
Abstract
Research Type:
Level 2 - Prospective comparative study, Meta-analysis of Level 2 studies or Level 1 studies with inconsistent results
Introduction/Purpose:
Charcot Neuroarthropathy (CNA) is a progressive and destructive joint condition resulting from a combination of peripheral neuropathy and repeated microtrauma. Non-surgical interventions alleviate pressure from the joint and are the primary treatment option for early stages of CNA. Delaying treatment can result in foot deformities, ulceration, infection and amputation. Understanding the relationship between gait kinematics and plantar pressure distributions of CNA patients may provide useful information in staging and management. 3D gait analysis technology for diagnosing and assessing gait abnormalities exists, but it is often inaccessible and costly. The aim of this study was to assess plantar pressures and two-dimensional kinematics of CNA patients during gait analyses. Four cohorts were compared (1) affected and non-affected limbs, (2) CNA patients and healthy controls.
Methods:
Following institutional review board approval, the study was conducted at a single institution using a case-controlled prospective selection of patients treated by two orthopaedic foot and ankle surgeons from June 2024 – December 2024. Fourteen patients diagnosed with CNA (n=14) and eleven control patients (“Healthy”) were placed in a diabetic slipper with F-64 TEKSCAN insole matrix system sensors. Adhesive-colored markers were placed on their greater trochanter, lateral knee, lateral malleolus, and distal fifth metatarsal. Using a handrail, participants walked at 0.6 mph and 1.0 mph on a treadmill. Maximum mean force as well as the percentage contribution of each discretized region: (hindfoot, midfoot, metatarsals and forefoot) were analyzed and normalized to the participant bodyweight. Angular range of motions (ROM) of the hip, knee, and ankle joints were measured. Two comparisons were made using the data: (1) Affected limb versus non-affected contralateral limb, (2) CNA patients vs control data.
Results:
Gait analysis was successful for all participants at both speeds. Hindfoot and metatarsal forces were significantly lower in CNA patients compared to controls for both speeds (p < 0.000001 and p < 0.01, respectively) (Fig. A,B). Midfoot forces were significantly higher in CNA patients compared to controls at both speeds (p = 0.002). There were no statistically significant differences between forefoot forces in CNA and controls at either speed. There were no statistically significant differences between affected and contralateral limbs of CNA patients. (Fig. C,D). On kinematic analysis, knee range of motion was significantly lower in CNA patients than controls (p < 0.00001) at 1.0 mph whereas there were no significant differences measured with the other two joints (Fig. E).
Conclusion:
Gait pattern abnormalities were observed in participants with CNA at both walking speeds. Greater midfoot plantar forces recorded for CNA patients highlight a common consequence of CNA, midfoot collapse. This is also evidenced by decreased plantar forces of the hindfoot and metatarsals of the CNA patients compared to controls. This data in combination with a decreased ROM of the knee joint reiterate the benefits of performing both gait analysis and collecting plantar force data to better categorize and treat patients with CNA. Future directions include creating specific devices to help mitigate higher midfoot pressures within the CNA population.
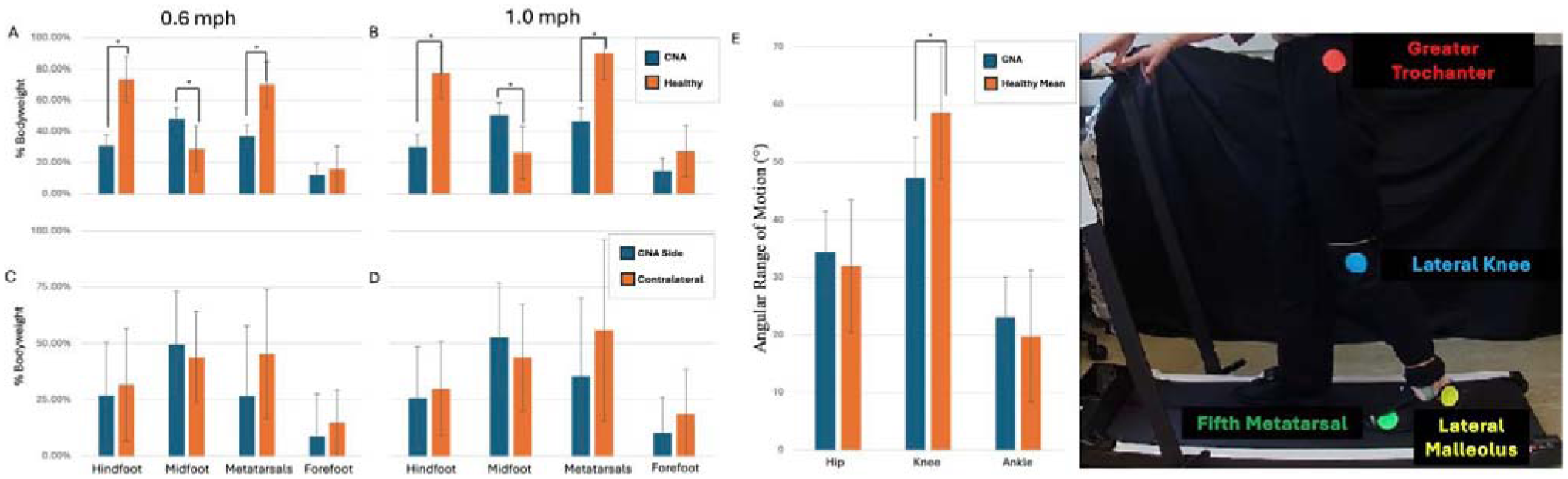
Figure 1: Plantar Force results for each region of interest including comparisons of bilateral mean CNA patient forces versus healthy controls (A-B) and the CNA affected limb versus the contralateral (C-D). The mean angular range of motion on 2D gait analysis of affected limb of CNA patients versus the mean healthy control. Error bars indicate + standard deviations, * indicate p<0.05.