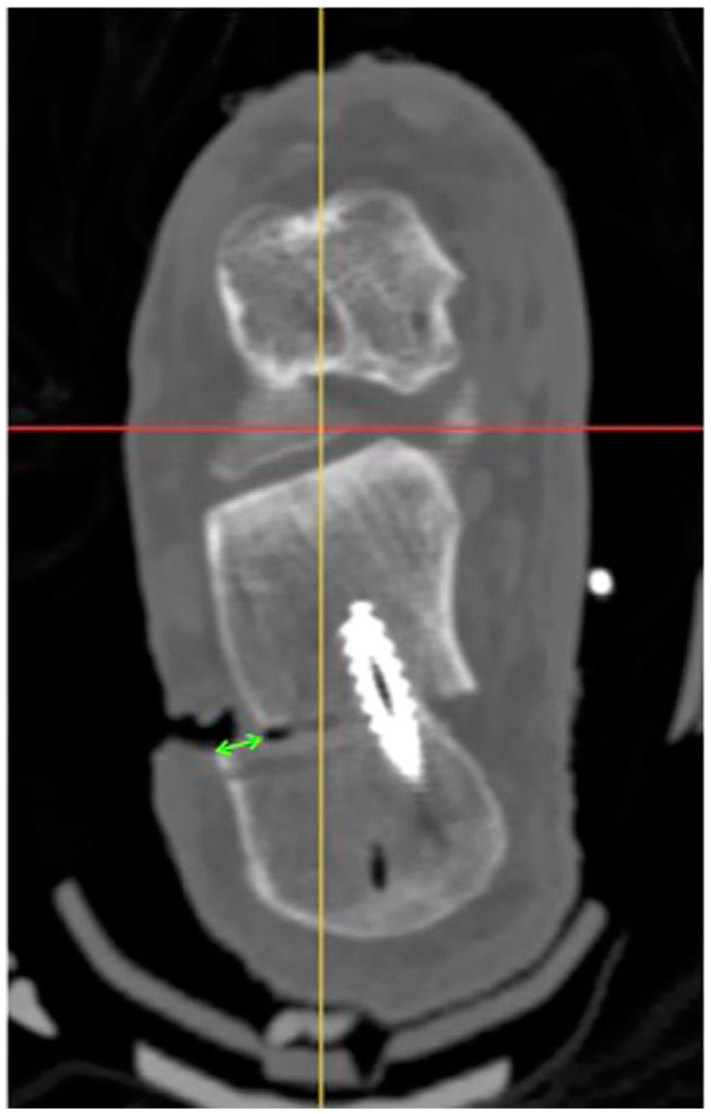
Axial computed tomographic image of a cadaveric ankle at the level of the maximum lateralization. Lateralization was measured along the lateral edge of the calcaneus as seen in the figure (green arrow).
Preoperative and postoperative tarsal tunnel volumes were measured using the techniques described by Bracilovic et al 12 and Stødle et al. 5 Briefly, cross-sectional views of the tarsal tunnel were calculated using an oblique ankle-hindfoot CT reconstruction plane. Using the bone and soft tissue windows, the tarsal tunnel was traced and defined as the medial border of the calcaneus, and the flexor retinaculum. The quadratus plantae muscle was included within the tarsal tunnel (Figure 2). The center of the tarsal tunnel was defined as the most anterior aspect of the posterior facet of the subtalar joint in the sagittal plane. To cover the same tarsal tunnel distance as Bracilovic et al and Stødle et al using our institution’s CT parameters (1-mm thickness and interspace), an additional cross-sectional area was measured both proximally and distally. After each measurement, the CT was advanced by 3 images, creating a net 5-mm distance between cross-sectional areas. To obtain volumes, each area was multiplied by 1 mm (slice thickness). The interspace volumes between each cross-section was calculated by taking the average of the 2 consecutive areas multiplied by the total interspace thickness between each measured image (5 mm). After advancing the CT through the entirety of the tarsal tunnel, the 9 slice volumes and 8 interspace volumes were summed to obtain the final volume.
All quantitative data are reported as mean ± SD. Pre- and postprocedure pressure values were analyzed using a 2-tailed Student t test. Statistical tests used the assumption of normality determining the utility of parametric or nonparametric test(s) of analyses, which, in turn, test for differences of significance and measure the strength and direction of relationship between continuous variables of interest, respectively. A P value of .05 was considered statistically significant.
Results
Lateralization
On our cadaveric specimens, we achieved an average lateralization of 6.33 ± 1.03 mm when performing the MIS burr calcaneal osteotomies.
