Abstract
Research Type:
Level 3 - Retrospective cohort study, Case-control study, Meta-analysis of Level 3 studies
Introduction/Purpose:
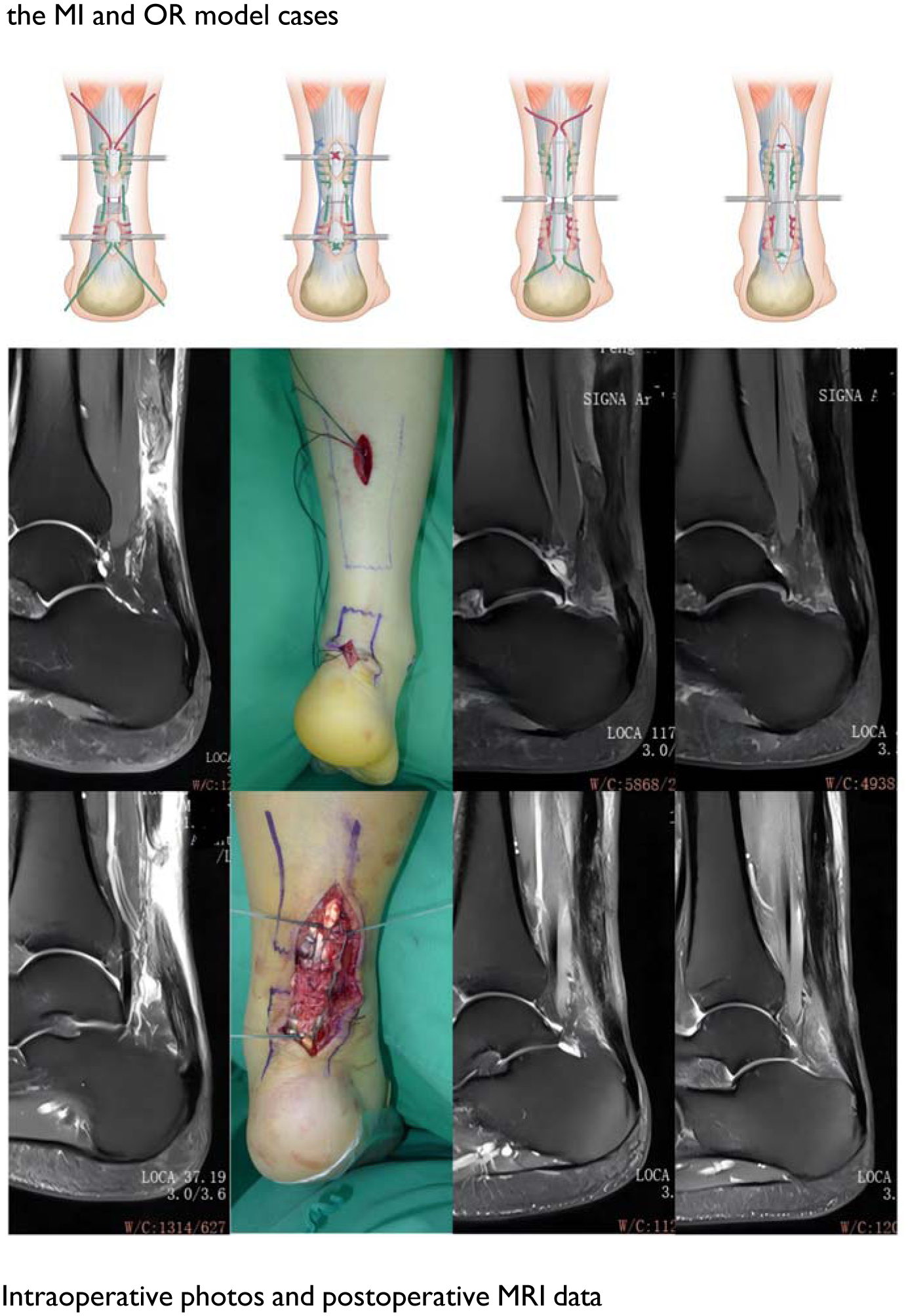
The paratenon, a protective sheath surrounding the Achilles tendon, has been shown to facilitate tendon healing. However, evidence supporting the benefits of paratenon preservation during surgical repair remains limited. This study retrospectively compared the outcomes of a minimally invasive paratenon-sparing technique(locking block modified Krackow) (MI group) versus an open repair technique (OR group) for Achilles tendon ruptures.
Methods:
Patients who underwent surgical treatment for Achilles tendon ruptures at our hospital between January 2015 and August 2021 were included in the analysis. Of these, 61 patients were treated using the minimally invasive paratenon protection technique (MI group), while 67 patients underwent the open repair technique (OR group). Both groups followed the same postoperative rehabilitation protocol. Outcome measures included operation time, complication rates, Achilles tendon length and cross-sectional area (CSA), shear wave elastography (SWE), calf triceps muscle CSA, isokinetic strength, Achilles tendon Total Rupture Score (ATRS), and the Victorian Institute of Sports Assessment–Achilles (VISA-A) score.
Results:
The average follow-up period was 40.0 ± 10.2 months. The MI group demonstrated significantly shorter operation times (P < .001) and lower complication rates (P = .031) compared to the OR group. Additionally, the MI group showed superior outcomes in several key measures: Higher ATRS (P = .015) and VISA-A scores (P = .002), indicating better functional recovery.Greater isokinetic strength at both 60°/second and 180°/second . Improved SWE values, reflecting better tendon elasticity. Larger CSA of the Achilles tendon, suggesting enhanced tendon healing.
Conversely, Achilles tendon extension length was negatively correlated with peak torque at 60°/second (r = -0.309, P < .001) and 180°/second (r = -0.218, P = .013), indicating that longer tendon extension was associated with reduced strength.
Conclusion:
The minimally invasive paratenon protection technique demonstrated superior clinical outcomes compared to the open repair technique. Patients in the MI group experienced shorter operation times, fewer complications, better functional scores, greater isokinetic strength, and improved mechanical properties of the Achilles tendon. These findings suggest that preserving the paratenon during surgical repair may enhance healing and functional recovery, making it a preferable approach for Achilles tendon repair.