
Abstract
Research Type:
Level 3 - Retrospective cohort study, Case-control study, Meta-analysis of Level 3 studies
Introduction/Purpose:
Concomitant flatfoot deformity is common in hallux valgus (HV) patients and may contribute to its development and recurrence. While symptomatic flatfoot is typically addressed with additional procedures during HV correction, treatment for asymptomatic flatfoot remains unclear. Previous studies have examined the impact of asymptomatic flatfoot on outcomes following HV correction using a Lapidus procedure or a minimally invasive chevron and Akin (MICA) bunionectomy. Both studies found no significant postoperative differences in radiographic and patient-reported outcome scores (PROMIS) between patients with and without asymptomatic flatfoot. However, no direct comparison has been made between the two surgical approaches in asymptomatic flatfoot patients. This study aims to compare postoperative changes in radiographic measures and PROMIS scores between the Lapidus procedure and MICA bunionectomy in asymptomatic flatfoot HV patients.
Methods:
This retrospective comparative cohort study identified HV patients who underwent either open Lapidus or MICA bunionectomy, using a prospectively collected foot and ankle registry. Asymptomatic flatfoot was defined by radiographic criteria for flatfoot, but no existing clinical symptoms of collapsing flatfoot. Radiographic flatfoot was defined by a Meary’s angle greater than four degrees, talonavicular coverage angle greater than seven degrees, and calcaneal pitch less than 18 degrees. Of the total 109 HV patients identified with asymptomatic flatfoot, 67 patients underwent an open Lapidus procedure, and 42 patients underwent a MICA bunionectomy. Preoperative, minimum 1-year postoperative, and change in the validated Patient-Reported Outcomes Measurement Information System (PROMIS) were compared between the Lapidus and MIS groups. Preoperative, minimum 6-months postoperative, and change in radiographic measures including hallux valgus angle (HVA), intermetatarsal angle (IMA), Meary’s angle, talonavicular coverage angle (TNCA), and calcaneal pitch (CP) were compared between the Lapidus and MIS groups.
Results:
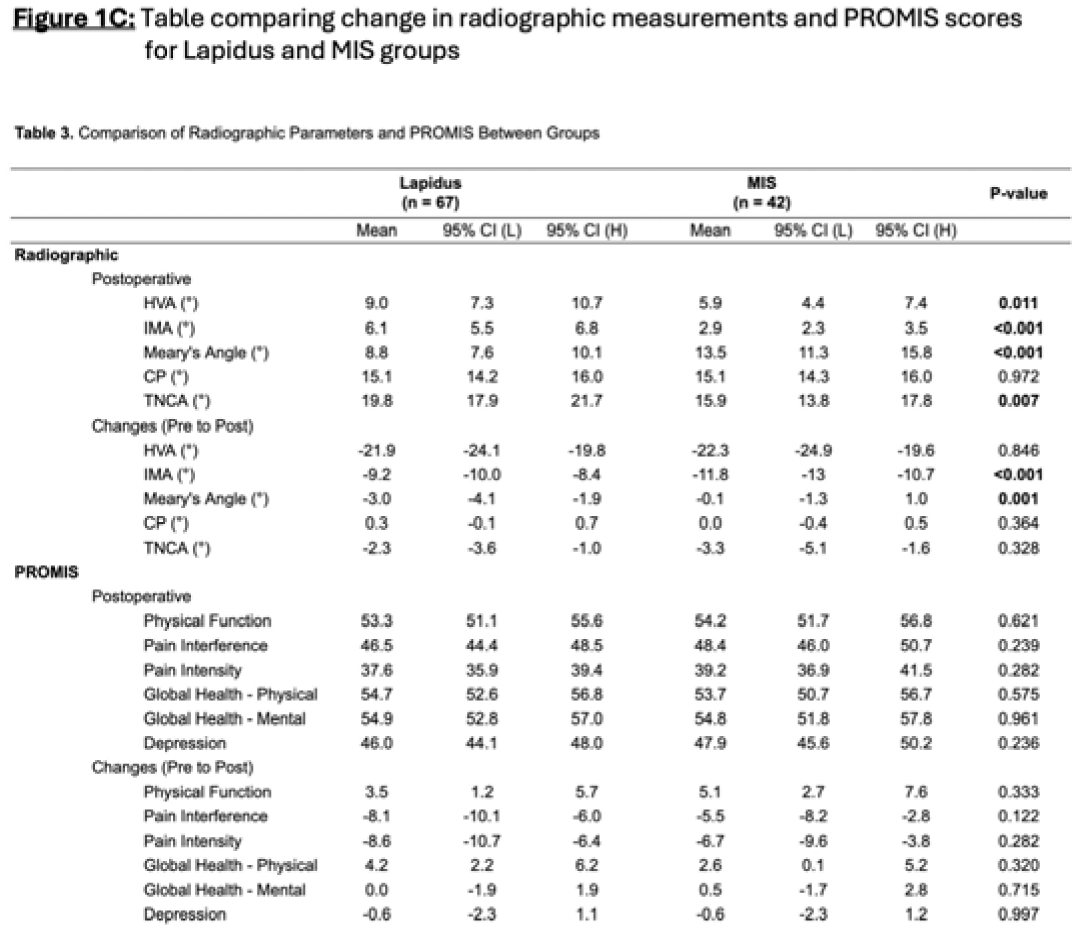
There were no significant differences between the Lapidus and MICA bunionectomy groups in terms of demographic variables (Figure 1A), preoperative radiographic measures, or baseline PROMIS scores. Both groups showed significant improvements from preoperative to postoperative assessment in PROMIS physical function, pain interference, pain intensity, and global physical health (all p < 0.05). However, no significant differences were observed between the Lapidus and MICA groups in the changes of these scores (Figure 1C). HVA correction was significantly reduced in both groups, though it did not differ significantly between the two surgical approaches (Figure 1B, 1C). MICA patients demonstrated slightly greater IMA correction (p < 0.001), while Lapidus patients saw significantly greater correction of Meary’s angle (p = 0.001).
Conclusion:
There were no significant differences in postoperative physical and pain-related PROMIS scores between the Lapidus and MICA procedures to suggest a distinction in outcomes between the two patient groups. Both the Lapidus and MICA procedures effectively corrected HVA and IMA. The MICA approach achieved a greater mean reduction in IMA, while Lapidus procedures resulted in significantly greater improvement in Meary’s angle, possibly indicating better arch restoration. However, both surgical approaches appear to be viable options for HV correction in asymptomatic flatfoot patients and can be utilized by surgeons for patients presenting with both painful hallux valgus and non-painful (non-collapsing) flatfoot.


Demographics and Outcomes for Lapidus and MIS Groups