Abstract
Research Type:
Level 5 - Case report, Expert opinion, Personal observation
Introduction/Purpose:
Hallux valgus is one of the most common deformities of the foot. More recently, there has been an increase in performing minimally invasive surgery (MIS) for the hallux valgus correction using a distal metatarsal osteotomy and proximal phalanx osteotomy. Many authors have published their MIS results, and the complication rates range from 8 to 18%. Nonunion is rarely described as a MIS bunion complication, with the highest reported nonunion rate being 0.4%. Although there is a low published incidence, the authors have identified a number of cases of nonunion as well as a lack of literature dealing with this complication. We therefore aim to describe our experience with the management of symptomatic nonunion following MIS bunion surgery.
Methods:
A retrospective review was performed using data collected as part of standard clinical care. Four orthopedic centers collaborated on this study: Hospital for Special Surgery (HSS), Wellington Hospital (TWH), Royal National Orthopedic Hospital (RNOH), and Assuta Medical Centre (AMC). At HSS and AMC, MIS surgery is performed, whereas TWH and RNOH manage tertiary referrals from other centers who performed the initial surgery. 1587 primary MIS bunion cases were identified at HSS and AMC, and of those cases, 5 nonunions were noted. The other 12 nonunions were referrals from other centers. Nonunion was defined as symptomatic incomplete healing of the distal metatarsal osteotomy at least six months after surgery. Data collected included age, smoking status, comorbidities, time to nonunion from index surgery, and status of vitamin D deficiency. Surgical approach, type of fixation, type of bone graft if used, complications, and time to union were noted for the revision surgery.
Results:
We identified 17 cases of symptomatic nonunion after MIS bunion surgery. Mean patient age was 47.44, with 53% female. Three patients had comorbidities (two with diabetes, one with Lyme disease), three had low vitamin D at nonunion diagnosis, and three were smokers at time of surgery. All had a CT prior to revision showing nonunion, and no initial infections were noted. Two patients experienced falls with trauma to the operated foot, and one was non-compliant with post-op instructions. Before revision, all patients used bone stimulators. 67% of revisions were open surgery, with bone graft used in 15/17 cases. 14 cases healed completely, and three showed progress on imaging.
Conclusion:
We report 17 cases of nonunion after MIS bunion surgery. The estimated nonunion prevalence is 0.3%, consistent with previous study findings. Risk factors for nonunion include surgical technique, patient comorbidities, low vitamin D, smoking, and medications, though no clear risk factors were identified in our series. Thermal bone necrosis from MIS burr heat may contribute to nonunion, highlighting the importance of irrigation and avoiding tourniquets.
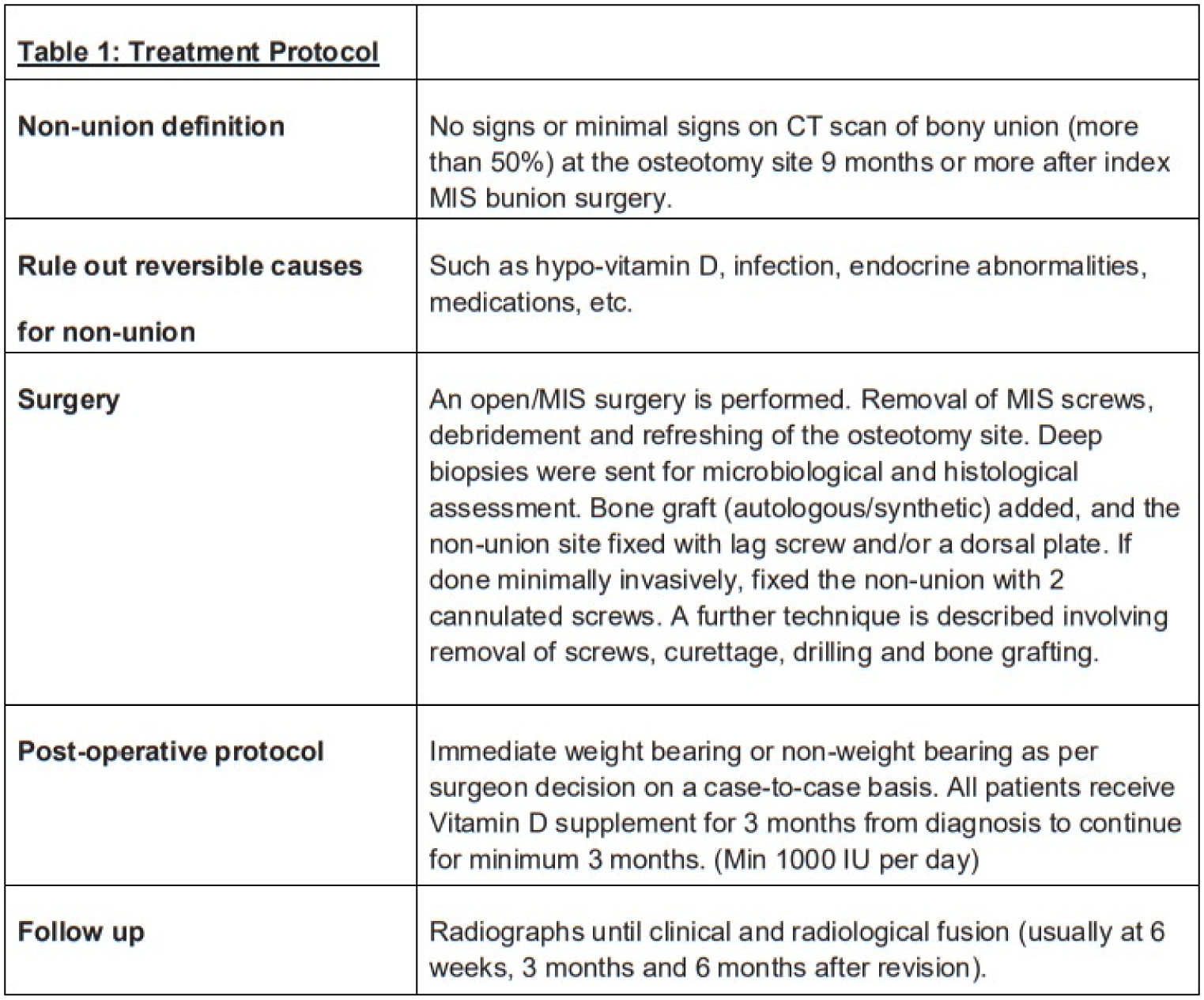
The union rate after revision was 83%, with an average time to union of 11 weeks. This study offers a preliminary protocol for managing symptomatic non-union, addressing a rare but challenging complication.