
Abstract

Introduction
Partial calcanectomy (PC) is a well-established limb salvage procedure, primarily indicated as an alternative to below-knee amputation (BKA) for nonhealing heel ulcerations with associated calcaneal osteomyelitis. 1 The procedure aims to resect all infected and nonviable bone and soft tissue, allowing for a tension-free closure and a functional, end-bearing limb. 1 Literature on PC largely focuses on high-risk patients with diabetes, vascular disease, or renal failure. Patients that require salvage procedures such as BKA are associated with high morbidity, ~70% five-year mortality, and poor rehabilitation potential.1,2
Existing studies are limited by short follow-up (24-36 months) and a near-exclusive focus on comorbid patients, with “success” defined narrowly as wound healing and amputation avoidance. 3 Consequently, there is a scarcity of data regarding the outcomes of PC for traumatic indications. Most partial calcanectomy (PC) studies involve physiologically compromised patients, with failure rates up to 65%.4-7 In contrast, this report describes a healthy 24-year-old soldier who sustained a blast injury and underwent PC, offering a unique 5-decade long-term perspective on outcomes in an optimized host.
Case Presentation
Initial Injury and Acute Management (1969)
In 1969, a 24-year-old male Vietnam war soldier sustained a high-energy blast injury to his left hindfoot from mortar round shrapnel. He was treated at the Second Surgical Hospital APO 96289. The injury resulted in extensive soft tissue damage and devitalization of the calcaneus. In the resource-poor field hospital, the decision was made to perform an immediate and aggressive surgical debridement, which included a partial calcanectomy of approximately 70% of the bone, sparing only the anterior process.
Following initial stabilization, the patient was transferred to the Ryuku Islands Medical Facility and subsequently to Valley Forge General Hospital for further management. The severity of the initial trauma was underscored by the rapid onset of significant complications. Just 11 days postinjury, he was diagnosed with a surgical site infection and osteomyelitis of the residual calcaneal remnant. Concurrently, a complete tibial nerve palsy was identified, resulting from direct or indirect nerve injury from the blast. This manifested as a complete loss of both motor and sensory function supplied by the medial and lateral plantar nerves, rendering the sole of his foot insensate (Table 1).
A timeline of the patient’s clinical journey including procedures, changes to clinical management and significant developments in the patient’s condition.

Chronic Management and Intervening Decades (1970-2012)
After being honorably discharged because of his wounds, the patient was admitted to a Veterans Affairs Hospital in late 1969, for management of fever and persistent drainage from the surgical site. From 1970 to 1984, he required repeated debridements for chronic osteomyelitis and was placed on long-term suppressive ciprofloxacin.
This strategy proved remarkably effective, ushering in a quiescent period that lasted 3 decades. From 1984 to 2012, the patient was clinically asymptomatic with respect to his hindfoot, allowing him the use of his limb for independent ambulation despite the underlying anatomical and neurologic deficits. Throughout his clinical course, he never utilized a functional brace or immobilization outside of the perioperative period. Prior to his injury, he was an exceptionally fit individual as an active servicemember. Following his injury, he was not able to participate in sports or high-demand activities but was able to ambulate at length and perform his activities of daily living.
Recurrence and Modern Management (2012-Present)
After 28 years of disease quiescence, the patient began to experience reactivation of the dormant infection. Between 2012 and 2015, recurrent infections required several debridements and multiple antibiotic trials. The operating surgeon deemed any further resection of the calcaneus would destabilize the foot and render it functionally useless, so no further deep debridements were performed. He remained clinically stable on ciprofloxacin from 2015 to 2024. The patient’s earliest radiographs from his clinical journey were not maintained by the health systems where he received treatment; however, the patient’s earliest obtainable radiographs are included (Figure 1).

