Abstract
Research Type:
Level 3 - Retrospective cohort study, Case-control study, Meta-analysis of Level 3 studies
Introduction/Purpose:
Total ankle arthroplasty (TAA) has become an increasingly common procedure for managing end-stage arthritis. While primary TAA is associated with favorable outcomes, the need for revision surgery is not uncommon and may compromise long-term results. When TAAs fail, surgical options include revision arthroplasty, arthrodesis, or in some circumstances, amputation. It is essential for both the surgeon and patient to understand the possible outcomes of revision TAA in order to make an informed decision in the treatment of TAA failure. However, limited studies have explored the differences in outcomes following primary versus revision TAA procedures. The present study aims to address this gap by comparing 5-year surgical complications between primary and revision TAA operations.
Methods:
Patients who underwent primary and revision TAA were identified by CPT codes using a national administrative claims database, which contains over 170 million patients between January 2010 and April 2023. Revision TAA patients were propensity-score matched by age, gender, Charlson Comorbidity Index (CCI) to the primary TAA cohort in a 2:1 ratio. Kaplan-Meier and Cox proportional hazards analyses were used to observe the 5-year cumulative incidence and risk of all-cause revision, periprosthetic joint infection (PJI), mechanical loosening, periprosthetic fracture (PPF), and osteolysis, identified using ICD-9 and ICD-10 diagnosis codes. Results were reported as hazard ratios with 95% confidence intervals.
Results:
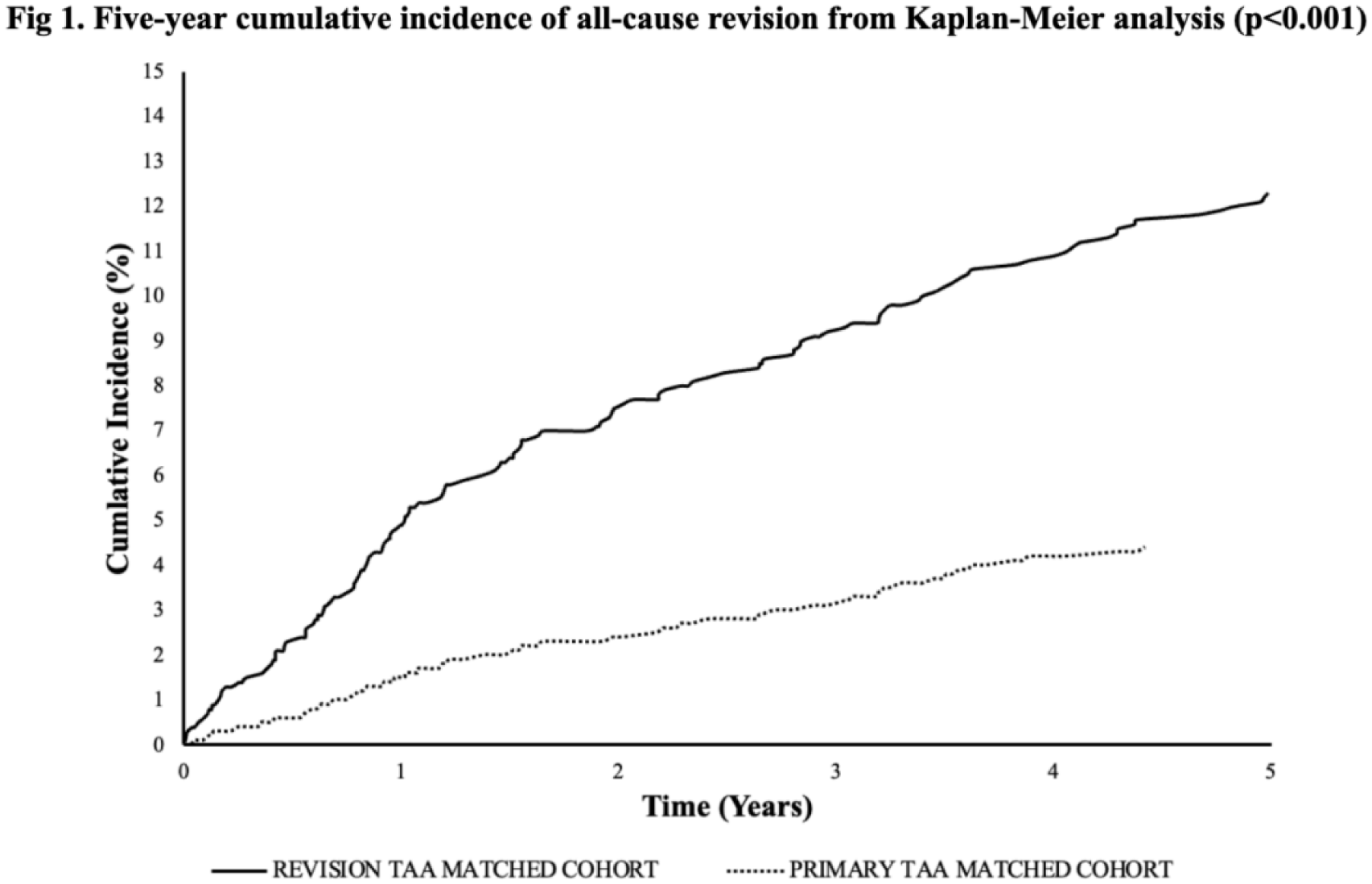
After matching, 3,146 total patients were included in this study: 2,083 in the primary TAA cohort and 1,063 in the revision TAA cohort. Patients undergoing revision TAA have higher 5-year risks of subsequent revision (HR: 17.21; CI: 10.84-27.33; p< 0.001), PJI (HR: 3.46; CI:2.67-4.47; p< 0.001), mechanical loosening (HR: 7.11; CI: 5.21-9.70; p< 0.001), PPF (HR: 2.07; CI: 1.06-4.07; p=0.034), and osteolysis (HR: 6.48; CI: 2.80-14.99; p< 0.001). Fig 1 reveals the cumulative incidence of all-cause revision over 5 years after the index surgery for each cohort.
Conclusion:
This study shows significantly worse 5-year outcomes among patients undergoing revision compared to primary TAA. These findings suggest complication risk increases significantly following revision ankle arthroplasty, emphasizing the importance of preventing causes of revision. This comparative analysis offers valuable insights to guide clinical decision-making and improve patient management strategies.