
Abstract
Background:
Minimal resection total ankle arthroplasty (TAA) has been linked to an increased incidence of tibial component lucency in large preoperative coronal plane deformity. Lucency has been linked to implant loosening. Because radiographic lucency may reflect implant micromotion, lack of bony ingrowth and/or early component loosening, we analyzed a series of TAA cases with varying degrees of preoperative coronal deformity. Our primary aim was to determine if larger preoperative tibiotalar angles were associated with increased postoperative tibial component lucency in the Cadence TAA system.
Methods:
A retrospective review of a single surgeon’s TAA procedures using the Cadence prosthesis was conducted. Patients aged ≥18 years who underwent Cadence TAA from January 1, 2018, to December 31, 2023, were included; those with <12 months’ follow-up or poor-quality radiographs were excluded. Lucency was defined as a radiolucent line at the interface between the tibia and the tibial component that was greater than 0.5 mm at any point. The patient’s final follow-up radiograph was used for this analysis. Pre- and postoperative tibiotalar alignment was recorded.
Results:
Fifty-five ankles were examined. The average follow-up duration was 29.8 months. Sixteen patients (29%) had no deformity. Twenty-seven patients (49%) had less than 15 degrees of angulation and 12 patients (22%) had more than 15 degrees of angulation. Postoperatively, all ankles were corrected to within 3.7 degrees of a coronal tibiotalar angle of 90 degrees. Comparisons among the 3 groups with χ2 tests and analyses of variance revealed no significant differences in tibial interface lucency across any zone (P > .05).
Conclusion:
Aseptic loosening in TAAs, indicated by peri-implant lucency, is a recognized mode of failure. Recent studies suggest that preoperative coronal tibiotalar angles greater than 15 degrees increase the risk of failure when using minimal resection TAA. In this short-term, single-surgeon cohort, there were no differences in peri-implant lucency between groups. Findings should be interpreted cautiously, given the limited follow-up and statistical power.
Level of Evidence:
Level IV, retrospective analysis.
Keywords
Introduction
As implant design in total ankle arthroplasty evolves, newer-generation minimal resection implants have become increasingly popular. These low-profile implants are designed to preserve bone stock by using small press-fit pegs or posts for initial osseous fixation. Early studies of these total ankle systems have demonstrated variable success, with the Cadence (Smith & Nephew, Inc) implant demonstrating success of 94% at 2 years and 98% at 3 years.1,2 However, a high rate of periprosthetic lucency has been reported among this implant type.1 -6 Findings from a recent study by Cody et al 3 showed a 6.5% incidence of global tibial implant lucency at 1 year with a 3.8% revision rate for tibial loosening. Furthermore, minimal resection implants may carry a higher risk of mechanical failure compared with stemmed or keeled implants. In a recent study by Henry et al, 7 implants with stems or keels reduced the risk of tibial implant failure by 95%.
One possible risk factor for postoperative tibial component lucency after minimal resection TAA is preoperative coronal plane deformity. Historically, preoperative coronal plane deformity greater than 15 degrees has been considered a contraindication to TAA, and multiple studies have implicated preoperative deformity as a risk factor for worse outcomes.8 -10 However, recent studies have demonstrated successful outcomes with minimal resection implants despite moderate to severe deformity.11 -18 As more patients with large coronal plane deformity undergo minimal resection TAA, the question of whether they carry increased risk for postoperative tibial component lucency, as well as the correlation of radiographic lucency with subsequent implant failure, remains controversial. A study by Cody et al 3 found that preoperative tibiotalar angle was not associated with increased rates of global periprosthetic lucency among low-profile implants including the Cadence (Smith & Nephew, Inc), Infinity (Stryker Medical Group), Infinity Adaptis (Stryker Medical Group), or Vantage (Exactech, Inc) prosthesis.
Our primary aim was to identify if an increase in the preoperative deformity was associated with more postoperative tibial component lucency in patients undergoing a Cadence TAA. Our secondary aim was to identify the most common sites of tibial component lucency at final follow up. Finally, we sought to identify if patients with preoperative varus deformity would develop more lateral tibial component loosening over time and, conversely, if patients with preoperative valgus deformity would develop more medial tibial component loosening over time when compared to patients without that specific deformity.
Methods
This study was approved by our internal Institutional Review Board committee.
A retrospective chart review of a single board-certified, foot and ankle fellowship–trained surgeon’s (C.J.) total ankle arthroplasty procedures using only the Cadence prosthesis with both chamfer and flat cut talus components were identified. This prosthesis was implanted via standard operative technique using traditional alignment guides via a direct anterior approach to the ankle.
The chart review was completed via an internal Current Procedural Terminology (CPT) code search of 27702. Inclusion criteria included patients who were more than 18 years old and underwent the total ankle arthroplasty procedure from January 1, 2018, through December 31, 2023. Eighty-five patients met these criteria. Exclusion criteria were less than 12 months of follow-up (20 patients) or poor-quality radiographs precluding accurate lucency analysis (10 patients). This yielded a total of 55 patients appropriate for radiographic review. In this time period, no patients underwent a revision surgery to revise their initially implanted Cadence total ankle arthroplasty. Demographic data of age, weight, laterality, date of service, and follow-up time was collected for all patients.
For all radiographic analysis, our practice-based PACS system (Merge PACS) was used. Using a tibiotalar angle measurement of 90 degrees (intersecting lines between the midsagittal line of the tibia and the talar dome, respectively) as the ideal baseline measurement, the amount of preoperative varus or valgus deformity was recorded. This measurement was recorded as a negative number for valgus and a positive number for varus ankles. These preoperative measurements were conducted by the operating surgeon (C.J.).