Earliest available nonweightbearing radiographs of the left foot including (A) anteroposterior, (B) oblique, and (C) lateral views demonstrating severe loss of the posterior and middle third of the calcaneus with complete absence of the calcaneal tuberosity but preservation of the anterior articulating surfaces of the calcaneus.
Despite several offers for amputation through the years, the patient consistently declined. He was well aware of the risks associated with chronic osteomyelitis and prolonged fluoroquinolone use, but prioritized limb preservation and functionality. By 2024, the patient’s cultures were uniformly resistant to ciprofloxacin after decades of exposure. He was switched to trimethoprim-sulfamethoxazole (TMP-SMX) and managed with repeated bedside irrigations.
A follow-up MRI in 2024 showed marrow signal changes consistent with prior osteomyelitis but no active evidence of infection, indicating successful infection control through suppressive and localized care (Figure 2).
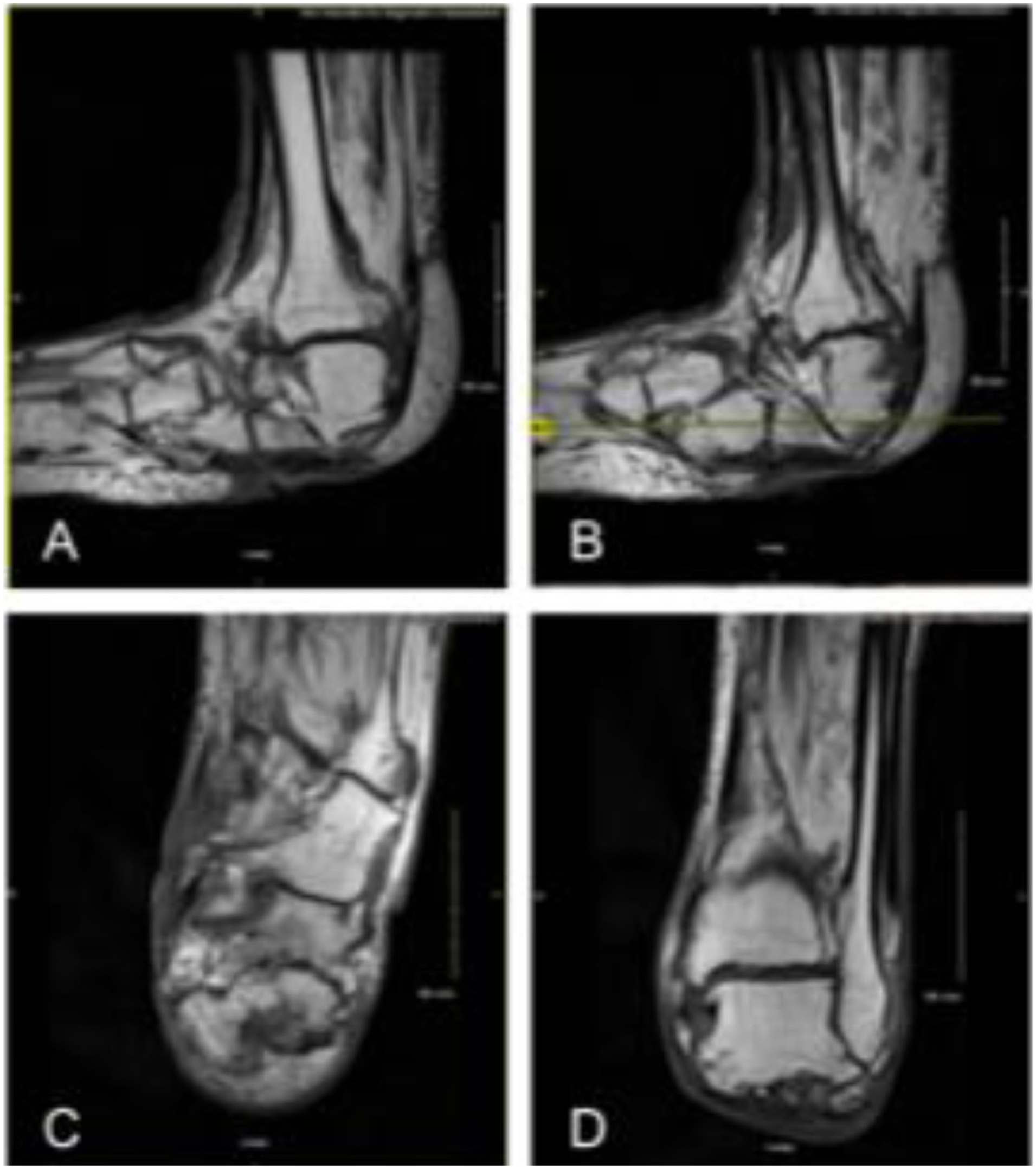
MRI of the left hindfoot (2024) showing postsurgical changes consistent with remote partial calcanectomy and no active osteomyelitis. (A) Sagittal T1-weighted view showing absence of posterior calcaneus. (B) Sagittal oblique image with preserved soft tissue envelope. (C) Coronal image showing no reactive marrow edema. (D) Axial view with remodeling of calcaneal remnant and no abscess formation.
Clinical Examination and Functional Status
Current physical examination showed a well-healed heel with lateral/posterior deformity and a chronic plantar sinus tract (Figure 3). Radiographs demonstrate the absence of the posterior calcaneus with preserved midfoot alignment (Figure 4).

Gross clinical photographs of the left foot: (A) Lateral weightbearing view shows altered contour of the hindfoot and absence of the posterior calcaneal prominence. (B) Posterior axial stance view reveals rounded, soft tissue–covered heel stump without structural calcaneal support. (C) Lateral view highlights soft tissue collapse and healed surgical scars. (D) Medial view showing pliable soft tissue envelope with evidence of past debridement and subtle scarring. (E) Plantar view displays a chronic draining sinus tract with superficial fibrinous exudate over the posterior heel pad.

