Abstract
Research Type:
Level 4 – Case series
Introduction/Purpose:
Varus ankle arthritis is increasingly recognized as a three-dimensional deformity involving the coronal, sagittal, and axial planes. While conventional supramalleolar osteotomies (SMOs) primarily address coronal malalignment, the role of axial plane correction remains underexplored. Dome SMO, a complete osteotomy, enables true three-dimensional realignment, yet its impact on axial rotation is not well understood. In advanced varus ankle arthritis, we have observed that axial plane rotation occurs concurrently with intentional varization of the distal tibial fragment, seemingly alleviating deforming forces and improving talar tilt. This phenomenon warrants further scientific investigation. The purpose of this study was to evaluate axial plane structural changes following dome SMO in advanced varus ankle arthritis, given its potential advantages over standard medial opening wedge SMOs.
Methods:
This retrospective analyzed prospectively collected data of patients with Takakura stage 3b varus ankle arthritis who underwent isolated dome SMO at a single institution. Patients who underwent any concurrent hindfoot or soft tissue procedures, such as tendon release or transfer, were excluded. All patients had valgus lower limb alignment and varus ankle involvement, making them unsuitable candidates for medial opening wedge osteotomies.
Intraoperative axial rotation of the distal tibia was assessed by inserting 1.6-mm Kirschner wires proximal and distal to the planned osteotomy site, photographed cranially before and after correction, and measured via ImageJ software.
Weightbearing radiographs were obtained preoperatively and at least one year postoperatively to assess talar tilt (TT) and medial distal tibial angle (MDTA). Additionally, weightbearing computed tomography (WBCT) evaluated axial plane changes, including the medial malleolus-talus angle, lateral malleolus-talus angle, and medial malleolus-talus distance. Pre- and postoperative Takakura stages were recorded.
Results:
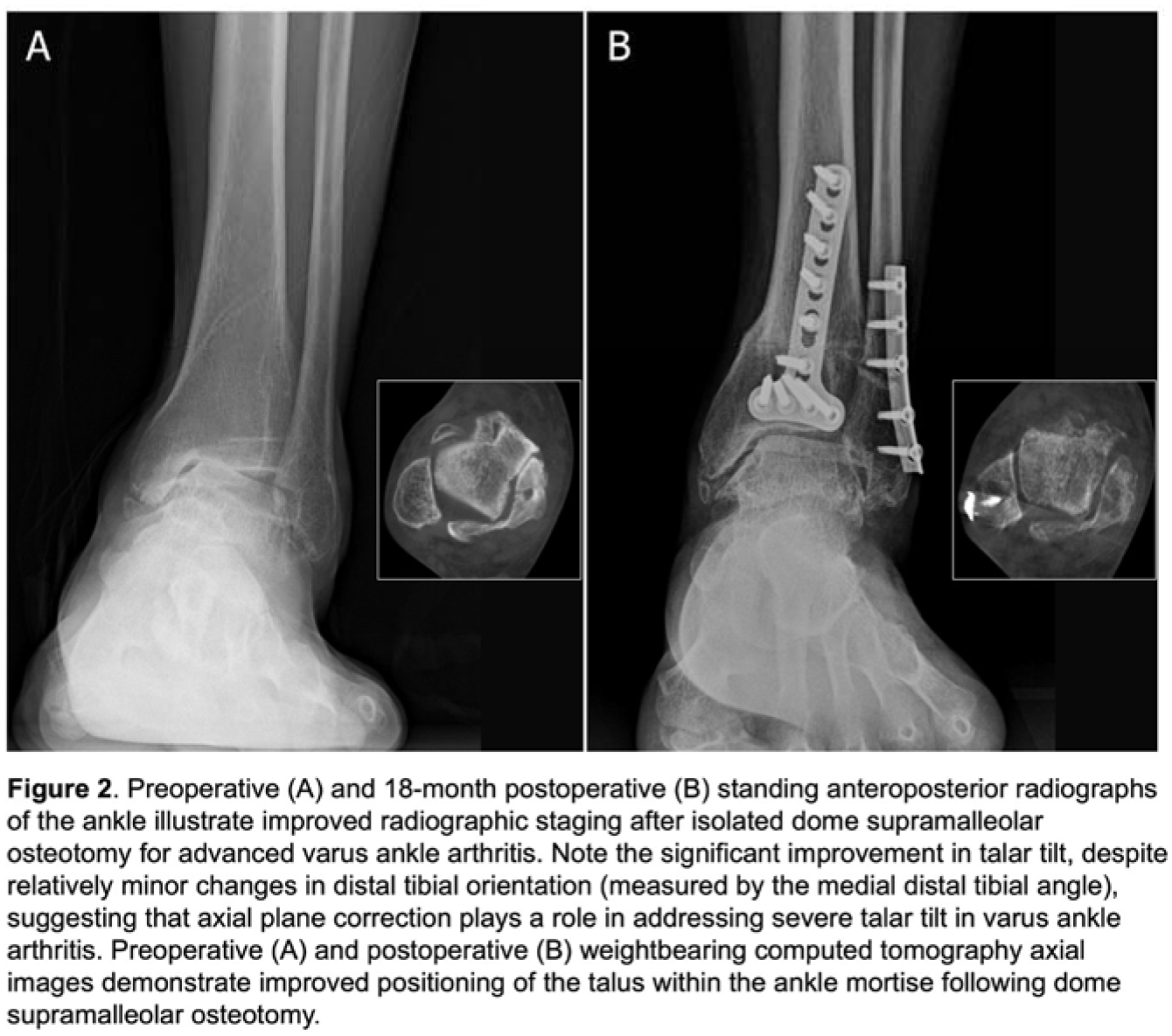
Eighteen ankles (17 patients; mean age: 60.1 years, mean follow-up: 16.6 months) met the inclusion criteria. Dome SMO resulted in a mean internal rotation of the distal tibia of 19.9° (SD 3.7) across the osteotomy site (Figure 1). On radiographs, TT significantly improved from 15.4° preoperatively to 6.7° postoperatively (p < 0.0001), while MDTA showed a modest change from 87.5° to 91.1°. WBCT analysis demonstrated external rotation of the talus within the ankle mortise, with both the medial and lateral malleolus-talus angles decreasing postoperatively. Sixteen ankles improved to Takakura stage 2 (Figure 2), indicating reduced varus deformity and improved talar tilt.
Conclusion:
This study highlights the significant axial plane changes in the distal tibia following dome SMO for advanced varus ankle arthritis. The simultaneous internal rotation of the distal tibia seems to help “untwist” deforming forces, resulting in improved talar tilt without the need for hindfoot or soft tissue procedures. The substantial improvement in talar tilt, despite only modest coronal realignment, suggests that rotational realignment plays a crucial role in joint preservation strategies for severe varus deformities. Although the study is limited by a small cohort and short-term follow-up, these findings underscore the importance of incorporating axial plane correction in SMO planning.