
Abstract
Research Type:
Level 4 – Case series
Introduction/Purpose:
Triple arthrodesis is a common surgical treatment for several types of arthritic patterns and deformity including progressive collapsing foot deformity (PCFD), cavovarus deformity, and Charcot arthropathy.
Many patients who undergo triple arthrodesis may also have— or later develop—concomitant tibiotalar joint deformity and/or arthritis. However, the effect on tibiotalar deformity (specifically talar tilt) after triple arthrodesis is not well studied. Our hypothesis is that in a series of patients undergoing triple arthrodesis, PCFD patients would have the largest change in talar tilt at final follow up.
Methods:
A retrospective case series was performed from January 2017 to December 2023 identifying all patients that underwent triple arthrodesis. 115 procedures with greater than 6 months of follow up were included. Those excluded did not have weight bearing radiographs, had prior or concomitant ankle fusion or replacement, or were revision cases. Demographics and diagnoses were collected. Median age was 65.4 (SD 12.67) and mean postoperative follow up was 11.9 months (SD 8.13). Diagnoses treated included PFCD (74 patients), cavovarus deformity (12), arthritis (13), Charcot (9), other (7). Talar tilt and lateral talus-1st metatarsal angle (Meary’s angle) were measured on weight-bearing radiographs at three time intervals: 1) preoperatively, 2) the first postoperative radiograph, and 3) final follow-up. The primary outcome was radiographic change in talar tilt and Meary’s angle from preoperative to final postoperative follow-up. Secondary outcomes measured were rate of subsequent ankle arthrodesis or arthroplasty and need for revision surgery.
Results:
Change in talar tilt by diagnosis can be found in Table 1. Patients with PFCD had a median preoperative talar tilt of 0.9 degrees (IQR 2.1) and a median change in talar tilt after triple arthrodesis of 1.8 degrees (IQR 3.1) at final follow up. The median preoperative Meary’s angle in the PFCD group was 23.3 degrees (IQR 16.1), and the median change in Meary’s angle was -13.8 degrees (IQR 14.22). 3 ( 2.6%) patients underwent planned staged triple arthrodesis followed by ankle fusion or replacement, and 6 (5.2% ) subsequently underwent ankle arthrodesis or arthroplasty due to the development of symptomatic ankle arthritis or deformity. Zero patients underwent a revision triple arthrodesis.
Conclusion:
Valgus talar tilt increased after triple arthrodesis most substantially in patients with PFCD. However, only few became symptomatic enough to require surgical intervention to address tibiotalar arthritis or deformity. These data can be used by surgeons to educate their patients both pre and post operatively and informs the need for surveillance weight-bearing ankle radiographs following triple arthrodesis. Further studies may consider how over or undercorrection of foot deformity longitudinally effects valgus tilt especially in the setting of PFCD.
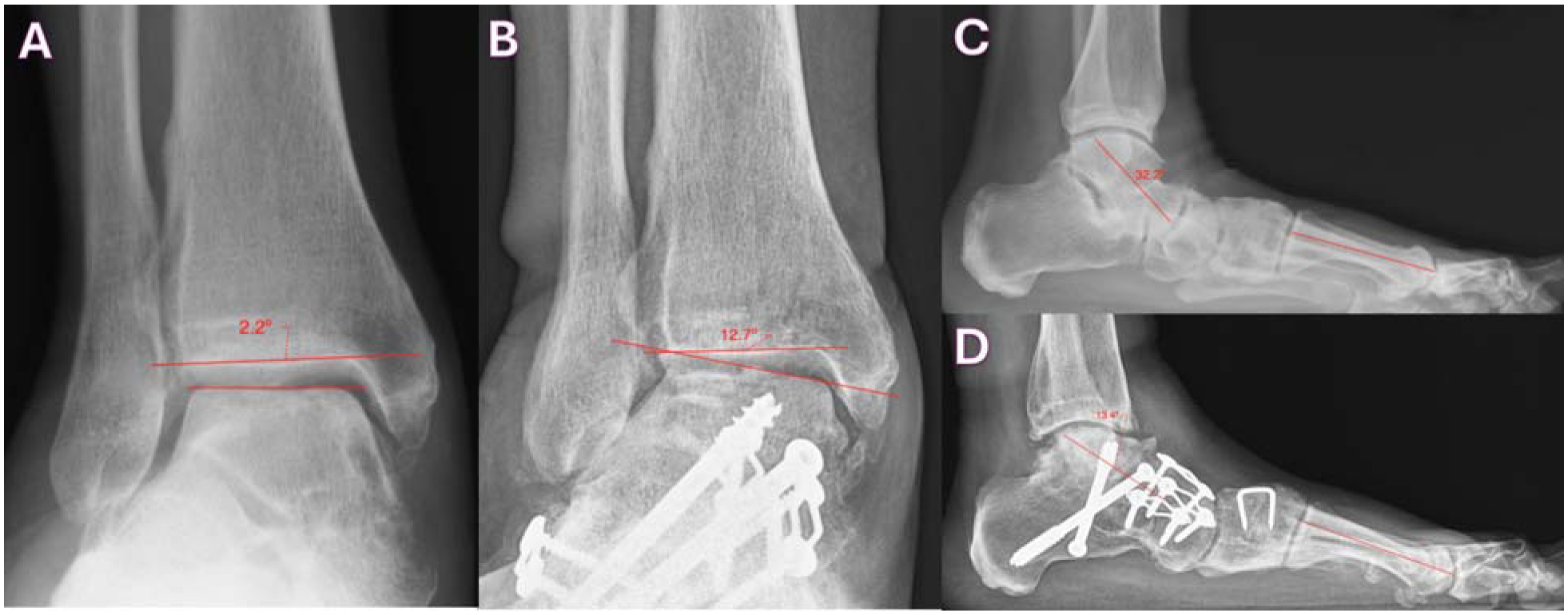
Figure 1
Talar tilt measurement on weight bearing radiographs at A) preoperative and B) 16 months postoperative follow up, and Meary’s angle measurement at C) preoperative and D) 16 months postoperative follow up.