Abstract
Research Type:
Level 3 - Retrospective cohort study, Case-control study, Meta-analysis of Level 3 studies
Introduction/Purpose:
Total Ankle Replacement (TAR) is an accepted treatment of end-stage ankle osteoarthritis (AOA). Valgus AOA poses a particular challenge due to the technical complexity of reconstructive efforts, often requiring additional realignment procedures in conjunction with TAR. Furthermore, frequency of these complex operations is increasing. Introduction of primary stemmed tibial implants have expanded TAR indications for challenging AOA deformities. Advancements in Weight Bearing Computed Tomography (WBCT) have improved surgical planning and precision. Despite this, current literature lacks characterization of factors that may influence the need for concurrent realignment procedures during valgus AOA TAR. In this study, we investigated these factors as well as those affecting short-term patient-reported outcomes. We hypothesized that valgus severity would correlate with additional procedures and poorer outcomes.
Methods:
This was a single-institution retrospective cohort study of 31 patients with valgus AOA who underwent primary TAR between January 2022 and April 2024 with available preoperative WBCT imaging and minimum follow-up of 6 months (13.26±6.87 months). There were 25.8% post-traumatic and 67.6% Progressive Collapsing Foot Deformity (PCFD) aetiologies. Patient demographics, operative details (implant type, concomitant realignment procedures), postoperative complications, and patient outcome scores (preoperative and postoperative PROMIS Pain Interference and Physical Function) were all collected and included for analysis. Pre- and post-operative alignments were measured using WBCT and radiographs, respectively. Descriptive statistics summarized the data, and comparisons were conducted using appropriate tests based on distribution. A multivariate linear regression analyzed Post-op PROMIS pain scores with FAO and Pre-op PROMIS pain score as predictors. Normality was assessed using the Shapiro-Wilk test. Statistical significance was set at p< 0.05.
Results:
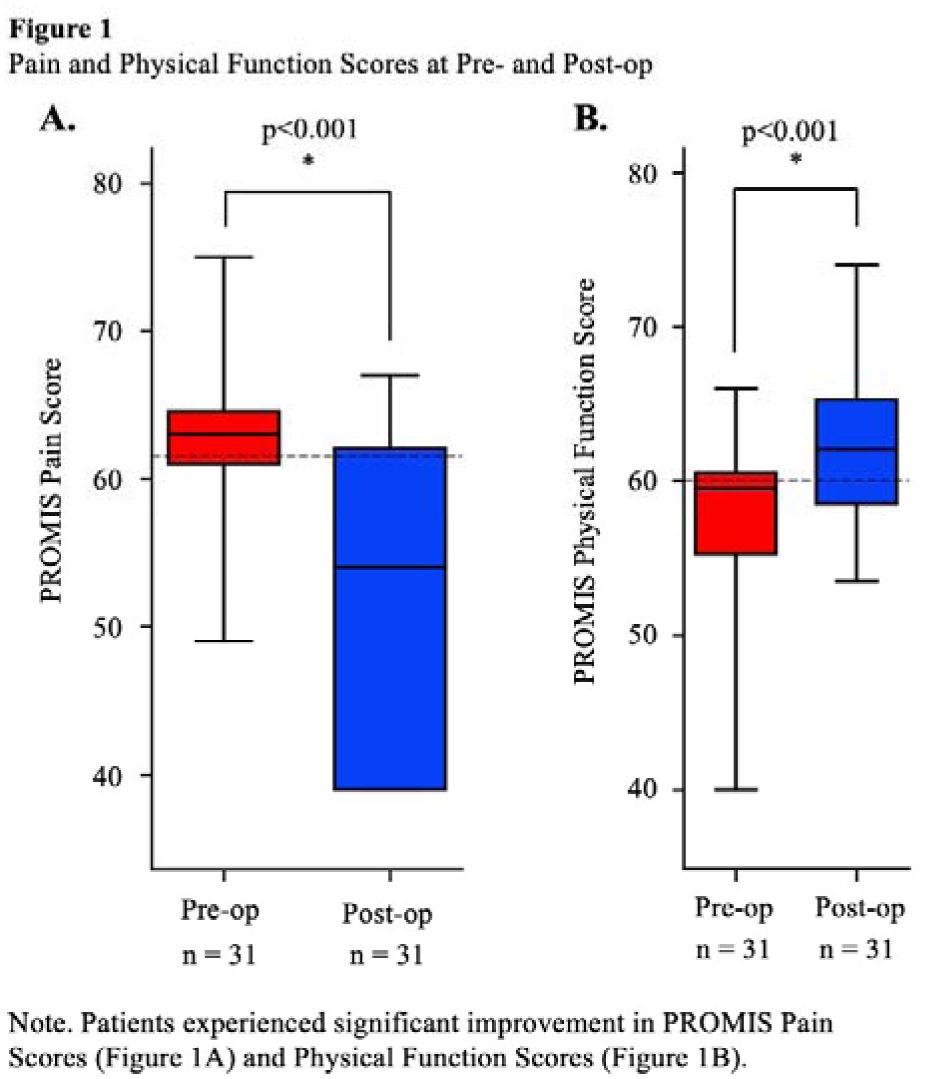
Concomitant realignment procedures were performed in 87.1% of cases, including 41.9% fusions, 32.3% osteotomies, and 80.6% soft-tissue reconstructions. 15 of 31 patients (48.4%) underwent TAR with stemmed implant, with no differences in outcomes by implant type. Severe valgus AOA (FAO≥16%) correlated with increased postoperative pain interference (p < 0.05) and higher likelihood of ≥2 realignment procedures (p < 0.05). PCFD Class C cases demonstrated greater preoperative FAO and increased likelihood of adjunct realignment procedures and stemmed implants (p < 0.05). PROMIS scores significantly improved following surgery, with Pain Interference decreasing from 63.0 to 54.0 (p < 0.001), and Physical Function increasing from 39.0 to 44.0 (p < 0.001). In multivariate analysis, higher pre-operative PROMIS pain score (p=0.0354) and FAO≥20.0 (p=0.0163) were associated with higher values of post-operative PROMIS pain score.
Conclusion:
Severe preoperative valgus deformity (FAO value of 16% or higher) was found to be the most significant predictor of requiring two or more associated realignment procedures, as well as to correlate with lower postoperative outcomes scores. Cases of PCFD with Class C deformity (arch collapse) were found to have more severe preoperative deformities and were more likely to require a stemmed implant for treatment. We also confirmed that TAR successfully improved short term PROMIS in end-stage valgus AOA. Further research, including longer-term and prospective studies, is necessary to validate the results of the current investigation.