Tarsal Tunnel Pressure
Tarsal tunnel pressures were measured preoperatively and postoperatively. Lateralization of the calcaneus resulted in a significant increase in tarsal tunnel pressures with a mean difference of 11.18 ± 6.19 mm Hg (P < .0001). The mean tarsal tunnel pressure postoperatively was 14.68 ± 6.13 mm Hg. There were only 2 measurements of the 60 completed measurements that exceeded 30 mm Hg.
Tarsal Tunnel Volume
Tarsal tunnel volumes were measured preoperatively and postoperatively via CT. The average preoperative volume was 19.87 ± 41.03 cm3. Lateralization of the calcaneus resulted in a significant decrease in tarsal tunnel volumes with a mean change of −3.07 ± 1.50 cm3 (P < .0001). This is equivalent to an average of 16.50% volume reduction.
Distance of Lateralization and Percentage Change in Volume
When examining the relationship between distance of lateralization and percentage change in volume, there was a significant direct relationship (R 2 = 0.184, P < .0001) (Figure 3).
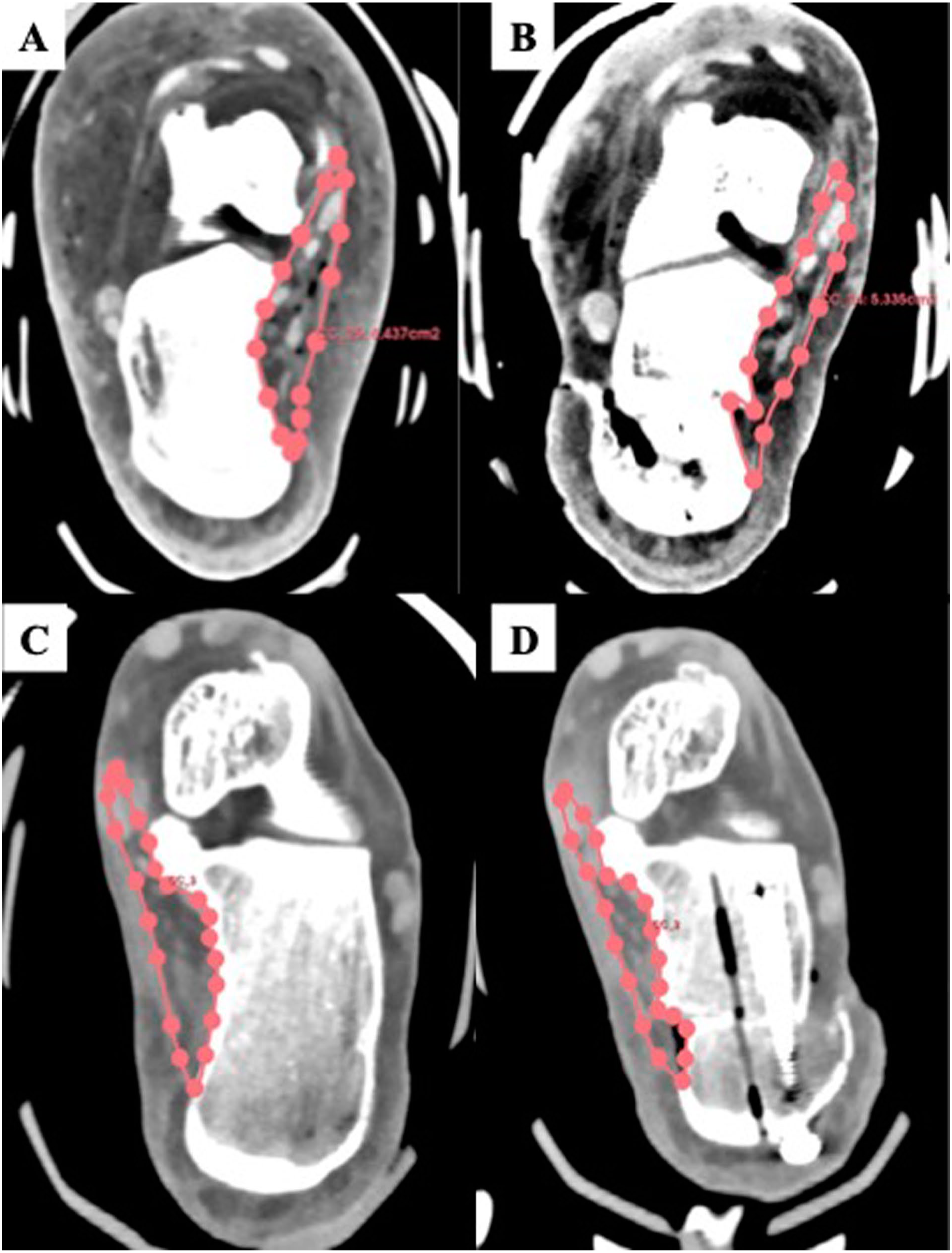
Axial computed tomographic images of the cadaveric ankles before (A and C) and after (B and D) calcaneal lateralization. The pink areas demonstrate the tarsal tunnel volumes that were calculated pre- and postoperatively.
