Abstract
Research Type:
Level 4 – Case series
Introduction/Purpose:
Posterior tibial tendon dysfunction (PTTD) is a common cause of adult-acquired flatfoot deformity, often requiring surgical intervention in advanced stages. Medial displacement calcaneal osteotomy (MDCO) and flexor digitorum longus (FDL) tendon transfer are frequently employed procedures for managing severe PTTD. This study aims to investigate the biomechanical impact of MDCO and FDL transfer on PTT tension, providing insights crucial for optimizing surgical techniques and improving patient outcomes in PTTD management.
Methods:
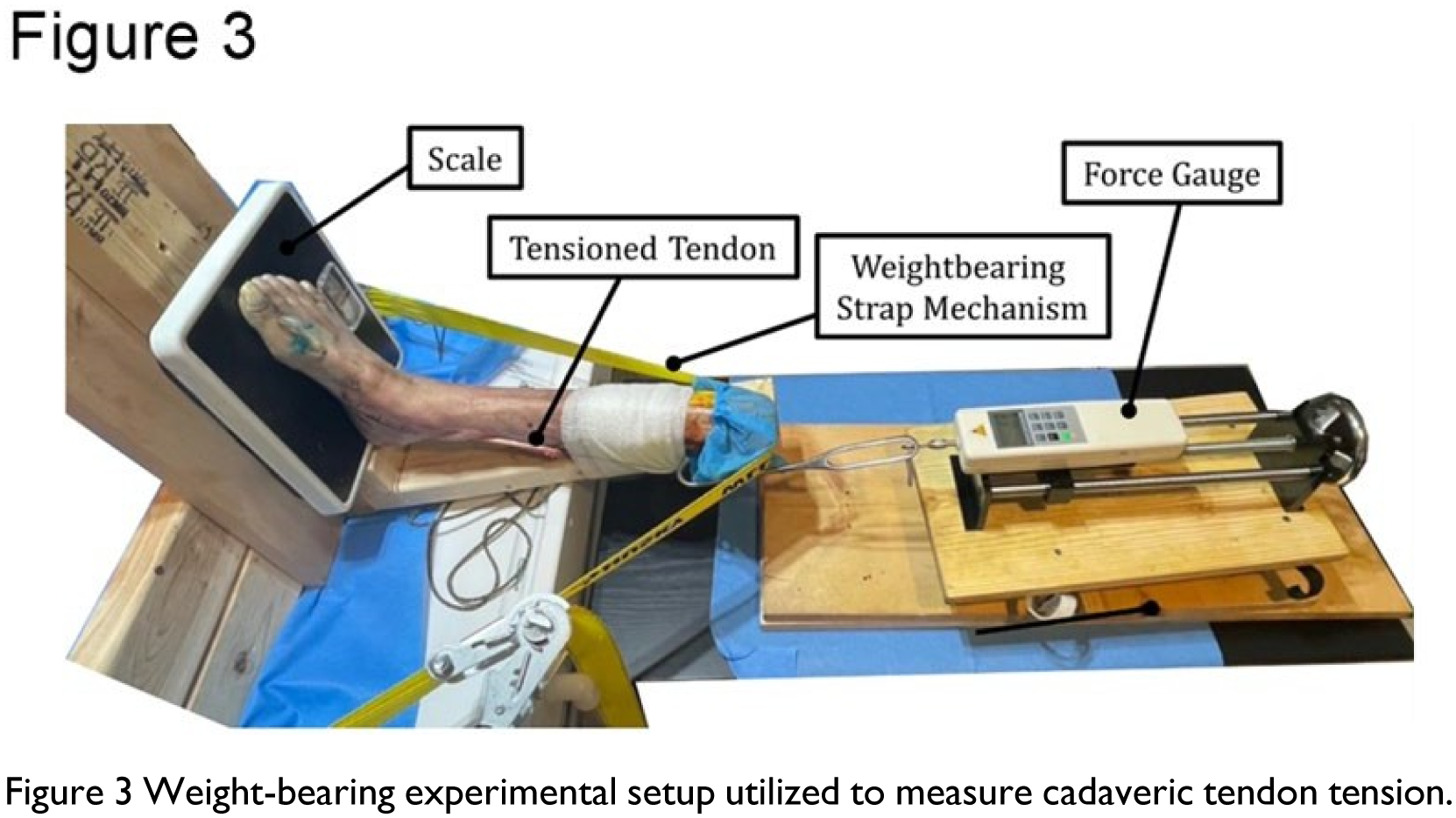
Twelve fresh-frozen cadaveric lower limbs (mean age: 65 ± 8 years) were disarticulated at the knee. The PTT was transected mid-tibia and prepared using the Krackow technique. The FDL was harvested after separation from the knot of Henry. For FDL transfer, an anchor was inserted to the navicular’s most prominent portion under C-arm guidance, securing the tendon transfer. Specimens were mounted in a testing system simulating 37.5 kg weight-bearing. MDCO was performed at 2, 4, 6, 8, and 10 mm, with PTT strain measured under both MDCO alone and MDCO with FDL transfer. The force meter recorded variations following pretensioning at 10N and controlled tendon excursion. The primary outcome was mean PTT strain across conditions, analyzed via the Friedman test with post hoc comparisons.
