
Abstract
Research Type:
Level 3 - Retrospective cohort study, Case-control study, Meta-analysis of Level 3 studies
Introduction/Purpose:
Over 10% of patients remain dissatisfied following hallux valgus (HV) surgery, which may be related to recurrence of the deformity. While the original Lapidus procedure included medial-middle (C1-C2) intercuneiform and first and second metatarsal base stabilization, the procedure has been modified to include only arthrodesis of the first TMT joint. However, Kim et al. (Foot and Ankle International 2024) reported a recurrence rate of 17.3% following a modified Lapidus procedure with no intercuneiform fixation (NS) and found an association between C1-C2 joint widening with a higher rate of HV recurrence. This study aims to identify whether the addition of an intercuneiform screw (ICS) from the base of the first metatarsal to C2 to a first TMT arthrodesis reduces HV recurrence and minimizes C1-C2 joint gapping.
Methods:
This retrospective comparative cohort study analyzed HV patients who underwent a modified Lapidus procedure, using data from a prospectively collected foot and ankle registry. A total of 171 patients were identified, of which 18 (11%) were male and 153 (89%) were female. Patients were categorized by screw fixation: 87 (51%) in the group without intercuneiform fixation (NS) and 84 (49%) in the intercuneiform screw (ICS) group. Otherwise, the surgical technique was similar between the groups. The primary outcome was HV recurrence, defined as a postoperative hallux valgus angle (HVA) exceeding 20° as previously defined in the literature (Park and Lee J Bone Joint Surg Am 2017). Preoperative and postoperative radiographic measurements including HVA, intermetatarsal angle (IMA), C1-C2 distance, sesamoid position, and first TMT pronation of the first ray were analyzed using coronal multiplanar reconstructed weight-bearing CT (WBCT) images to assess C1-C2 joint gapping.
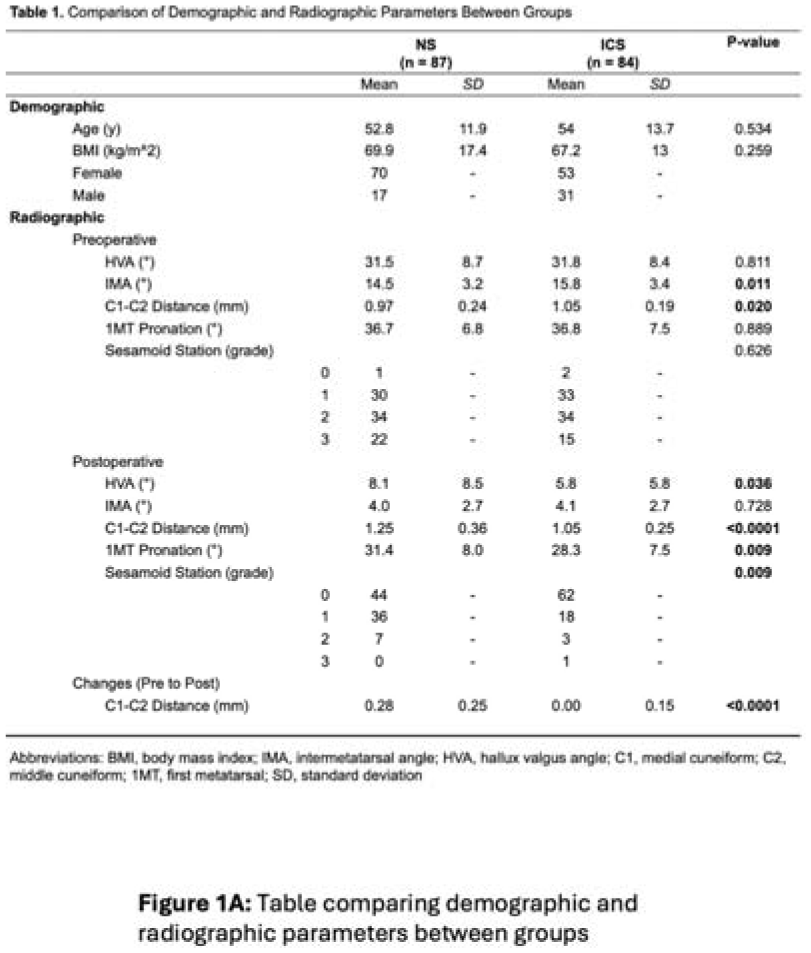
Results:
Mean ages were 52.8 years for the NS group and 54.0 years for the ICS group (p=0.534). Recurrence occurred in six of 87 (7%) NS patients, but none in the ICS group (p=0.029). Preoperative HVA was similar between groups but was lower postoperatively in the ICS group (p=0.036). IMA was higher preoperatively for the IS group (p=0.011), though it did not differ postoperatively (Table 1). C1-C2 joint distance in the ICS group was significantly higher preoperatively (p=0.020) and lower postoperatively (p < 0.001). Change in intercuneiform gapping was significantly reduced in the ICS group (p < 0.001). Postoperative first TMT pronation and sesamoid station were both lower in the ICS group (p=0.009; p=0.009).
Conclusion:
Our findings suggest that an additional first metatarsal base - C2 screw fixation reduces recurrence and decreases C1-C2 joint gapping in the modified Lapidus procedure. Additionally, patients with stabilization across the intercuneiform joint had improved first metatarsal pronation and sesamoid reduction compared with patients who did not have a screw from the first metatarsal base to C2. These results suggest that stabilization of the intercuneiform joint may improve HV deformity correction. However, further research on failure rates and patient-reported outcomes (PROMIS) is needed to evaluate long-term clinical efficacy.


Comparison of Intercuneiform C1-C2 Stability Between NS and ICS Fixation Techniques
This figure presents a radiographic and WBCT Analysis comparing C1-C2 joint stability between NS and ICS fixation techniques. It illustrates differences in preoperative and postoperative joint distance, percent change distribution, and the stabilizing effect of the additional intercuneiform screw (ICS).