Abstract
Research Type:
Level 3 - Retrospective cohort study, Case-control study, Meta-analysis of Level 3 studies
Introduction/Purpose:
Diabetic foot complications are a leading cause of limb loss, with minor amputations often performed as a limb-salvage strategy. However, their long-term impact on survival and the prevention of major amputations remains unclear. While transmetatarsal and ray amputations preserve limb function, high ulcer recurrence and reamputation rates raise concerns about their effectiveness. Most studies report short-term outcomes, but data on long-term survival and reamputation risks are scarce. This study aimed to evaluate a decade-long follow-up of diabetic patients undergoing minor amputations, focusing on overall survival, ulcer recurrence, and reamputation rates.
Methods:
This retrospective cohort study analyzed diabetic patients who underwent ray or transmetatarsal amputations at a tertiary hospital between 2013 and 2022. Patient data, including demographics, comorbidities, and surgical outcomes, were extracted from medical records. Survival analysis was performed using the Kaplan-Meier method, with a primary outcome of overall survival and secondary outcomes including ulcer recurrence and need for reamputation. Patients with less than one year of follow-up were excluded to ensure data reliability. Statistical comparisons were conducted using log-rank tests and Cox proportional hazards models. With a mean follow-up of 55.4 months (range: 19.5–131.9 months), this study provides one of the most comprehensive long-term analyses of minor amputations in diabetic foot patients.
Results:
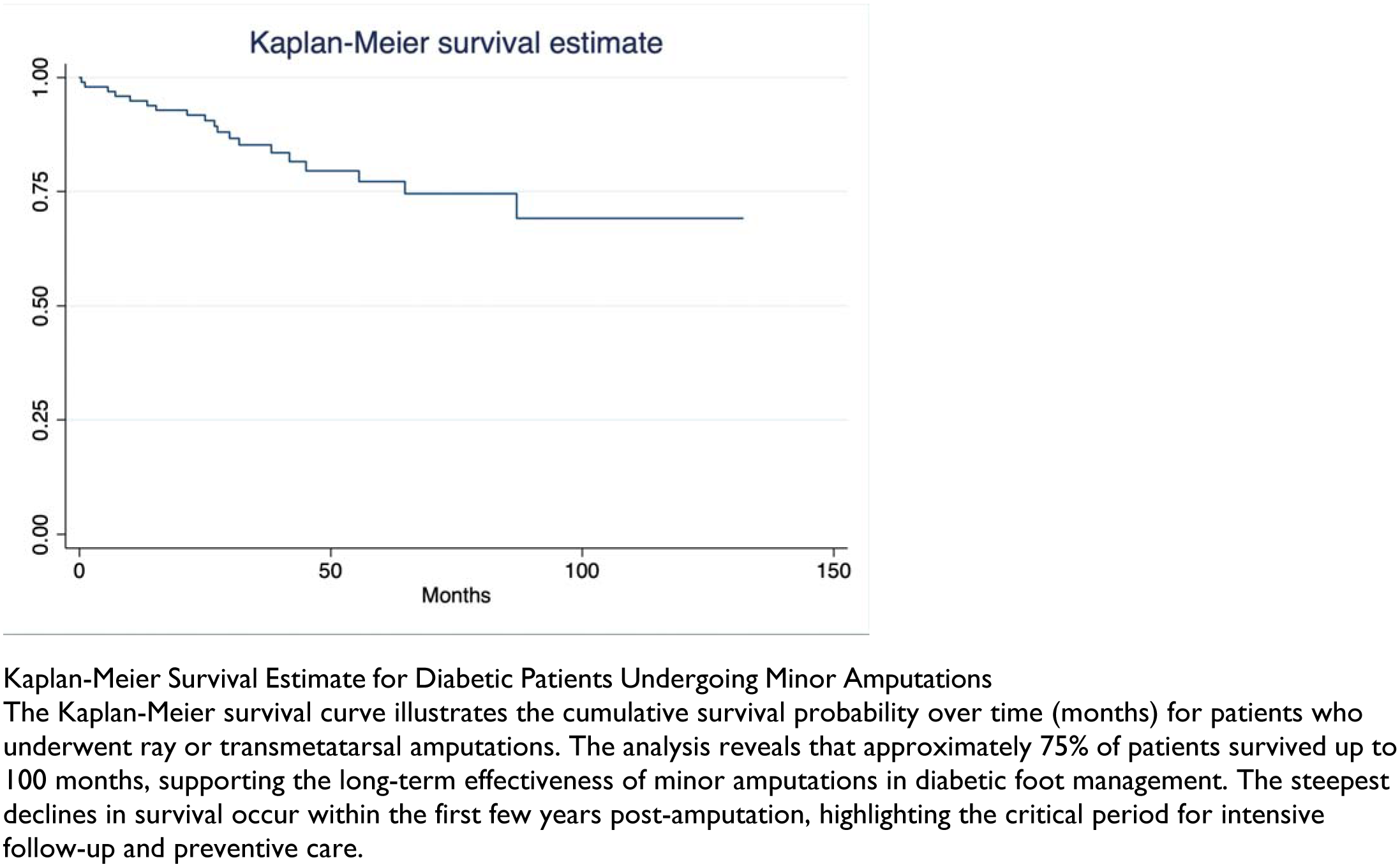
A total of 100 patients were included, with a mean survival of 47.9 months. Kaplan-Meier analysis showed that 75% of patients survived up to 100 months, indicating favorable long-term outcomes compared to historical major amputation data. The two-year mortality rate was 20.4%, lower than previously reported rates (29–35%). Ulcer recurrence was observed in 53.2% of patients, with some experiencing up to seven recurrences. Reamputation was required in 26% of cases, with a proximal progression pattern. Notably, only 6.67% of patients with transmetatarsal amputations progressed to transtibial amputation, suggesting that minor amputations effectively delay or prevent major limb loss when combined with structured postoperative care.
Conclusion:
This 10-year follow-up study reinforces the role of minor amputations in preserving limb function and reducing the need for major amputations in diabetic foot patients. Despite high ulcer recurrence and a 26% reamputation rate, most patients did not require proximal amputations. The lower-than-expected two-year mortality rate (20.4%) suggests that structured postoperative care significantly contributes to improved survival. These findings emphasize the need for long-term follow-up, early intervention, and patient-centered management to enhance outcomes. These findings highlight the importance of long-term monitoring and multidisciplinary management to optimize outcomes.