Abstract
Research Type:
Level 3 - Retrospective cohort study, Case-control study, Meta-analysis of Level 3 studies
Introduction/Purpose:
Gender disparities persist in the surgical workforce, with orthopedics projected to reach gender parity only by 2236. The foot and ankle subspecialty presents a unique opportunity to examine disparities across both orthopedics and podiatry. Recent studies document persistent payment gaps in procedural specialties, but few have directly compared reimbursement patterns in competing specialties treating identical conditions. This study aims to: (1) characterize Medicare reimbursement patterns between genders in foot and ankle surgery across orthopedics and podiatry; (2) identify geographic and temporal variations in these reimbursements; and (3) evaluate differences in practice patterns, procedural complexity, and patient population characteristics that may contribute to these disparities.
Methods:
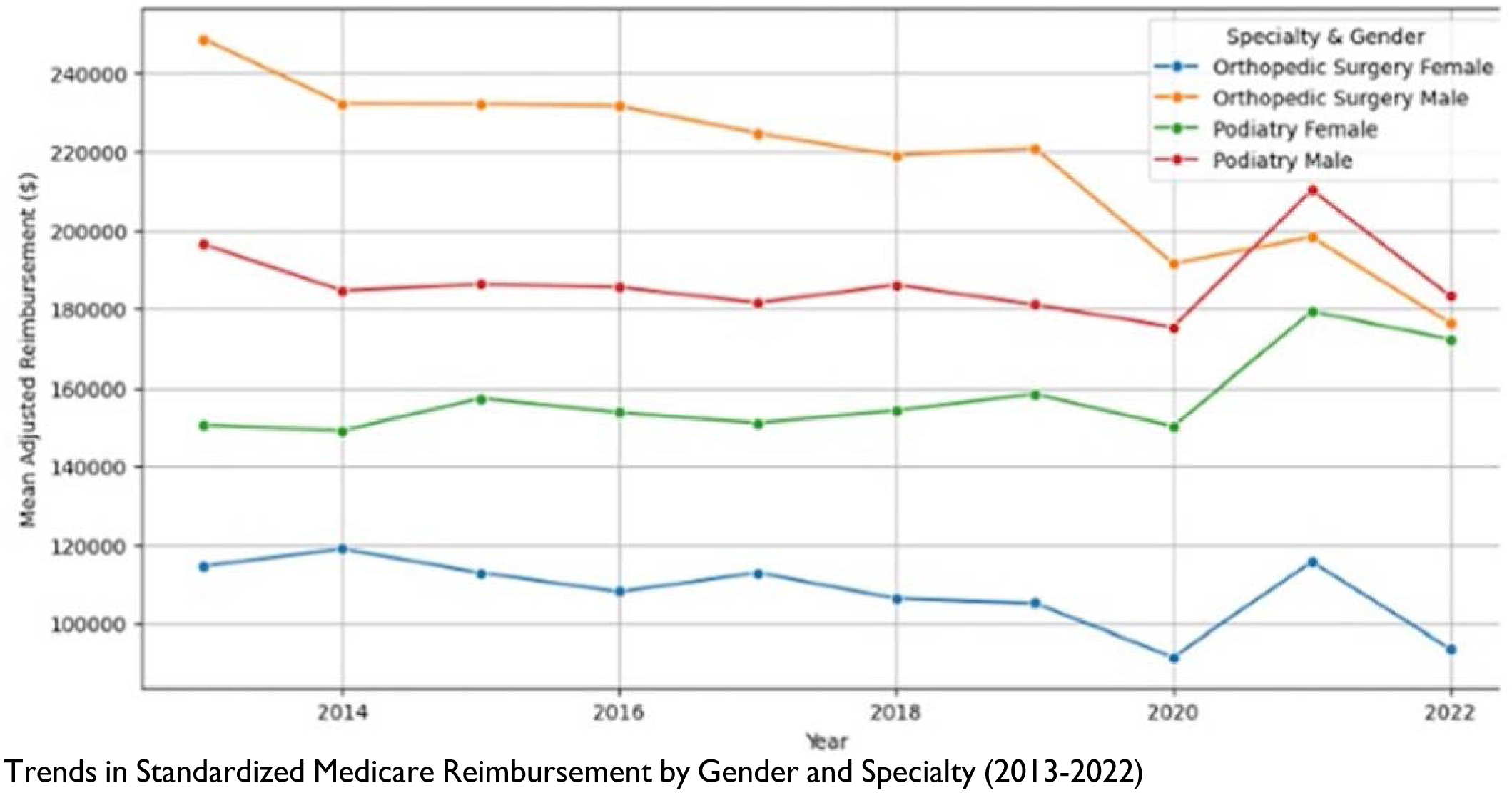
We performed a comprehensive retrospective analysis of Medicare Fee-for-Service Provider Utilization and Payment data (2013-2022) filtered by foot and ankle procedural codes. Individual providers were identified using National Provider Identifiers and cross-referenced with CMS Physician Compare data to determine gender, specialty, years in practice, and practice location. We excluded group practices, collaborative clinics, and providers with fewer than 11 annual services to ensure data integrity. Reimbursement values were standardized to 2022 dollars using healthcare-specific Consumer Price Index adjustments. We analyzed procedure diversity using unique CPT codes, procedural complexity by relative value units, and patient complexity using Hierarchical Condition Category (HCC) risk scores. Multivariable linear regression models accounting for geographic clustering were used to isolate gender-based reimbursement differences, controlling for practice volume, patient demographics, and years in practice.
Results:
Among orthopedic surgeons, 8.9% were female (105/1184) versus 10.7% in podiatry (339/3173). Male providers earned significantly more than female providers across all geographic regions (p < 0.001). Female providers were concentrated in the South (orthopedics: 38.3%, podiatry: 41.8%) and served higher-risk patients (Hierarchical Condition Category score: 1.58 vs. 1.52; p=0.0063) but billed fewer unique CPT codes and performed fewer complex procedures. The reimbursement gap widened with experience, becoming significant after 5 years in practice for both specialties (orthopedics: p< 0.001, podiatry: p=0.0027).
Conclusion:
This study highlights significant gender and specialty disparities in reimbursement and workforce representation. Geographic disparities underline the importance of tailored recruiting and retention models. This discrepancy could be because female providers with equal training and seniority received fewer new patient referrals. Reforms should aim to address systemic inequalities in reimbursement workforce distribution and patient referrals. Academic institutions should strengthen female faculty recruitment, ensure equitable promotion efforts and improve female medical student mentorship. Outreach initiatives should be implemented to broaden the training pipeline and enhance diversity in orthopedic surgery and podiatry.