Abstract
Research Type:
Level 4 – Case series
Introduction/Purpose:
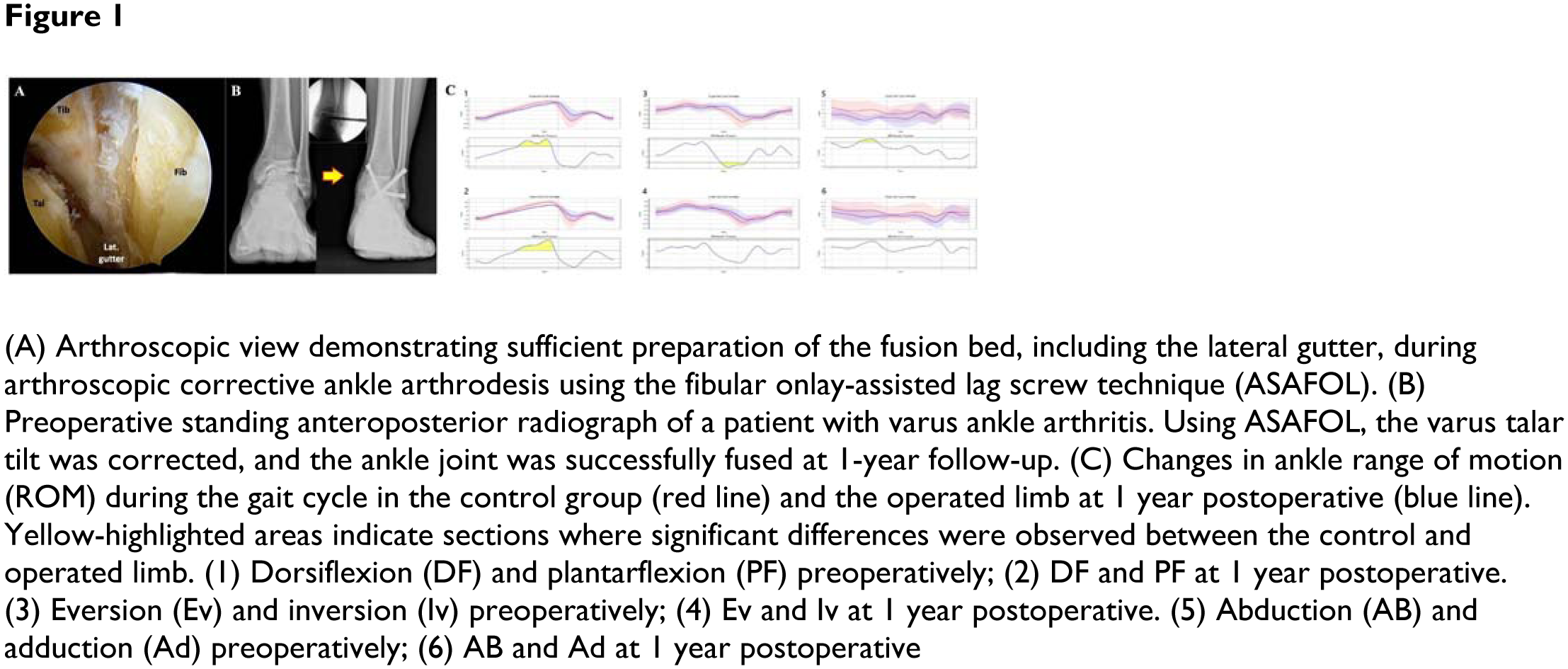
Ankle arthrodesis (AA) is a well-established surgical option for painful advanced ankle arthritis, with various approaches and fixation methods available. The fibular onlay grafting technique, performed through an open lateral approach, has demonstrated favorable outcomes by providing lateral stability. Meanwhile, arthroscopic AA has gained popularity with advancements in techniques and instrumentation. To combine the advantages of both techniques, we introduce arthroscopic corrective ankle arthrodesis using a fibular onlay-assisted lag screw technique (ASAFOL) (Figure 1A, 1B). While multiple systematic reviews and meta-analyses have compared open versus arthroscopic AA, most have focused on fusion rates and clinical outcomes. However, assessing gait function recovery is equally important in evaluating surgical success. This study aims to assess the surgical outcomes of ASAFOL using conventional scoring systems and gait analysis.
Methods:
From December 2022 to October 2023, ASAFOL was performed on seven patients. Clinical outcomes were assessed using the VAS, FAAM, LEFS, AOFAS ankle-hindfoot scale, and Karlsson scale. Real-time gait analysis was conducted using deep learning-assisted markerless motion capture software (Remobody-S, Remo Inc., South Korea) integrated with the HuMoR architecture. Gait analysis was conducted preoperatively and 1 year postoperatively to evaluate changes in ankle range of motion (ROM) during the gait cycle. Statistical parametric mapping was used to compare pre- and postoperative ROM with those of a normal control group (n=20). Nine gait parameters were analyzed, including gait speed, cadence, step length, stance phase, swing phase, double support phase, opposite heel strike, cycle duration, and step width. Clinically significant differences between operated and non-operated limbs were assessed using Bland-Altman analysis, with 95% CI. Differences exceeding this interval indicated a limping gait.
Results:
Clinical scores improved across all measures except for the FAAM-Sports subscale. Preoperative ankle ROM during the gait cycle showed statistically significant differences from normal ROM in certain phases across all three axes (sagittal, coronal, axial). Postoperatively, these differences were no longer significant (Figure 1C). However, due to arthrodesis, plantarflexion remained restricted during the terminal stance phase. At 1 year postoperative, no significant differences were observed in nine gait parameters between patients and the normal control group. Similarly, no clinically significant differences in these parameters were found between the operated and non-operated limbs.
Conclusion:
ASAFOL demonstrated improvements in functional outcomes and partial normalization of ankle ROM during gait, despite the inherent restrictions of arthrodesis. At 1 year postoperative, no significant differences were observed in nine gait parameters between patients and normal controls. Additionally, no clinically significant differences were found between the operated and non-operated limbs, indicating that ASAFOL effectively restores gait symmetry. These findings suggest that ASAFOL is a viable technique for achieving both structural stability and functional recovery in patients with advanced ankle arthritis requiring arthrodesis.