Abstract
Research Type:
Level 3 - Retrospective cohort study, Case-control study, Meta-analysis of Level 3 studies
Introduction/Purpose:
The use of weight-bearing computed tomography (WBCT) scans has steadily increased within the past five years and has shown to aid in the diagnosis and progression of foot and ankle orthopedic pathologies.1 WBCT allows the visualization of pathologies associated with impingement, joint space narrowing, and malalignment that would not be appreciated using other forms of radiographic imaging.1,3 However, current standards involve using two-dimensional (2D) imaging as a method of diagnosis in three-dimensional (3D) deformities of Charcot neuroarthropathy (CN).1,2,3 The purpose of this study was to quantify and compare the angular and distance measurements represented in standard 2D weight-bearing imaging and 3D WBCT for deformities detected in CN patients.
Methods:
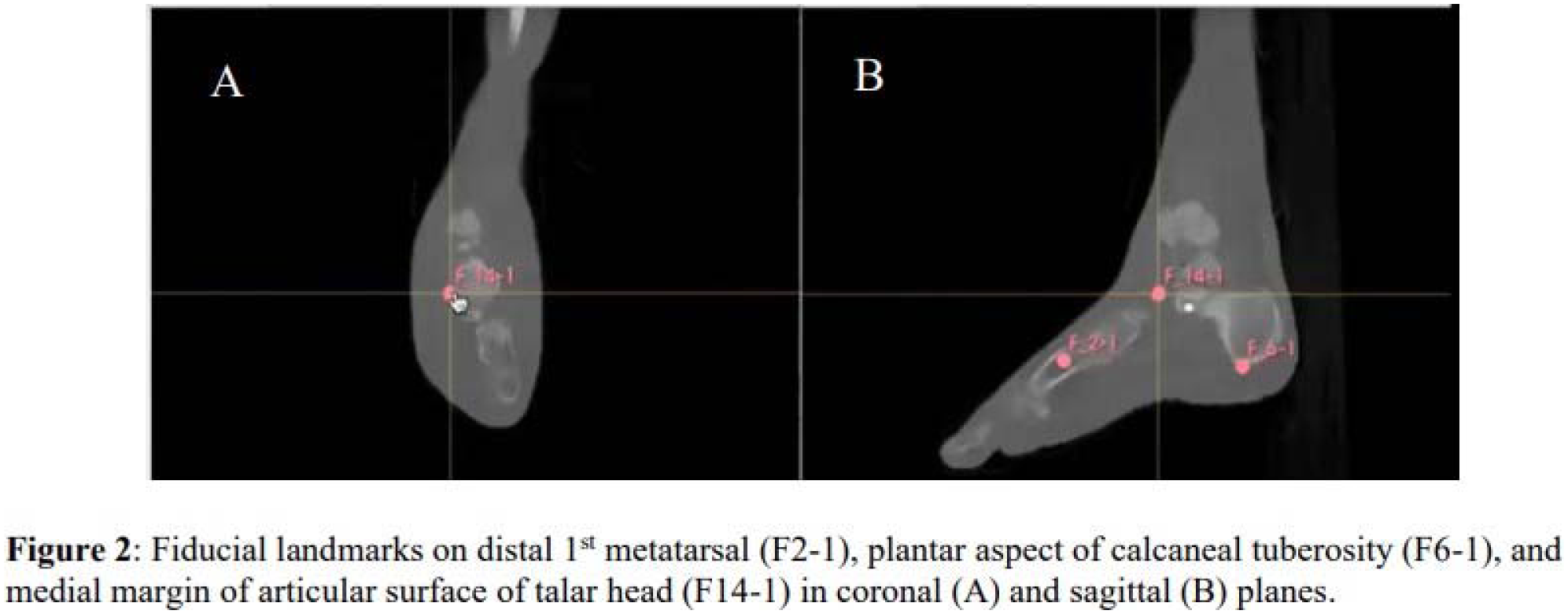
The 2D weight-bearing radiographs and 3D WBCT scans were measured for 10 patients with CN, from 2019 to 2024. 2D measurements were obtained by annotating planar radiographs. The 3D measurements were obtained by manually placing fiducials on anatomic landmarks. These fiducials were then input into a custom-built code to automatically transform the foot into a patient specific anatomic coordinate system and calculate all angle and distance measurements either in 3D or as projected on their true anatomic plane (Figure 2). Each radiograph and WBCT was measured by three observers. Statistical analysis included representing 2D and 3D measurements as means +/- standard deviation, and any variation between the two methods was evaluated using paired t-test. This study was approved by our institutions IRB.
