Abstract
Research Type:
Level 3 - Retrospective cohort study, Case-control study, Meta-analysis of Level 3 studies
Introduction/Purpose:
Under physiological conditions, the center of rotation of the subtalar joint (STJ) is located at the middle facet. Previous studies have shown that the progression of Progressive Collapsing Foot Deformity (PCFD) follows a specific sequence: peritalar subluxation (PTS) without impingement, sinus tarsi impingement (STI), subfibular impingement (SFI), and, in the most severe cases, valgus talar tilt (class E). However, no longitudinal study has yet examined the behavior of the STJ to confirm this sequence. The aim of this cross-sectional progression modeling analysis was to analyze the subtalar joint behavior across a wide spectrum of PCFD severity in a large cohort. We hypothesized that the STJ’s contribution to the deformity varies depending on the presence or absence of impingement.
Methods:
We conducted a retrospective comparative study of 173 PCFD cases (116 women, 57 men; mean BMI 32.3±6.8 kg/m²; mean age 56±14.7 years) with available Weight Bearing CT (WBCT).They were divided into 5 groups: patients without PTS: “no-PTS” (16.2%), PTS without impingement: “PTS no-IMP” (11%), PTS with subtalar impingement: “PTS-STI” (41.6%), PTS with sinus tarsi impingement: “PTS-SFI” (19.7%), and class E (11.6%). Foot and ankle offset (FAO), middle facet subluxation (MFS) and incongruence angle (INC) were measured. Subtalar joint offset (SJO) and lateral process offset (LPO) were measured using the proximal aspect of the calcaneal middle facet (SJO) and the distal extremity of the talar lateral process (LPO), relative to the WB foot tripod. The difference between SJO and LPO was calculated (SJO-LPO). Measurements were compared across groups based on hindfoot alignment (HA). Statistical significance was set at p< 0.05.
Results:
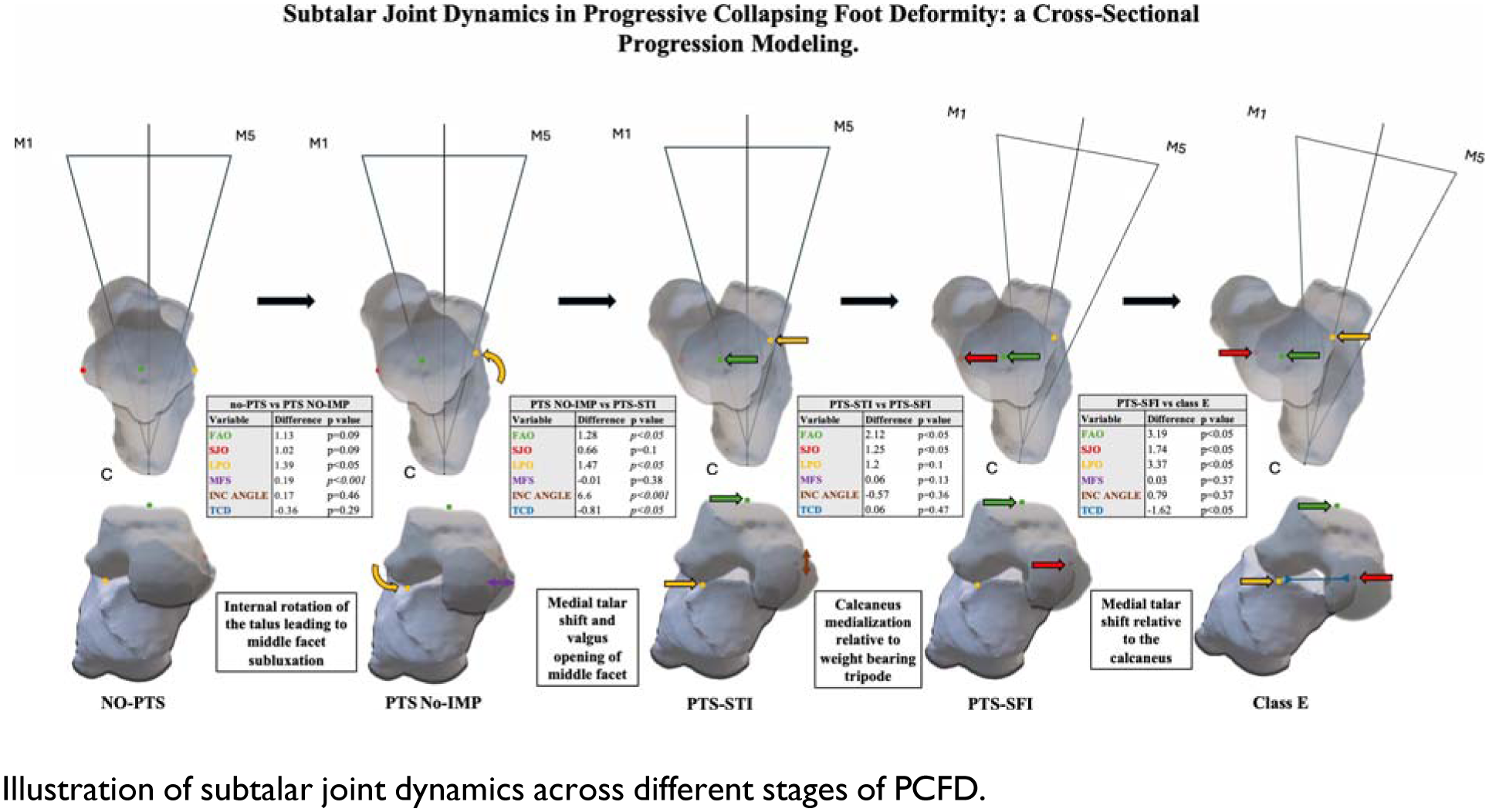
Between “no-PTS” and “PTS no-IMP”, only MFS (0.16±0.06 vs 0.35±0.08; p< 0.001) and LPO (-2.04±3.27 vs - 0.65±2.22; p< 0.05) significantly increased, reflecting internal rotation of the talus (medialization of LPO, stable FAO and SJO). Between “PTS no-IMP” and “PTS-STI”, significant increases in FAO (7.03±2.32 vs 8.31±3.64; p< 0.05), LPO (-0.65±2.23 vs 0.82±3.3; p< 0.05), INC (8.23±5.64 vs 14.83±7.04; p< 0.001) and decrease in SJO-LPO (19.18±1.43 vs 18.37±2.29; p< 0.05) corresponded to medial talar shift and valgus opening of the middle facet. Between “PTS-STI” and “PTS-SFI”, FAO (8.31±3.64 vs 10.43±5.08; p< 0.05) and SJO (19.19±2.92 vs 20.44±3.39 p< 0.05) increased significantly, indicating middle facet medialization (absence of STJ involvement in FAO increase). Between “PTS-SFI” and “class E”, FAO, SJO, LPO, and SJO-LPO increased significantly (p < 0.05), reflecting medial shift of the talus above the calcaneus.
Conclusion:
In this cross-sectional progression modeling study, PCFD progression involved primary talus internal rotation and medial shift until STI. Subsequently, STJ involvement in PCFD progression decreases until occurrence of talar tilt. Following talar tilt, the stresses applied to the subtalar joint due to its inclination lead to a significant medial translation of the talus over the calcaneus. These results clarify SJ behavior in PCFD and could provide guidance as to further studies are necessary to better understand midfoot and forefoot contributions to the deformity.