Abstract
Research Type:
Level 3 - Retrospective cohort study, Case-control study, Meta-analysis of Level 3 studies
Introduction/Purpose:
There has been a substantial increase in the utilization of total ankle arthroplasty (TAA) in recent years. However, there is a paucity of literature encompassing a comprehensive evaluation of the influence of socioeconomic factors on TAA outcomes. This study aims to use a large deidentified database to identify the effect of socioeconomic factors on outcomes following TAA.
Methods:
The National Inpatient Sample (NIS) was queried from 2016-2019 using International Classification of Diseases codes for TAA to identify 21,360 patients. Patient information collected included age, sex, race, primary payer status, year of surgery, length of hospital stay (LOS), and median household income quartile (determined using patient zip code). Patients were grouped by race (White, Black, Hispanic), insurance type (Medicare, Medicaid, and Private), and income quartile (Q1-4 with Q1 being the lowest) and analyzed for comorbidity score, length of stay, mortality, adverse discharge, and complications.
Results:
Within the NIS database, black patients undergoing TAA were statistically significantly younger, more female, had a higher rate of comorbidities, and most often were in the lowest income quartile as compared to white patients. Similarly, Hispanic patients were statistically significantly younger and from the lowest income quartile as compared to white patients. Black and Hispanic patients had statistically significantly increased risk of extended LOS ≥4 days (Black: odds ratio [OR]=1.947) (Hispanic: OR=2.054), adverse discharge to facility (Black: OR=1.450) (Hispanic: OR=1.205), additionally, black patients were at increased risk of any complication (Black: OR=1.404).
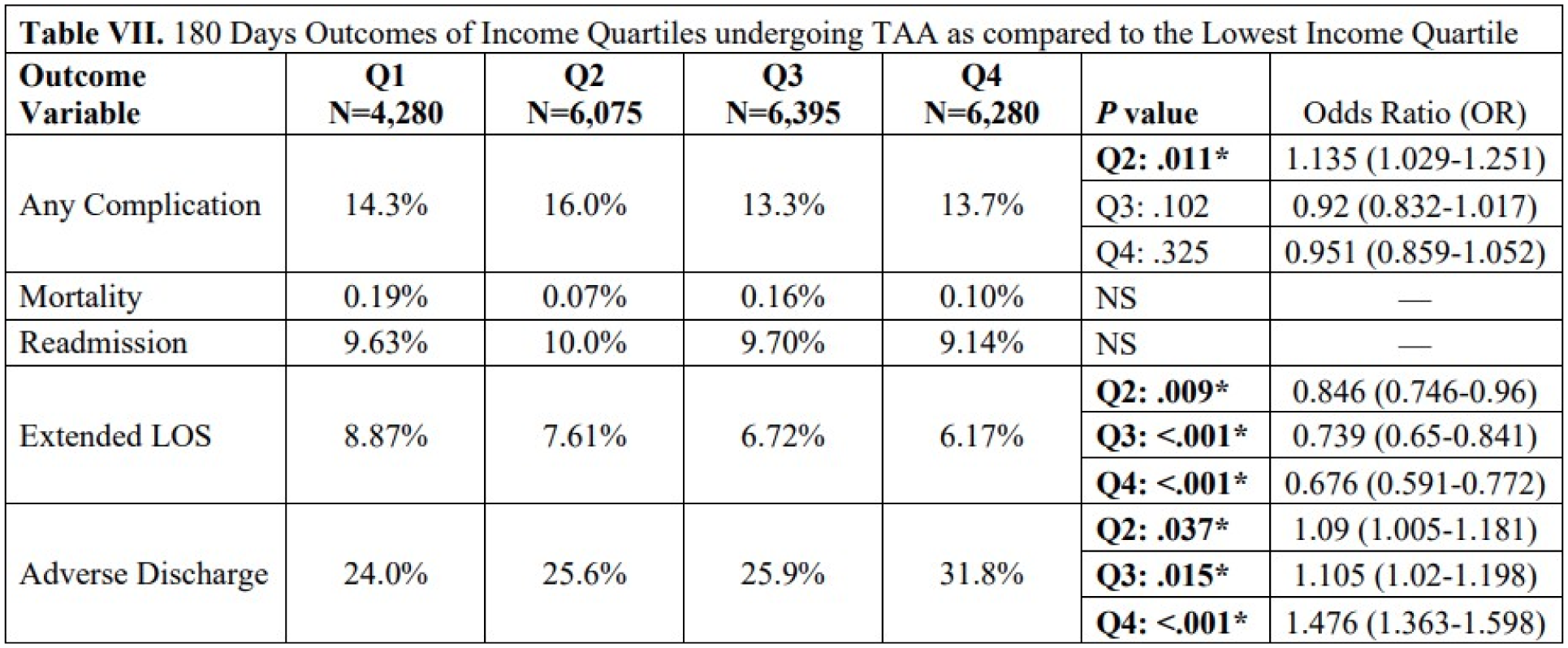
Conclusion:
Patients of minority races undergoing TAA were found to be at significantly greater risk of adverse outcomes postoperatively. Interestingly, lower mean zip code income quartile was found to be predictive of greater risk for extended length of stay. These findings are valuable to increase our understanding of the complex interplay between socioeconomic factors and operative outcomes.