Abstract
Research Type:
Level 4 – Case series
Introduction/Purpose:
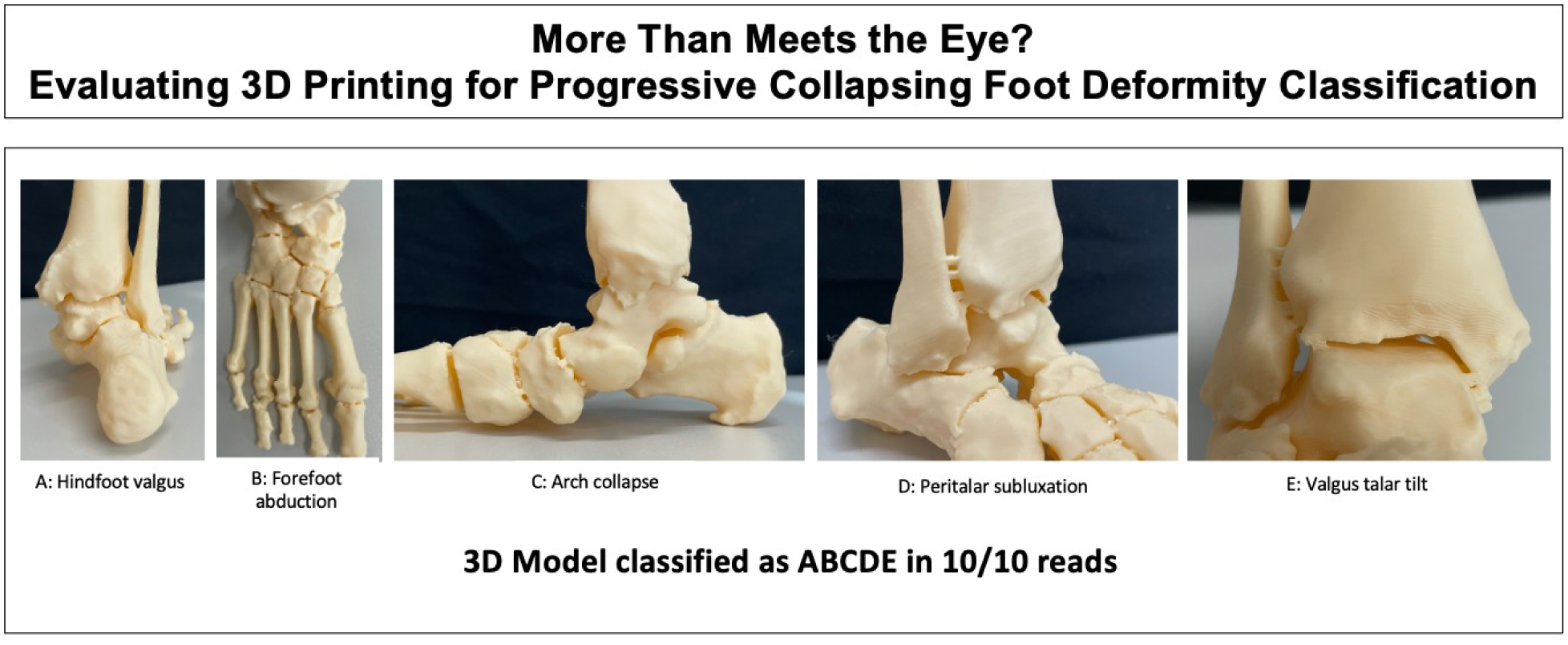
The complex, three-dimensional nature of Progressive collapsing foot deformity (PCFD) makes it difficult to grasp using conventional imaging displays. The new PCFD classification system categorizes deformities into Class A (hindfoot valgus), Class B (midfoot/forefoot abduction), Class C (forefoot varus/medial column instability), Class D (peritalar subluxation), and Class E (valgus talar tilt). Emerging technologies such as Weightbearing CT (WBCT) based 3D printing of patient-specific anatomical models may have the potential to enhance diagnostics by providing improved 3D visualization and a tactile experience. This study aimed to evaluate the inter- and intraobserver reliability of orthopedic foot and ankle surgeons in identifying each PCFD class relying solely on anatomical 3D-printed foot models.
Methods:
Sixty patients (37 female, 23 male; mean age 53 ±17.2 years) who underwent surgical correction of PCFD by a single surgeon were included. Preoperative weightbearing CT (WBCT) scans were semiautomatically segmented, and a 3D reconstruction (as stereolithography model) of each foot was created with linking bars between bones, and subsequently 3D-printed. Five fellowship-trained foot and ankle surgeons independently assessed the models, blinded to clinical data. Without conducting measurements, they identified the presence or absence of PCFD classes A to E solely based on experience and visual-tactile analysis. Staging between flexible and rigid PCFD was not performed due to the presence of connecting bars. After several weeks, the assessments were repeated for a second reading.
