
Abstract
Research Type:
Level 2 - Prospective comparative study, Meta-analysis of Level 2 studies or Level 1 studies with inconsistent results
Introduction/Purpose:
Bone structure abnormalities characterize the pathogenesis and progression of osteoarthritis (OA). However, these structural changes have not been well studied in the ankle joint, or in relation to the most common etiologies of ankle arthritis: post-traumatic after fracture, or arthritis with associated ligamentous instability. This lack of information hampers our ability to optimize treatment plans for late-stage ankle OA. Utilizing a multidisciplinary approach, we sought to comprehensively quantify bone quality and patient-reported outcomes (PROs) of pain in patients with non-inflammatory ankle OA. The data analyzed represent the midway point of an ongoing prospective study supported by the Arthritis Foundation and AOFAS.
Methods:
Patients with noninflammatory ankle OA indicated for total ankle replacement (TAR) from a single institution were prospectively enrolled. Exclusion criteria were conditions (e.g., osteoporosis) or medications known to affect bone quality. Demographics and baseline patient-reported outcome (PRO) scores (PROMIS and Ankle Osteoarthritis Scale [AOS]) were obtained. Preoperatively, serum markers of bone turnover and pro-inflammatory cytokines associated with arthritis were collected. A subgroup of patients also underwent bilateral preoperative high-resolution peripheral quantitative computed tomography (HR-pQCT) of the distal tibia, which quantifies the quality of the cortical and trabecular bone. Intraoperatively, bone resected at the time of TAR underwent histopathologic analysis to characterize changes in the subchondral bone and capsule and micro-computed tomography (CT) to characterize in vivo bone quality. Correlations were described between of HR-pQCT bone quality, serum markers, PROs, and microCT results. Comparisons between post-traumatic (post-fracture) arthritis (“PTA”) and arthritis associated chronic ligamentous instability (“CIA”) were conducted.
Results:
56 patients were included to date, with mean age 65.5 ± 7.6 years, 60.7% (34/56) males, and mean BMI 29.3 ± 4.0 kg/m2. Micro-CT of intraoperative bone demonstrated that the bone density profile (as expressed by bone volume fraction [BV/TV]), was significantly associated with preoperative AOS Disability scores (R=0.343, p=0.035). However, serum bone turnover markers were not significantly associated with AOS Pain or Disability (p>0.05 for all). Serum bone turnover markers and pro-inflammatory markers as well as HR-pQCT markers of bone quality were statistically similar between PTA and CIA. Higher values of serum TNF-alpha and IL-1 correlated negatively with several HR-pQCT markers of bone quality, including total, trabecular, and cortical volumetric bone mineral density (vBMD), trabecular area, and cortical perimeter size (P < 0.05 for all).
Conclusion:
This preliminary study describes serum markers of bone turnover, imaging descriptions of bone quality, and intraoperative markers of bone quality in patients with ankle OA. Patients with post-traumatic OA secondary to fracture and patients with OA secondary to chronic ligamentous instability had similar serum markers and bone quality measures, despite very different processes that lead to the development of their arthritis. However, image-derived assessment of bone quality was associated significantly with serum biomarkers. This suggests that there may be an ultimate common pathway leading to non-inflammatory ankle OA, and there may potentially be targets for intervention, regardless of arthritis etiology.
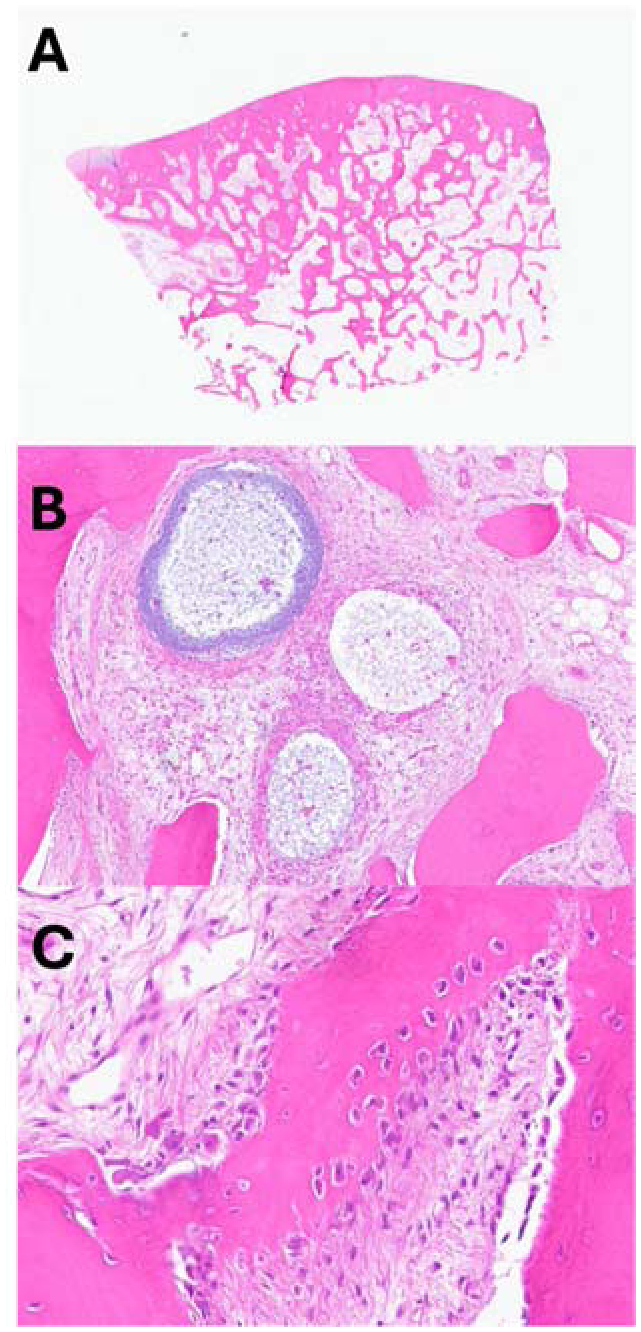
Pathologic features of end-stage ankle arthritis as determined through histopathology analysis.
A. Loss of articular cartilage with subchondral bone sclerosis of the tibia. B. Woven bone remodeling demonstrating active osteoblastic and osteoclastic activity. C. Subchondral bone interspace with cystic change.