Abstract
Research Type:
Level 3 - Retrospective cohort study, Case-control study, Meta-analysis of Level 3 studies
Introduction/Purpose:
Tourniquet use during surgery has been thought to yield shorter operating times, reduced bleeding, diminished total blood loss, and enhanced visibility and surgical precision. Despite these proposed benefits, tourniquet use has been linked to complications including nerve damage and postoperative pain. Therefore, an increase in pain following tourniquet use could potentially lead to increased opioid use postoperatively. Additionally, various anesthesia types including regional anesthesia use have the potential to affect postoperative pain and therefore opioid consumption. The purpose of this study was to assess if tourniquet use and anesthesia type are associated with increased postoperative opioid consumption after open reduction and internal fixation (ORIF) surgery of tibial plafond (pilon) fractures.
Methods:
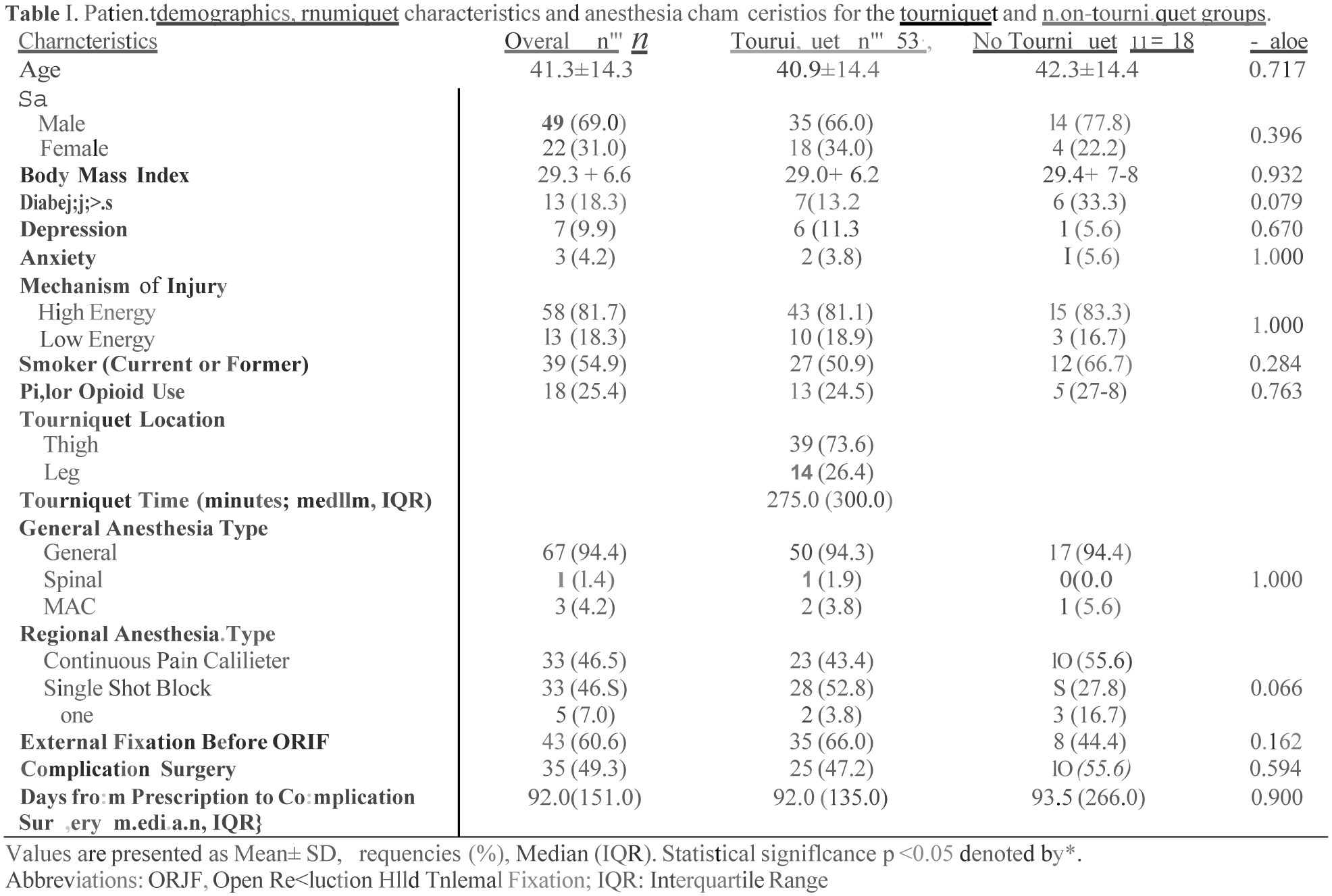
A retrospective chart review at a level one trauma center was conducted using Current Procedural Terminology codes to identify patients with isolated pilon fractures who underwent open reduction and internal fixation surgery from January 2019 to June 2023. Patient demographic data, tourniquet use, location, and inflation time, anesthesia type, regional anesthesia use/type, and ambulatory opioid prescriptions converted to morphine milligram equivalents (MME) were collected. Prescriptions were tracked from discharge until prescription cessation or complication surgery. Polytrauma patients and patients under 18 years old were excluded. Independent T-test, Mann-Whitney U test, and Fisher’s exact test were used as appropriate. A multiple linear regression model was employed with the natural logarithm of MME as the dependent variable for both the tourniquet and non-tourniquet groups and the tourniquet-only group to achieve normality and constant variance assumptions. A significance level of < 0.05 was used to determine statistical significance.
Results:
The regression model (n = 71) demonstrated a poor overall fit (R2 = 0.13), suggesting that only 13% of the variance in log-transformed MME is explained by the model. The F-statistic was 1.016 (p = 0.438) indicating that the model was not statistically significant overall. Thus, the model did not effectively clarify the relationship between MME and key predictors. While the analysis suggested possible associations – such as higher MME in males, a history of prior opioid use, and the presence of a tourniquet – these findings were not statistically significant. Similarly, a regression analysis of the tourniquet-only group (n = 53) also yielded a poor model fit (R2 = 0.13) with no statistically significant associations including between MME and tourniquet location or inflation time.
Conclusion:
The results of this study demonstrated no significant association between tourniquet use or anesthesia type and ambulatory opioid consumption after ORIF of pilon fractures. Tourniquet location and inflation time, general anesthesia type, and regional anesthesia use/type were all not significantly associated with increased post-discharge opioid use. These findings can therefore support surgeon preference for tourniquet and anesthesia use during isolated pilon fracture surgeries.