Pre- and Postoperative Pressure and Volume
When examining the relationship between preoperative pressure and volume, there was found to be a significant correlation (R2 = 0.039, P < .0001) (Figure 4A). When examining the relationship between postoperative pressure and volume, there was found to be a significant correlation (R2 = 0.127, P < .0001) (Figure 4B). Because all pressure measurements were completed in triplicates, Figure 5 depicts the maximum postoperative pressure for each cadaver relative to its volume.

Graph depicting the linear relationship between the distance of lateralization and the percentage change in volume.

Graphs depicting the pressure-volume relationship in the tarsal tunnel both preoperatively (A) and postoperatively (B). Pressure values depicted here are an average of the triplicate measurements.
Discussion
Calcaneal lateralization using an MIS burr significantly changes the volume and pressure in the tarsal tunnel with statistically significant but relatively modest absolute increases in intratunnel pressure. This cadaveric study found that there was a significant decrease in tarsal tunnel volume and increase in pressure following the procedure, as expected by our hypothesis. The tarsal tunnel, found on the medial aspect of the hindfoot, is affected by the lateral shift of the calcaneus, closing down the space contained by the flexor retinaculum. As expected, when the volume of this space decreases, the pressure within that space increases, as proven by this study. The lack of a perfectly direct relationship is likely due to the elasticity and anatomy of human tissue. We also found a relationship between degree of lateralization and increased tarsal tunnel pressures, which must be considered when deciding if flexor retinaculum release might be beneficial concurrently with the osteotomy.
With increased pressure around the tibial nerve, abnormal neural function may occur, leading to symptoms associated with that of tarsal tunnel syndrome. This would include pain in the tibial nerve distribution about the plantar aspect of the foot, numbness, tingling, or a burning sensation on the bottom of the foot. This has proven to occur when there is a compression of the tibial nerve, which may occur with increased pressure within the tarsal tunnel.6,13 Symptoms of tibial nerve compression have been reported to occur with 30.0 mm Hg of pressure; however, it is also dependent on the location of compression and duration of compression. 3 Temporary nerve compression at these pressures are unlikely to cause persistent nerve dysfunction. Acute nerve function loss has been reported to occur between 40 and 50 mm Hg of pressure, and pressures above 60-80 mm Hg can cause irreversible damage.14 -16 There are other possible causes of tibial nerve pathology postoperatively that should be considered, such as iatrogenic injury or traction neuropraxia. In our study, 2 measurements had pressure readings above 30 mm Hg with an average much lower than that concerning for nerve damage (Figure 6). Despite the minimally invasive nature of our technique, the increased pressure of calcaneal lateralization still has theoretical potential to cause nerve irritation within the tarsal tunnel.

Graph depicting the relationship between the maximum measured postoperative pressure and postoperative volume. Greater than 30.00 mm Hg (orange shading) indicates a theoretical concern for tarsal tunnel symptoms to occur.