Weightbearing plain radiographs of the left foot. (A) Dorsoplantar view showing preserved alignment of the forefoot and midfoot with complete absence of the posterior calcaneus. (B) Lateral view illustrating loss of the posterior calcaneal tuberosity, remodeling of the anterior calcaneal process, and preserved tibiotalar and subtalar joint integrity.
Despite the massive 70% calcanectomy with subsequent debridement leading to even further resection, the chronic osteomyelitis, and the complete plantar insensitivity, the patient, now 79 years old, ambulates independently without the use of a cane, walker, or brace. His gait is observably altered but is stable and effective for community ambulation. Throughout his 54-year clinical journey, he has remained resolute in his desire to preserve his limb, consistently refusing the option of a BKA. The patient is overall satisfied with the state of his limb as it allowed him a functional extremity with the understanding that he would have lifetime limitations. The patient was able to maintain a full-time occupation until his retirement at the age of 65.
Discussion
Partial calcanectomy is well described for heel ulcers from vascular insufficiency, but little literature exists on traumatic cases because of rarity and alternative salvage methods.3,4,5
In this case report, we describe the medical journey of a man who sustained a near-total partial calcanectomy as a result of a high-energy blast injury sustained during combat and the following 50+ years of clinical management. Although our patient sustained significant soft tissue damage and devascularization of the hindfoot in the context of wartime resource limitations, he still retained functional use of his extremity and was otherwise physiologically healthy at the time of his injury. This begs the question, in similar patients with isolated and unreconstructable hindfoot injuries, can near-total calcanectomy be a viable salvage option especially as it preserves amputation as a viable option later?
The described patient requires lifelong suppressive antibiotics because of intermittent worsening infections, requiring debridement procedures performed either in-office or in the operating room. This requires close medical follow-up with numerous anesthesia events and an untold amount of time and effort spent in the preservation of his limb. The patient’s family shared how difficult it was for them to live with his injury, unable to play or engage in activities with them like other people could. Unquestionably, to this patient amputation would have been unacceptable as long as there was even the smallest chance of salvaging the limb and his family supported him but although only one sustained the injury, they paid the cost together.
There are many clinical, functional, and economic implications of limb salvage vs BKA that remain important dimensions of treatment decision making. Recent prospective evidence is provided by the OUTLET study, which compared limb salvage to transtibial amputation in adults with severe lower extremity injuries. 8 Authors found small differences between these groups in most patient-reported functional outcomes such as physical performance, pain, return to work, and participation in rigorous activities. However, there was a significant improvement in mobility scores among the amputation group, particularly among complex pilon/ankle fracture injury patterns. This is consistent with our patient’s lived experience.
In aggregate, functional long-term outcomes may be similar between the 2 treatment options but recent data have suggested that in injuries of increasing severity and complexity, especially of the hindfoot or ankle, outcomes favor BKA. Economically, limb salvage has higher initial costs because of the complex nature of the procedures and prolonged care but lower lifetime costs when considering ongoing prosthesis and rehabilitation expenses. Additionally psychosocial burden with amputation should be considered, as higher rates of depression, anxiety, and social isolation are seen among these patients.9,10 A key consideration in this patient’s perceived success and an important limitation in the design of the OUTLET study is the concept of choice. The described patient chose this clinical course for himself at every turn and thus gained a large sense of agency and personal investment in the outcome. In the OUTLET study, patients were stratified to their respective groups at the discretion of the operating surgeon. Although some degree of patient agency and joint decision making is assumed in the modern era, the degree to which each patient would have chosen their respective clinical course if given an informed choice is unknown.
With the benefit of hindsight and the current understanding of patient outcomes in similar complex injuries, whether this patient would have chosen to undergo a BKA is ultimately a matter of preference and context. What is certain is that the presented patient’s decades-long limb preservation reflects remarkable resilience and is a triumph of highly coordinated interdisciplinary care.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251413583 – Supplemental material for Unable to Heel: The Clinical Journey of a Traumatic Near-Total Calcanectomy With 54 Years of Follow-up
Supplemental material, sj-pdf-1-fao-10.1177_24730114251413583 for Unable to Heel: The Clinical Journey of a Traumatic Near-Total Calcanectomy With 54 Years of Follow-up by Serge Andreou, Najeeb Baig, Rumyah Rafique, Ameen Suhrawardy, Pranav Khambete and Robert Meehan in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
Ethical approval was not sought for the present study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Serge Andreou: Chief Research Officer of MERGE Surgical Solutions LLC. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.