Results:
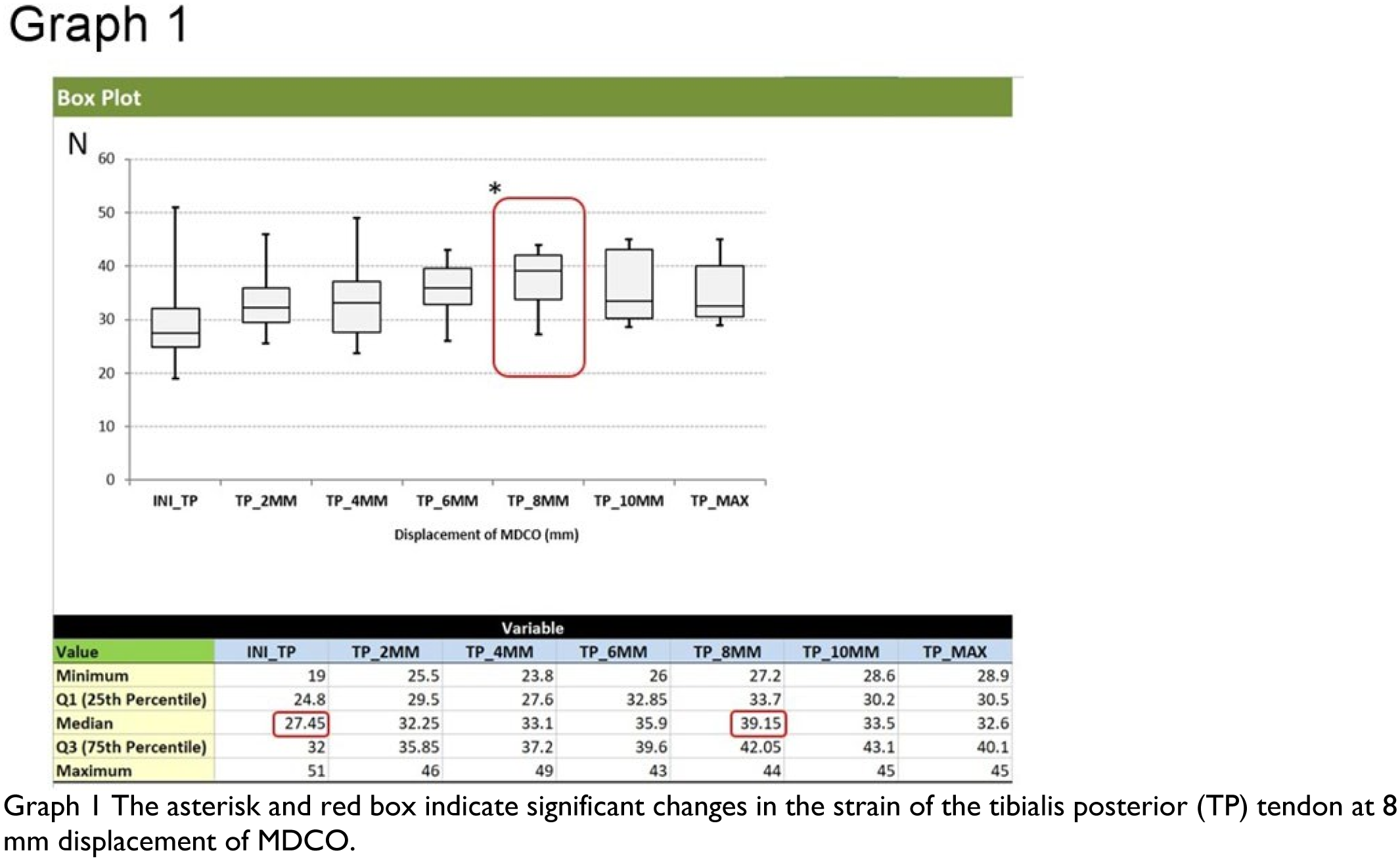
In 12 cadaveric specimens, PTT strain significantly increased from a preoperative median of 27.45 N to 39.15 N at 8 mm of MDCO (p = 0.004), representing peak strain. In 10 specimens with MDCO and FDL transfer, PTT strain rose from 28.95 N to 37 N at 6 mm (p = 0.004) and 40 N at 8 mm (p = 0.002). FDL transfer alone had no significant effect (p = 0.284). Friedman test showed that PTT strain increased at 2 mm MDCO but differed significantly from baseline only beyond 4 mm (p = 0.001). The highest strain occurred at 8 mm MDCO with FDL transfer. Strain did not exceed this level beyond 10 mm MDCO.
Conclusion:
MDCO significantly decreases PTT strain, with peak strain observed at 8 mm of displacement. Adding FDL tendon transfer further amplifies PTT strain, particularly beyond 4 mm of MDCO, with the highest strain recorded at 8 mm of displacement. Based on strain changes, 8 mm of displacement in solitary MDCO appears optimal and suitable for combining FDL transfer. We recommend an ideal displacement of 8 mm in MDCO or MDCO with FDL transfer, corresponding to 56% of the maximal displacement. Without MDCO, solitary FDL transfer does not significantly alter PTT strain.