Abstract
Research Type:
Level 3 - Retrospective cohort study, Case-control study, Meta-analysis of Level 3 studies
Introduction/Purpose:
Reduced foot muscle strength has been identified as a significant risk factor for recurrent falls, particularly in older adults. Radiographic assessments, such as Magnetic Resonance Imaging (MRI), have demonstrated that foot muscle size, as measured by Cross Sectional Area (CSA), correlates with muscle strength. However, the direct relationship between foot muscle CSA and the risk of recurrent falls remains poorly understood. Establishing this relationship is critical, as it could enhance our understanding of fall biomechanics and inform targeted interventions to prevent falls. This study aimed to investigate the association between foot muscle CSA, as quantified through MRI, and a history of recurrent falls.
Methods:
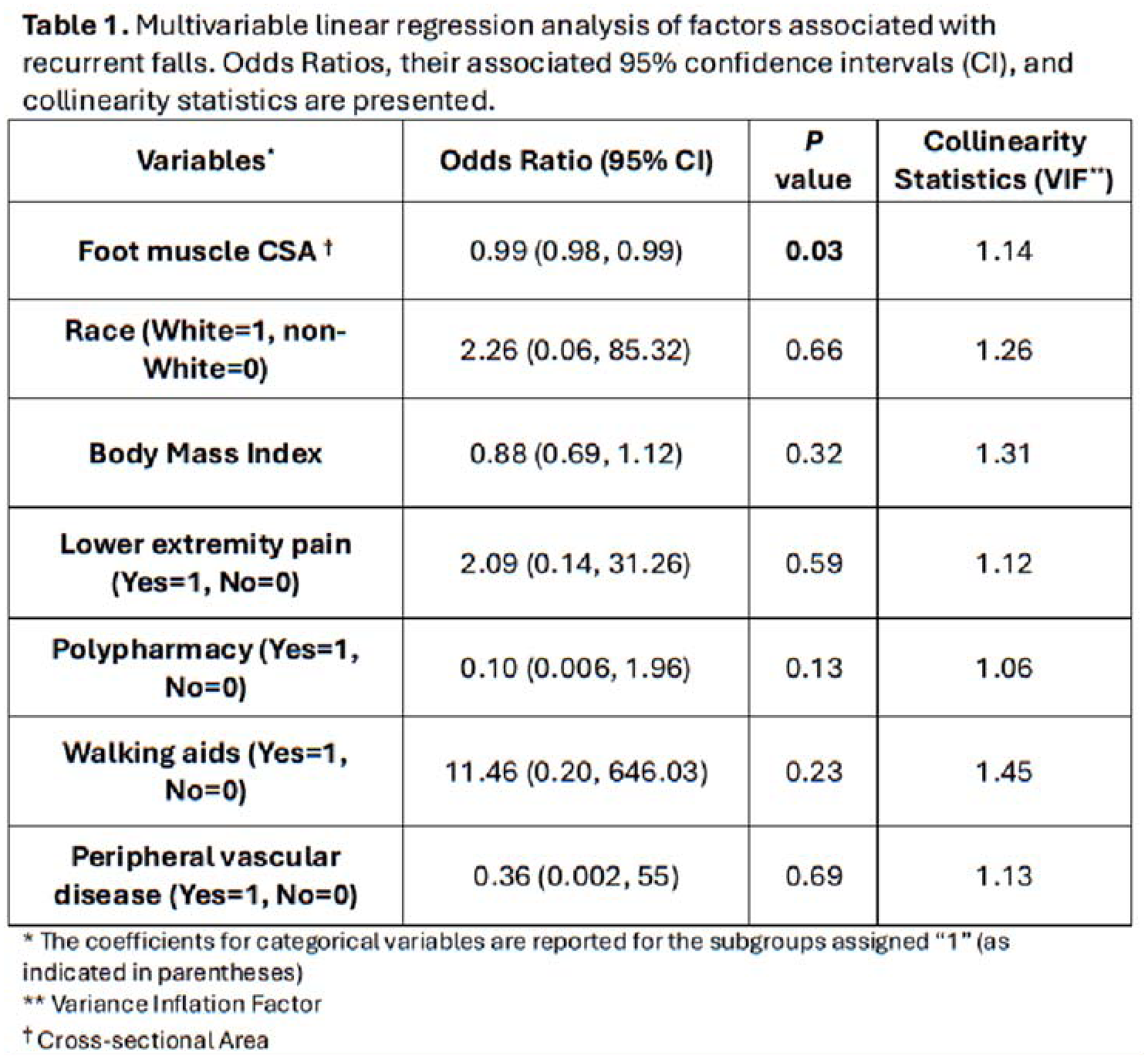
A retrospective case-control study included patients aged ≥60 years with a history of repeated falls (≥2) and age- and sex-matched controls without falls. Demographic data were collected along with clinical variables associated with falls, including polypharmacy (≥5 medications), use of walking aids, and history of lower extremity vascular disease or pain. Foot muscle CSA at the first tarsometatarsal joint was measured on T1-weighted (n=8) or proton density (n=18) MRI images using OsiriX Lite software (Figure 1). Non-contractile components, including bone, tendon, and fat, were excluded based on their distinct signal intensity compared to muscle tissue. Measurements were performed by two independent raters, with inter-rater agreement assessed via the Intraclass Correlation Coefficient (ICC). Multiple regression analysis was performed, adjusting for potential confounding variables (Table 1). Statistical significance was set at P < 0.05. Continuous values were presented as Mean ± Standard Deviation.
Results:
A total of 26 patients were included, with 13 in the case group (age: 70.62 ± 8.54 years) and 13 in the control group (age: 69.46 ± 6.86 years), maintaining an equal gender distribution (38% female). Baseline characteristics were not different between groups, except for CSA measurements [cases: 285.5 ± 220.17 mm2, controls: 542.03 ± 218.62 mm2; P=0.006]. The interrater agreement was calculated to be excellent (ICC=0.92, P < 0.001). Foot muscle CSA was shown to be inversely associated with recurrent falls (P=0.03; Table 1) even when adjusted for other fall-related variables.
Conclusion:
Reduced foot muscle CSA on MRI is independently associated with an increased risk of recurrent falls in older adults. Although preliminary, these results suggest that CSA measurements could be a valuable tool for identifying individuals at risk of recurrent falls. Additionally, CSA may serve as a valuable monitoring metric to assess the effectiveness of interventions aimed at preserving or enhancing foot muscle strength in this population.