Abstract
Research Type:
Level 2 - Prospective comparative study, Meta-analysis of Level 2 studies or Level 1 studies with inconsistent results
Introduction/Purpose:
Numerous surgical procedures have been described for correction of a hallux valgus deformity. Minimally invasive chevron akin (MICA) hallux valgus correction has gained increased interest as it may result in improved pain scores, increased patient satisfaction, earlier rehabilitation, and less scarring, while remaining an effective surgical treatment. However, there have been concerns regarding heat generation from the percutaneous burr resulting in possible thermal necrosis of bone. The primary aim of this study is to determine if tourniquet use impacts internal temperature of the first metatarsal during MICA hallux valgus correction. The secondary aim is to determine the change in temperature of the first metatarsal caused by the osteotomy.
Methods:
Female patients 40-60 years old indicated for MICA hallux valgus correction during routine clinical care who elected to undergo the procedure independent of study participation were eligible for the study. Patients who required concurrent forefoot procedures could participate, however, the MICA was performed first. Patients who had a prior ipsilateral forefoot surgery were excluded. Patients were randomized to surgery with or without a tourniquet. Multiple temperature measurements were obtained using a sterile temperature probe. A starting temperature was measured after incision prior to use of the burr. Temperature of the first metatarsal was then measured after the pilot hole was made, after the dorsal osteotomy was completed, and both 30 and 60 seconds after the osteotomy. The surgery was performed by one of two senior surgeons using the same burr system. A t-test was used to compare differences between the two groups. Statistical significance was set at P < 0.05.
Results:
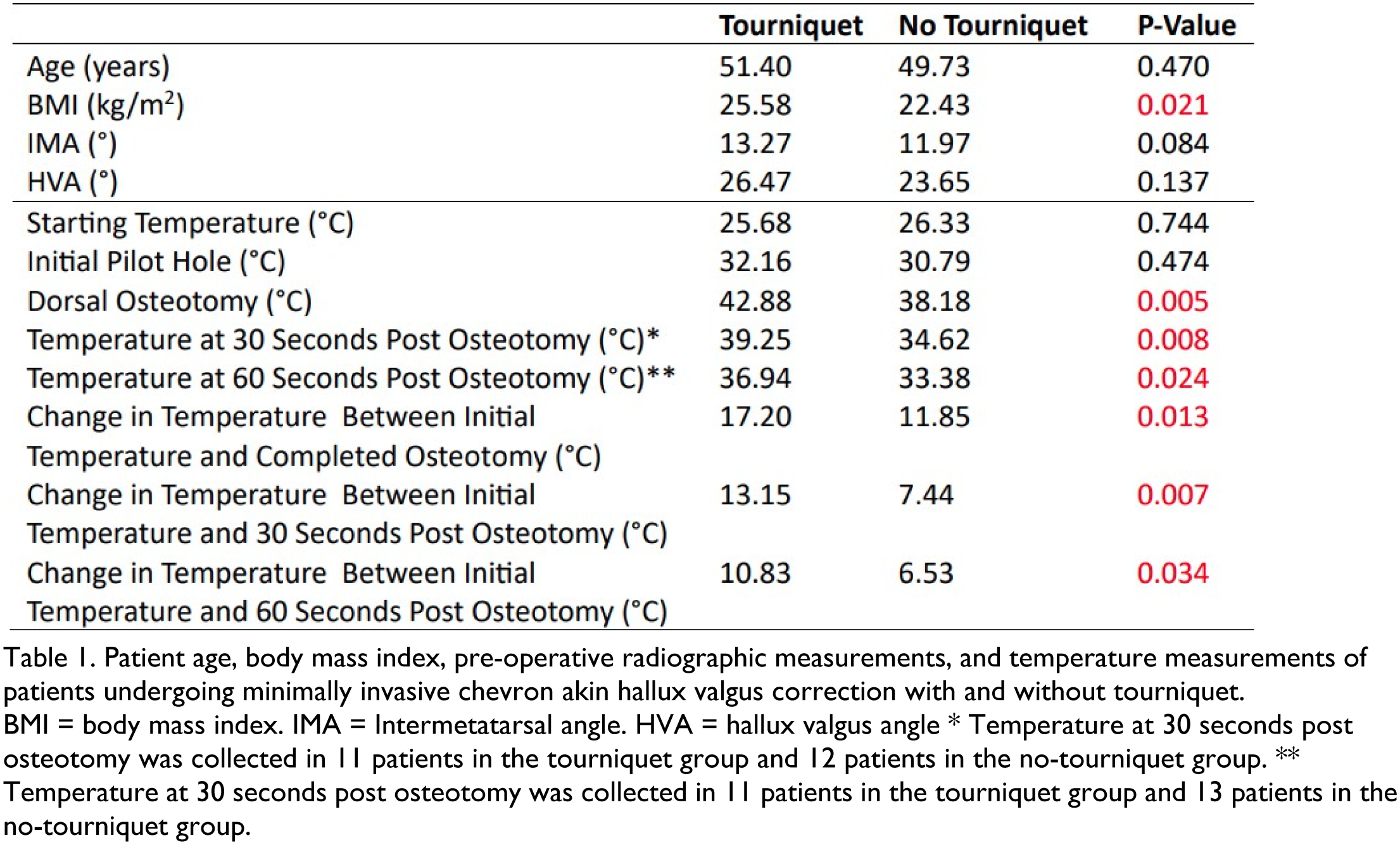
There were 15 patients per study arm. Baseline characteristics were similar between the two groups, however, there was a statistically significant difference in body mass index despite randomization (Table 1;p=0.021). There was no significant difference regarding the average start temperature (tourniquet 25.68 °C versus no tourniquet 26.33°C; p=0.744) or temperature after the pilot hole (32.16°C versus 30.79°C; p=0.474). There was a statically significant difference between the groups after completion of the dorsal osteotomy (42.88°C versus 38.18°C; p=0.005), 30 seconds later (39.25°C versus 34.62°C; p=0.008), and 60 seconds later (36.94°C versus 33.38°C; p=0.024). This held true at all time points for the change in temperature from the index measurement as well (Table 1). Both groups had the same maximum temperature (45°C) after the dorsal osteotomy.
Conclusion:
The results of this study are the first to assess the impact of tourniquet use on the temperature of the first metatarsal during the chevron osteotomy when performing a MICA hallux valgus correction. Our study showed a statistically significant difference in both the absolute and change in temperature of the first metatarsal between the groups at completion of the osteotomy and at 30 and 60 seconds after completion of the osteotomy. Of note, neither group appeared to reach temperatures consistent with thermal necrosis of bone as previously reported in the literature.