Abstract
Research Type:
Level 4 – Case series
Introduction/Purpose:
Percutaneous Achilles tendon lengthening (PATL) is a widely used procedure for addressing gastroc-soleus equinus contracture. This study evaluates the biomechanical and anatomical outcomes of PATL using different incision distances from the Achilles tendon insertion. Key outcomes included ankle dorsiflexion improvement, tendon integrity, and sural nerve injury.
Methods:
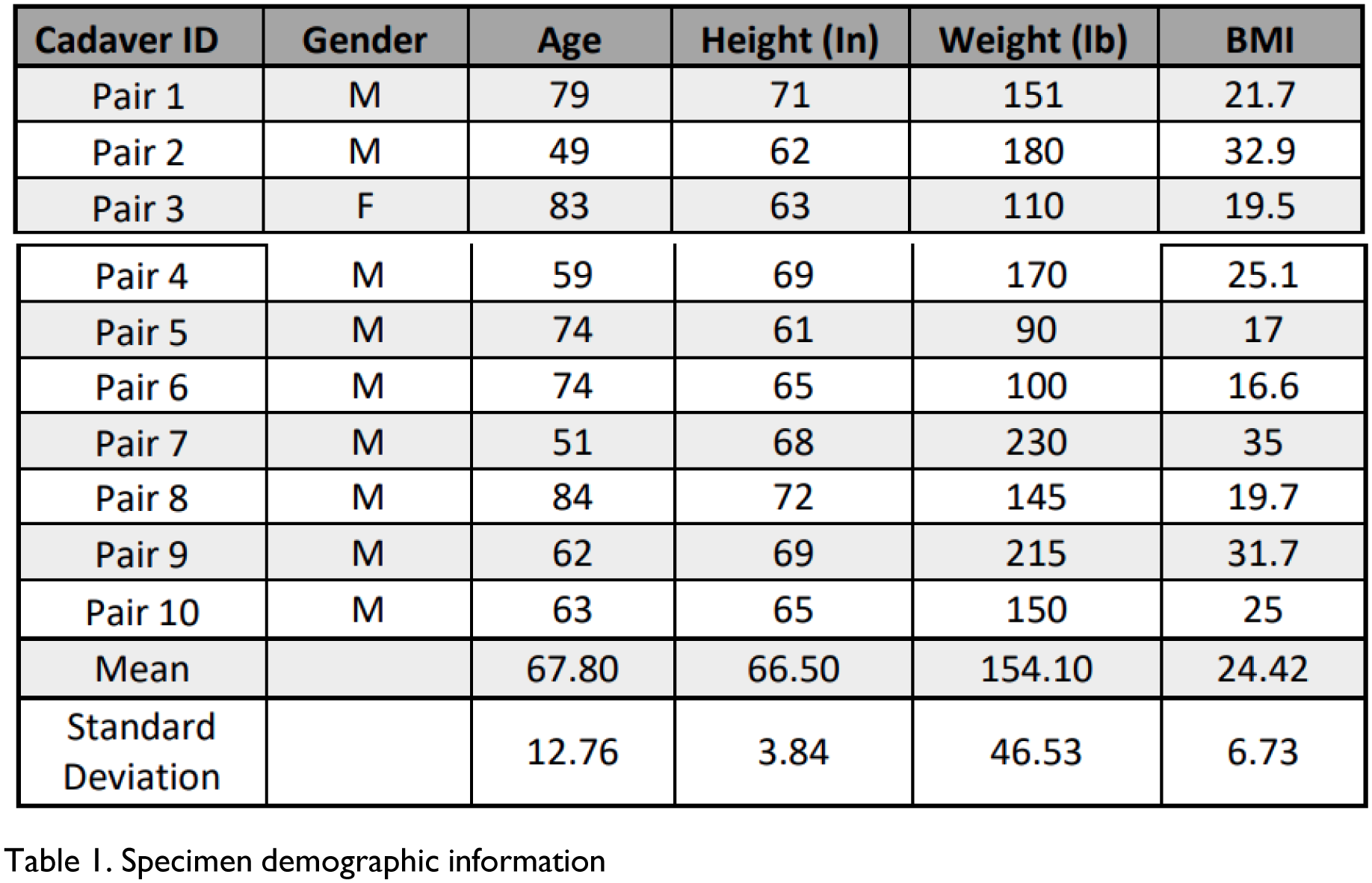
Twenty thawed fresh-frozen above-knee cadaveric specimens (ten matched pairs) were examined. Identification numbers were assigned, and demographics recorded. Limbs were marked along the distal fibula and lateral heel border, then loaded with four pounds of pressure via a tension dynamometer to measure ankle dorsiflexion in knee flexion and extension. Triple hemisection incisions were marked and performed in a medial-lateral-medial pattern, spaced either three or five centimeters apart, starting three centimeters proximal to the Achilles insertion. After hemisection, dorsiflexion measurements were repeated and tendon tension at failure recorded. Dissection assessed paratenon and sural nerve integrity, and gapping (>5 mm) at each tenotomy. Additional measurements included tendon width percentages, distances to gastrocnemius aponeurosis, and rupture status.
Investigators performed individual tasks throughout to avoid investigator bias.
Results:
The 3 cm incision group showed dorsiflexion improvements of 12.70 degrees with a straight knee and 14.60 degrees with a flexed knee, while the 5 cm incision group showed improvements of 10.50 and 12.40 degrees, respectively. Both techniques effectively increased ankle range of motion, with 3 cm incisions yielding slightly better dorsiflexion gains and higher success rates for proximal hemisections. However, the 5 cm incision group demonstrated a higher incidence of incomplete proximal cuts and insufficient tendon sliding, leading to less effective lengthening.
Sural nerve injuries were observed in 25% of specimens, and a 10% incidence of Achilles tendon rupture was recorded, particularly with 3 cm incisions. Anatomical variations in the gastrocnemius aponeurosis also influenced outcomes.
Conclusion:
These findings underscore the need for meticulous surgical planning and consideration of individual anatomical differences to optimize patient outcomes. Further clinical studies are recommended to confirm these results and guide future surgical practices.

Figure 1a-d: An example of a cadaveric specimen undergoing dorsiflexion testing pre-hemisectioning preparations.

Figure 2a-c: Examples of the aponeurosis types, 2a transverse, 2b proximal oblique, and 2c distal oblique