
Abstract
Research Type:
Level 2 - Prospective comparative study, Meta-analysis of Level 2 studies or Level 1 studies with inconsistent results
Introduction/Purpose:
Cadaveric testing has shown that traditional Broström repairs of the native ATFL have inferior strength compared to the native ligament, necessitating early protection postoperatively. Augmenting Broström repairs with suture tape improves strength and stiffness, potentially allowing for faster rehabilitation.
Recently, bioinductive copolymers, such as polycaprolactone-based polyurethane urea (PUUR), have been introduced to replicate native ligament elasticity while gradually degrading. These copolymers have been proposed as augmentation materials for Broström repairs, yet no biomechanical studies have assessed their tensile properties in cadaveric models. In this study, we developed a novel copolymer augmentation technique for lateral ligament reconstruction and evaluated its biomechanical properties in a cadaveric model, comparing them to those of the native ATFL.
Methods:
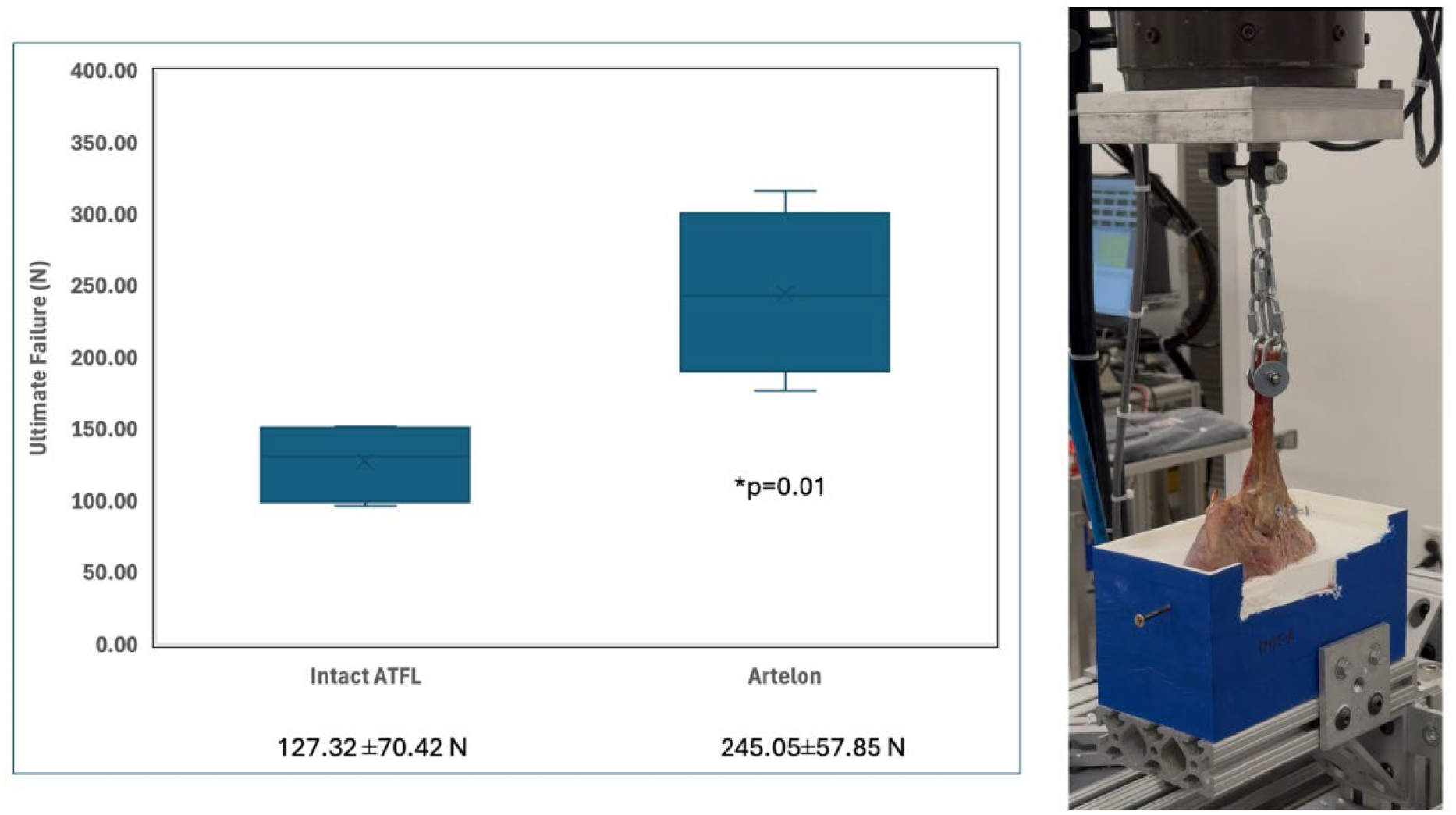
Four matched pairs of fresh-frozen cadaveric lower extremities (mean age: 89.5 years; range: 86–96) were dissected to remove soft tissue and adjacent structures, isolating the native ATFL. Each specimen was embedded in resin using a custom 3D-printed positioning system, ensuring a standardized foot alignment of 20° inversion and 10° plantar flexion relative to a vertical fibula. To enhance stability during loading, a 50 mm cortical screw was inserted superiorly to inferiorly across the subtalar joint. Unmodified copolymer augmentation samples (Flexband®, Artelon), measuring 5 mm in width and 1.5 mm in thickness, were secured with 3.85 mm anchors. A motion analysis system (Vicon) tracked reflective markers at the ATFL footprint for both native and augmented constructs. Statistical analyses assessed load (N) at 3.0 mm displacement, structural stiffness, and ultimate failure load, with significance set at p < 0.05.
Results:
At 3 mm displacement, failure load did not differ significantly between the native ATFL and copolymer construct (98.5 ± 34.3 N vs. 124.9 ± 49.8 N; p = 0.086), nor did stiffness (9.74 ± 1.63 N vs. 13.62 ± 1.48 N; p = 0.065). However, the copolymer construct had a significantly higher ultimate failure load than the native ATFL (245.05 ± 57.85 N vs. 127.32 ± 70.42 N; p = 0.01). Native ATFL specimens failed at the talar insertion, while copolymer specimens failed due to fibular anchor loosening. The copolymer band remained intact in all cases.
Conclusion:
Copolymers have emerged as an alternative to ultra-high molecular weight polyethylene (UHMWPE) sutures for ATFL repair augmentation. They replicate native ligament elasticity and promote tissue regeneration. This study is the first to assess the biomechanical properties of copolymer-augmented ATFL repairs in a cadaveric model. Our findings demonstrate that copolymer augmentation significantly increases the ultimate load to failure compared to the native ATFL. Further research with larger cadaveric studies is needed to better understand the potential benefits of copolymer augmentation in ligament repair and its role in enhancing ATFL reconstruction outcomes.
The bioinductive copolymer demonstrated a significantly higher ultimate load to failure than the native ATFL in our biomechanical study.