Results:
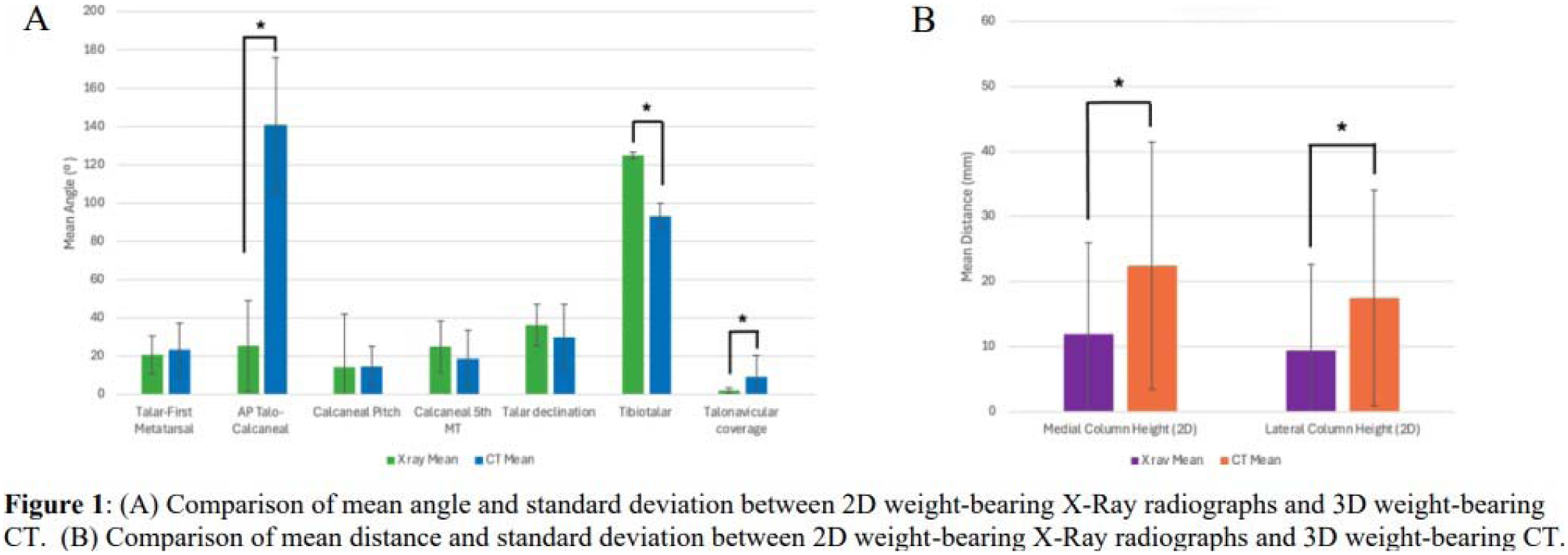
The AP talocalcaneal angle was significantly greater in 3D WBCT compared to weight-bearing radiographs (140.63 ± 35.39º vs. 25.35 ± 23.94º, p < 0.0001). Similarly, the talonavicular angle was significantly greater in 3D WBCT compared to weight-bearing radiographs (9.06 ± 11.36º vs. 2.04 ± 1.27º, p = 0.0012). The medial column heights were significantly greater (22.45 ± 19.03 mm vs. 11.85 ± 14.18 mm, p = 0.016) and lateral column heights were significantly greater (17.50 ± 16.63 mm vs. 9.40 ± 13.28 mm, p = 0.027) in 3D WBCT compared to weight-bearing radiographs. Conversely, the tibiotalar angle was significantly lower in 3D WBCT compared to weight-bearing radiographs (93.06 ± 6.83º vs. 124.99 ± 10.87º, p < 0.0001) (Figure 1).
Conclusion:
This study compared weight-bearing 2D radiographs and 3D WBCT for CN and found significant differences in several angular and distance measurements used to describe the pathological deformities. Therefore, true pathological alignment of the joints and deformities evident in CN deviate from weight-bearing 2D radiographs compared to 3D WBCT. This potentially enables earlier and improved detection, and better understanding of the severity of deformity in CN. With the increase in use of WBCT in foot and ankle orthopedics, this study incorporates a novel method of analyzing WBCT data in order to aid in the diagnosis and progression of CN.