
Abstract
Research Type:
Level 3 - Retrospective cohort study, Case-control study, Meta-analysis of Level 3 studies
Introduction/Purpose:
The development of primary osteoarthritis (OA) in the ankle is rare, with the majority of cases being post-traumatic in nature. Despite this, the specific injuries that predispose individuals to post-traumatic OA (PTOA) and the timeframe between initial trauma and symptomatic end-stage ankle OA remain unclear. This ongoing multicenter retrospective study aims to identify the specific injuries that lead to PTOA in the ankle, as well as to determine the time course between initial trauma, symptom development, and the need for definitive treatment.
Additionally, the study seeks to investigate how patient-specific factors such as BMI, gender, and age may influence the risk of developing end-stage ankle OA.
Methods:
In this retrospective multicenter cohort study, we identified all patients with end-stage ankle osteoarthritis (OA) who underwent ankle arthrodesis (AA) or total ankle replacement (TAR) at five tertiary medical centers by reviewing electronic medical records and using CPT codes. Patients with prior foot/ankle fusions or adjacent subtalar fusion (tibiotalocalcaneal) were excluded from the study. Ankle OA causes were categorized broadly into idiopathic (primary), secondary (hindfoot deformity, rheumatoid arthritis, haemophiliac / hemochromatosis, septic, congenital, avascular necrosis, Charcot arthropathy), or post-traumatic groups based on medical record review. For cases of ankle post-traumatic OA, radiographs of the initial injury films were obtained when available. Additional data extracted from medical records included the time elapsed between injury and the initial presentation of end-stage ankle OA symptoms, as well as the timing of final treatment with AA or TAR.
Results:
Of 2001 total patients included, 57.3% were male, 42.7% female. Mean age was 46 years at time of injury and mean BMI was 32.2kg/m2. In this cohort, 66% percent underwent TAR and 33.4% AA. Additionally, 54.4% had PTOA, 30.1% primary OA, and 13.5% secondary OA. Ankle fractures or recurrent ankle sprains accounted for 67.3% of PTOA cases (Table 1). Mean time to clinic presentation amongst cases involving ankle fracture was 14.4 years.
Average time between injury and TAR/AA was 18.5 years overall, versus PTOA was 16.6 years. Mean age at TAR/AA was 62 years for primary/secondary OA and 59 years for PTOA. Patients who sustained previous pilon fractures were more likely to receive AA (62.8%), while ankle fractures were more likely to undergo TAR (68.5%).
Conclusion:
This multicenter retrospective study provides valuable insights into the development of ankle PTOA. The findings suggest that ankle fractures and recurrent ankle sprains are the primary injuries predisposing individuals to PTOA, with an average time of 14 years between initial trauma and symptomatic end-stage ankle OA. Patients sustaining pilon fractures were more likely to undergo fusion compared to patients who sustained rotational ankle fractures. Furthermore, this study highlights the influence of patient-specific factors such as age, BMI, and injury type on the risk of developing PTOA. Our findings can improve the understanding and management of patients with end-stage ankle OA.
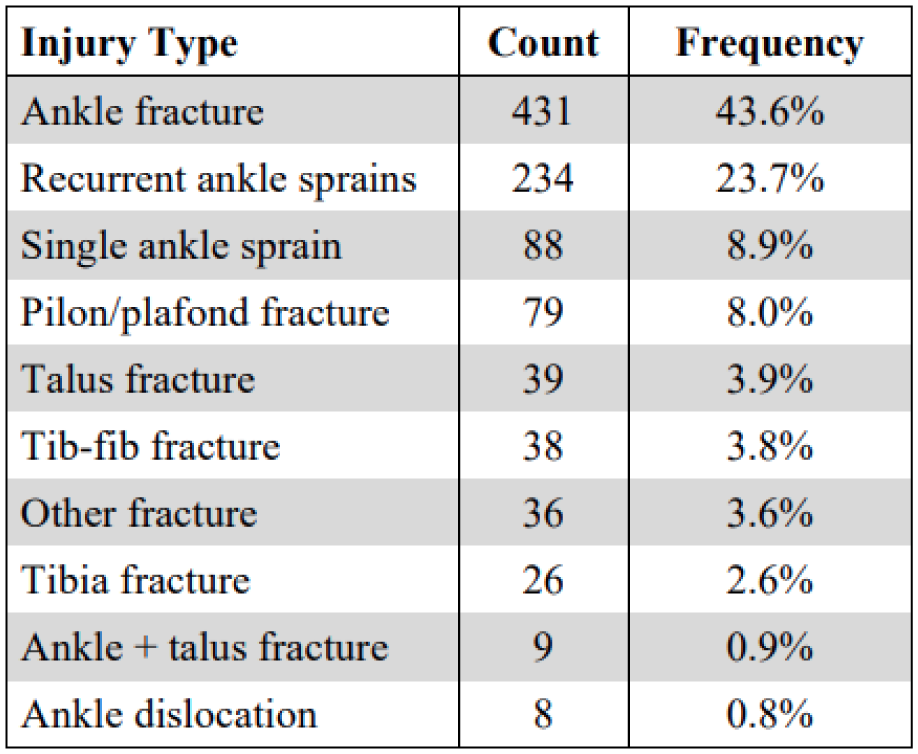
Table 1. Distribution of injuries within post-traumatic OA cases