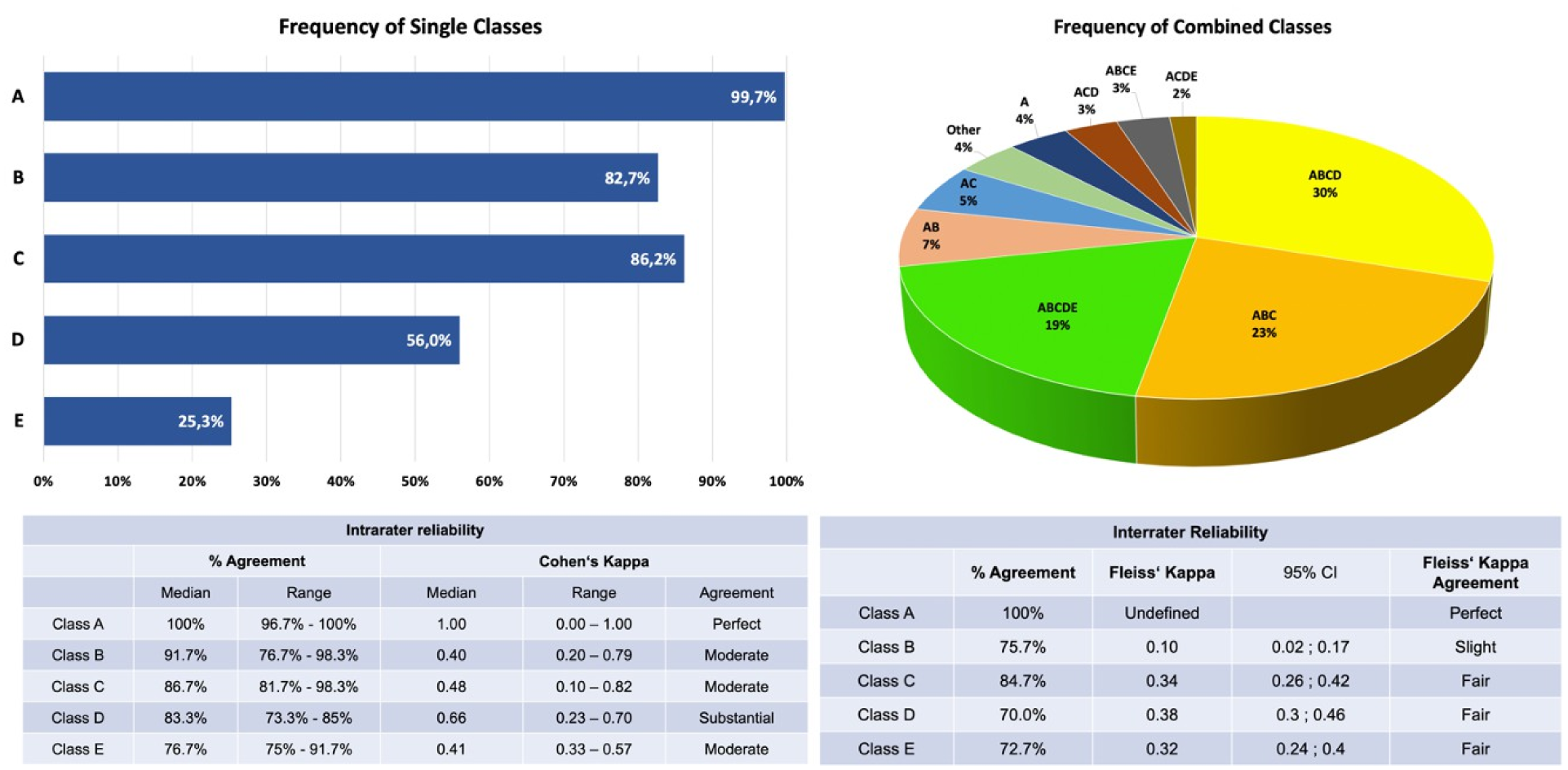
Percentage agreement within and between readers was calculated, and intra- and interobserver reliability for each PCFD class was evaluated using Cohen’s kappa and Fleiss’ kappa, respectively.
Results:
Intrarater reliability varied across PCFD classes. Class A showed perfect agreement (Cohen’s Kappa = 1.00). Other classes had moderate reliability, with Class D being the highest (Kappa = 0.66) and Class B the lowest (Kappa = 0.40). Agreement ranged widely, with Class A showing the highest consistency (96.7% - 100%) and Class E the lowest (75% - 91.7%). Inter-rater reliability also varied. Class A had perfect agreement (100%), making Fleiss’ Kappa undefined. The remaining classes had poor to fair agreement, with Class B showing the lowest reliability (75.7%, Kappa = 0.1).
The most frequently observed class combinations were ABCD (30%), ABC (23%), and ABCDE (19%), while Class A (99.7%) and Class C (86.2%) were the most frequently described single classes.
Conclusion:
This study highlighted the potential of 3D printing for classifying PCFD cases. Inter- and intraobserver reliability varied across classes, with limitations in identifying all deformities solely from 3D-printed models without the WBCT images – an issue not present in the clinical setting. While Class A exhibited perfect agreement, Class B had the lowest kappa values, but still achieved intra- and interrater percent agreements of 91.7% and 75.7%, respectively. 3D printing may serve as a valuable supplement for diagnostics and treatment planning, but further research is needed to determine which model-specific factors influence readers' decisions compared to multiplanar WBCT imaging.