Abstract
Research Type:
Level 4 – Case series
Introduction/Purpose:
Müller-Weiss disease (MWD) is a rare orthopedic condition involving navicular bone collapse and fragmentation, leading to midfoot and hindfoot deformities. Structural deficits, malalignment, and poor vascularity complicate surgical treatment, increasing the risk of nonunion and poor functional outcomes. No consensus exists on the optimal surgical approach. We developed a novel technique to resect the collapsed lateral and central navicular segments while preserving the viable medial pole and reconstructing the central column with a structural bone allograft. We hypothesize that this approach improves foot alignment while maintaining a vascularized medial column for predictable healing and successful allograft incorporation.
Methods:
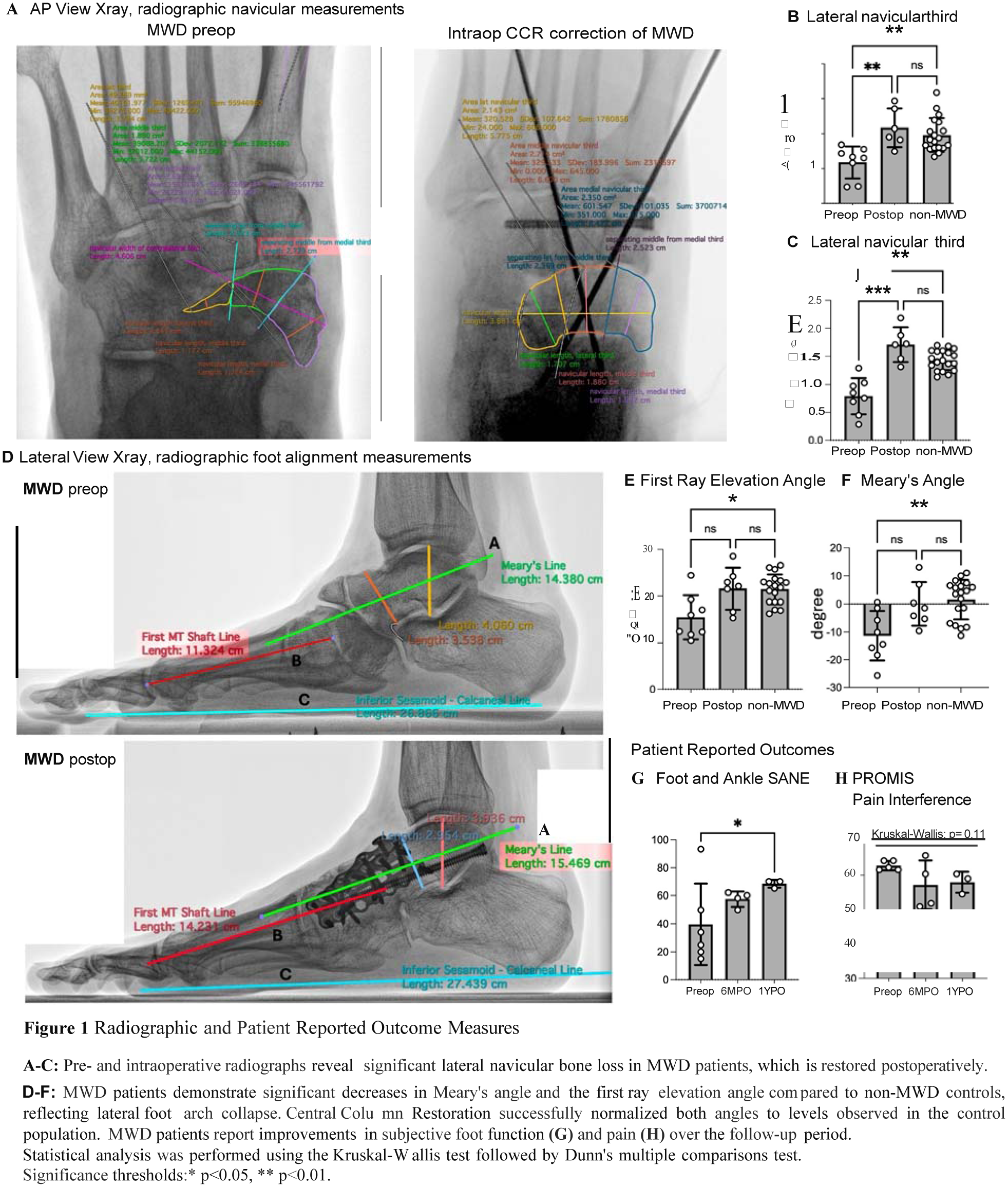
Seven consecutive MWD patients treated between 2021 and 2024 were scheduled for surgery. The medial navicular pole and soft tissue attachments were preserved, while the lateral navicular segment was debrided. Central column alignment was restored using a structural allograft (e.g., femoral head) shaped to replace the central and lateral navicular. Radiographic analysis included navicular width, measured as the largest bone diameter, with thirds defined perpendicular to the talonavicular joint surface. To mitigate distortion from fragmentation, contralateral navicular width was used as a reference. Lateral foot alignment was assessed using Meary’s angle, measuring the intersection of the talar and first metatarsal midline axes, and the First Ray Elevation Angle, quantifying forefoot collapse. Pre- and postoperative radiographic parameters and patient-reported outcome measures (PROMs) were retrospectively compared with a control cohort without navicular abnormalities.
Results:
Central Column Restoration restored the lateral third navicular anatomy (Fig1A-C) and improved lateral foot alignment parameters (Meary’s angle and first ray elevation angle) to levels observed in non-MWD controls (Fig1D-F). PROMs showed significant improvements in foot function (Foot and Ankle SANE, Fig1G)) and a downward trend of pain interference (PROMIS Pain Interference, Fig1H) 12 months postoperatively.
Conclusion:
Central Column Restoration with structural bone allograft effectively corrects MWD-related deformities and can improve functional outcome scores post-surgically, potentially allowing for a return to higher-level function. Further studies with larger cohorts and extended follow-up are necessary to confirm these findings and evaluate long-term outcomes.