Abstract
Research Type:
Level 3 - Retrospective cohort study, Case-control study, Meta-analysis of Level 3 studies
Introduction/Purpose:
Lisfranc injuries represent a diagnostic challenge, particularly in detecting subtle instability with minimal displacement. Recent advancements in 3D Weight Bearing Computed Tomography (WBCT), including semi-automated measurements, distance mapping (DM), and coverage mapping (CM), offer new diagnostic insights, though their utility in Lisfranc injuries remains underexplored. Traditionally, the uninjured contralateral foot has served as the reference to account for anatomical variability. However, prior injuries, surgeries, or unavailable bilateral scans may necessitate alternative reference values. This study aimed to compare contralateral feet of patients with Lisfranc injuries to matched controls, using DM and CM. We hypothesized the absence of differences between controlaterals and controls, which would support the use of normative values of the Lisfranc complex for diagnostic purposes.
Methods:
This retrospective study included the uninjured contralateral feet of 34 patients with Lisfranc injuries, excluding those with prior injury, surgery and radiographic signs of midfoot arthritis or deformities. The control group consisted of the unaffected feet of 34 patients who underwent WBCT for unspecified foot and ankle pain or other injuries. Cases and controls were matched 1:1 by gender and laterality, as well as by age and BMI using a 0.3 SD caliper width. Semi-automated WBCT segmentation was performed, followed by manual selection of eight Lisfranc complex regions (M1-C1, M2-C2, C1-M2, C1-C2, C2-C3, NC1-3). M1-C1, M2-C2, and C1-C2 were further divided into four subregions. Using MATLAB, DM quantified joint spacing, and joint coverage was measured as the percentage of distances < 4mm. Agreement between DM and CM was assessed using ICCs and Bland-Altman charts. Group differences in DM, CM, and foot alignment were compared using paired t-tests (p < 0.05 considered significant).
Results:
Each group included 34 patients (23 women and 11 men), with 16 right and 18 left feet. The Lisfranc patients’ mean age was 41.6 (SD 18.1) years, while controls averaged 42.2 (SD 17.2) years (P=0.37). BMI values were 28.3 kg/m2 (SD 6.4) and 28.1 kg/m2 (SD 6.4), respectively (P=0.34). ICCs were poor for both DM (-0.19 to 0.31) and CM
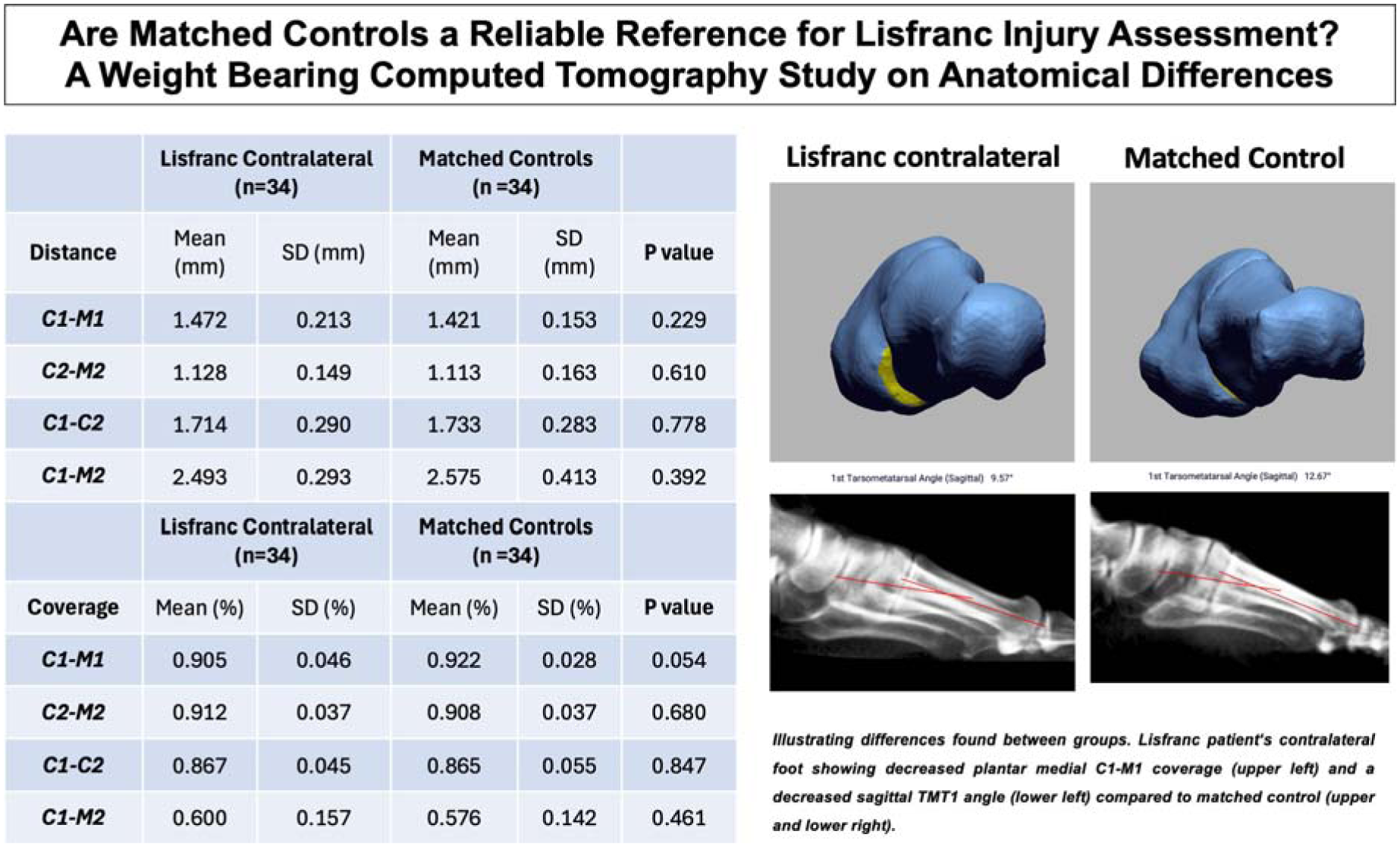
(-0.26 to 0.47). No significant differences were found in all measured 20 distances and 19 of 20 joint space coverage values, with the smallest differences in C1-M1, C2-M2, C1-C2 and C1-M2. However, plantar medial C1-M1 coverage was lower in contralateral Lisfranc feet (74.5% vs. 81.4%, P=0.016). Among 27 foot alignment measurements only the sagittal first tarsometatarsal angle differed significantly (8.33° vs. 9.63°, P=0.0229).
Conclusion:
Unlike the contralateral side, DM and CM from a paired matched control should not be used to assess Lisfranc injuries. However, our study provided DM and CM values from a matched control group which on average did not differ from the contralateral sides and may serve as normative values: C1-M1 (1.421mm, 0.922% coverage), C2-M2 (1.113mm, 0.908%), C1-C2 (1.733mm, 0.865%), and C1-M2 (2.575mm, 0.576%). The first TMT joint
demonstrated differences in joint coverage and sagittal first metatarsal angle. Further research should explore how altered potential constitutional instability of the first TMT joint may contribute to Lisfranc injuries.