Other studies have analyzed the pressures in the tarsal tunnel before and after release. Iborra Marcos et al 17 performed a study in those with tarsal tunnel syndrome that measured tarsal tunnel pressures before and after decompression. They found that release of the tarsal tunnel significantly decreased tarsal tunnel pressures and improved patients’ symptoms, thus validating that pressure is an effective measurement tool in predicting tarsal tunnel syndrome. 17
It has been known that lateral slide calcaneal osteotomy, regardless of standard transverse technique or Malerba Z-type osteotomy, increases tarsal tunnel pressures and decreases volume, which is why some argue for prophylactic flexor retinaculum release during this procedure.2,8 Siddiqui et al 9 directly measured the tarsal tunnel pressures when performing calcaneal lateralization using a Shannon burr vs oscillating saw. They found that both techniques increase tarsal pressures, which substantiates our study; however, they also found that the oscillating saw produced significantly higher pressures than the Shannon burr. 9 Despite these risks of increased tarsal tunnel pressures, it is known that minimally invasive techniques provide a safer alternative to neurovascular structures during calcaneal osteotomies relative to other open techniques.18,19 One study by Kendal et al 19 demonstrated that MIS calcaneal osteotomies had significantly lower complications compared to an open technique when using a lateral approach. Another study by Durston et al 18 analyzed the risk of neurovascular injury using a minimally invasive Shannon burr, which was shown to minimize surgical morbidity and maximize surgical efficiency. Contrarily, using a burr may also cause unintended side effects such as heat necrosis, further damaging surrounding bone. However, it was found that these effects are likely similar to that of a saw. 20
Changes in the mechanics of the tarsal tunnel may also cause problems with the vasculature that runs through this space. The patency of the vasculature is dependent on the difference between the internal pressure and the external pressure from the surrounding compartment. 21 Therefore, this patency is positional, and dependent on an individual being supine versus standing. Regardless, there is a theoretical concern that increased tarsal tunnel pressures could cause venous occlusion and subsequent stasis. It is estimated that occlusion could occur with pressures greater than 25 mm Hg in a supine position, greater than 50 mm Hg in a sitting position, or greater than 70 mm Hg in a standing position. 21 In an extreme situation, there could be concern for arterial occlusion, but this is unlikely as compartment pressures would need to exceed >100 mm Hg. 22 The maximum postoperative pressure that we observed in this study was 30 mm Hg, posing no risk to arterial occlusion.
Although this study suggests that MIS techniques may still not be benign in preventing all morbidity following calcaneal osteotomies, it is limited mainly in its cadaveric nature. First, we do not know the status of the cadaver foot, whether it has subtle cavus, neutral or valgus foot deformities. We opted for a neutral position when performing the procedure, but cannot with certainty know the eventual weightbearing positions on loading. Additionally, the stiffened soft tissues may limit the lateral slide distance and thus the effect on pressure. We had an average calcaneal slide of 6.33 mm, a relatively small translation. Surgeons should consider the benefit of flexor retinaculum release on ease for larger translation in addition to avoidance of tarsal tunnel syndrome. Dash et al 23 noted an increase in 3-mm lateralization when including a flexor retinaculum release. Second, when using cadavers, we are unable to determine the physiologic effects of these changes in the tarsal tunnel. The cadaver is a reasonable model of in vivo anatomy; however, the pressure measurement of interstitial fluid in the cadaver is limited in its translation to clinical practice. Whether they actually cause symptomatic changes will need to be studied in a living population. Additionally, it was a common occurrence that our pressure probe placement shifted following operation. Although this was mitigated with ultrasound guidance and triplicate measurements, variability in tarsal tunnel pressures is inevitable because of changes in position. Finally, this calcaneal osteotomy is typically used for a varus ankle. Our cadavers were not measured preoperatively for varus or valgus predispositions. Perhaps living varus feet adjust for changes in pressure through tissue remodeling. This is another reason why future studies are required in living participants to fully understand the changes in dimension and pressure that occur following calcaneal osteotomy, regardless of technique used.
Conclusion
Minimally invasive calcaneal lateralization osteotomies significantly decrease tarsal tunnel volume and increase intratunnel pressure, potentially predisposing patients to tibial nerve compression. With that being said the average postoperative pressure was only 14 mm Hg and only 2 cadavers had 1 measurement each that exceeded 30 mm Hg. Thus, this significant change may not lead to a clinically important issue such as a tarsal tunnel syndrome. Although it would be helpful to know what pressure should concern us, this number does not exist in the literature. From a practical perspective, if a larger translation is required, a tarsal tunnel release can be performed. This will allow greater translation and should decrease the risk of substantial increase in tarsal tunnel pressure. Future studies will be aimed at quantifying how much additional translation is attainable with a tarsal tunnel release.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261420155 – Supplemental material for Changes in Tarsal Tunnel Volume and Pressure After Minimally Invasive Lateral Sliding Calcaneal Osteotomy: A Cadaveric Study
Supplemental material, sj-pdf-1-fao-10.1177_24730114261420155 for Changes in Tarsal Tunnel Volume and Pressure After Minimally Invasive Lateral Sliding Calcaneal Osteotomy: A Cadaveric Study by Christopher Warburton, William Rate, Quinn Ehlen, William Cade, Errol Bailey, Stephen Henry and Steven Steinlauf in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
Ethical approval was not required for this cadaveric study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Stryker provided the implants, the burrs, and the power boxes, and other necessary items. Miami Center for Orthopaedic Research and education provided funding for the project.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Errol Bailey, MD, and Steven Steinlauf, MD, are both paid consultants for Stryker and have developed the calcaneal cutting guides used in the study. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.