Abstract
Research Type:
Level 2 - Prospective comparative study, Meta-analysis of Level 2 studies or Level 1 studies with inconsistent results
Introduction/Purpose:
Adult acquired flatfoot deformity is characterized by medial rotation and plantar flexion of the talus, eversion of the calcaneus, collapsed medial arch and abduction of the forefoot and occurs in between 5-37% of the population. A stage II flexible flatfoot can be treated with a medializing calcaneal osteotomy and a transfer of the flexor digitorum longus (FDL) tendon. This is currently usually performed using a Metal/Biotenodesis screw. The human allogenic cortical bone screw is an alternative and forms a solid bony unit immediately after implantation, which is remodeled into the patient's own trabecular bone. The aim of this study is to evaluate the outcome after medializing calcaneal osteotomy (± FDL-transfer) with the human allogeneic cortical bone screw in comparison to the Metal/Biotenodesis-screws.
Methods:
Forty-eight patients were treated with medializing calcaneal osteotomy, and if necessary, with FDL transfer. They were divided into 2 cohorts one being treated with the human allogeneic cortical bone screw, the other with the Metal/Biotenodesis-screw. Patient Related Radiological (time to union) and Patient-Related Outcome Measures (PROMS) were recorded for at up to 24 months: American Orthopedic Foot and Ankle Outcome Score (AOFAS), Foot and Ankle Outcome Score (FAOS), Foot Function Index (FFI) and VAS-Pain Score (VAS). Follow-up-visits were performed at 6 weeks, 6, 12 and 24 months.
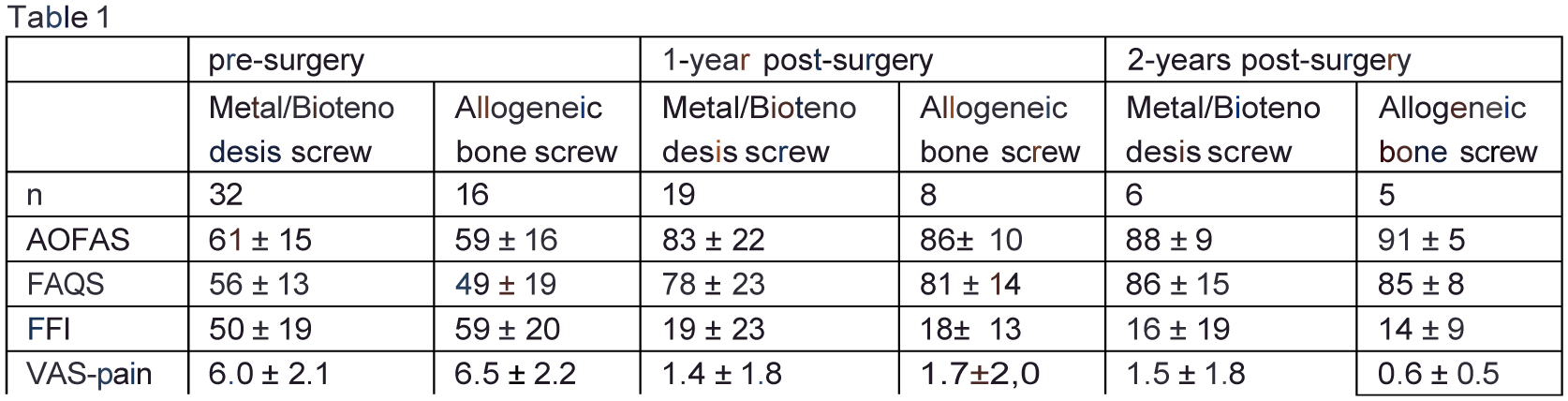
Results:
Complete union was recorded after 3.6 months and 4.5 months for the human allogeneic cortical bone screw (fig.1) and Metal/Biotenodesis group, respectively. PROM's of 27 patients after 1-year and 11 patients after 2 years are shown in the tab 1. For both groups, the PROM's improved (tab 1, fig. 2). The available data indicate that the allogeneic bone screw group tend to achieve better results earlier, for all PROM's (tab 1, fig. 2). A total of 11 implant removals (33%) were performed in the Metal/Biotenodesis group.
Conclusion:
Both methods led to similar clinical and radiologic outcomes. However, patients in the cortical bone screw group tend to recover faster than patients in the Metal/Biotenodesis group and do not need a second operation for metal removal. One characteristic of the human allogeneic cortical bone screw is its inherent biocompatibility, which might be an additional advantage in the process of bone healing.