These patients were then divided into 3 groups. The groups were patients with no tibiotalar deformity, less than 15 degrees of deformity, and more than 15 degrees of deformity. Postoperative radiographic evaluations of each ankle were conducted at the patient’s final follow-up in the clinic, which was at an average of 29.8 months postoperatively. All deformities were corrected to within 3.7 degrees of our ideal 90-degree tibiotalar angle measurement. The range was 0 to 3.7 degrees, with an average correction of within 0.29 degrees. Examples of varus and valgus preoperative deformities are seen in Figure 2.
Lucency was defined as a radiolucent line at the interface between the distal tibia and the tibial component that was greater than 0.5 mm in thickness at any point in the defined zones as described by Malherbe et al 1 (Figure 1). The postoperative radiographic evaluations of peri-implant lucency were conducted by a board-certified, foot and ankle fellowship–trained orthopaedic surgeon (P.M.) and a board-eligible foot and ankle orthopaedic fellow (M.C.).
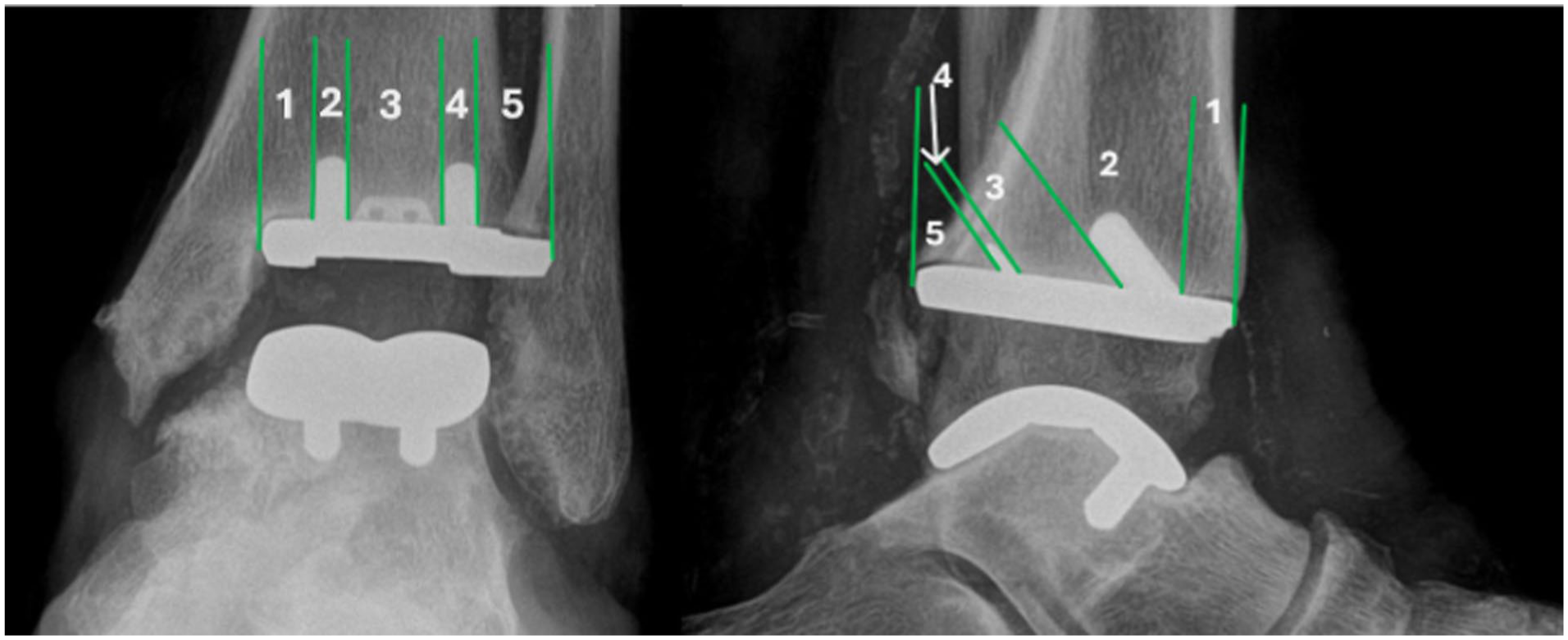
Anteroposterior (AP) and lateral zones of tibial peri-implant lucency on the Cadence total ankle arthroplasty system. In this image, the AP radiograph has lucency in zones 1 and 5, whereas the lateral radiograph has lucency in zones 1 and 5.

Radiographs showing pre- and postoperative varus and valgus deformities. (A) Preoperative varus deformity. (B) Postoperative varus deformity. (C) Preoperative valgus deformity. (D) Postoperative valgus deformity.
Statistical analysis was conducted with Data Analysis ToolPak for Microsoft Excel (Microsoft). χ2 tests were used to analyze the differences in radiographic lucency at each tibial zone between the different groups. This was also used for the nominal variables between the 3 groups (sex). One-way analyses of variance were used to compare continuous demographic data between the 3 groups (age, weight, follow-up time). Critical alpha level was set to .05, and calculated P values at or below .05 were defined as statistically significant. Based on our data set, a post hoc analysis was completed showing an estimated effect size of 0.38, which corresponds to a moderate effect. With a total sample size of 55 and 4 degrees of freedom, the achieved power is approximately 60%.
Results
Fifty-five individual ankles were analyzed after adhering to the inclusion and exclusion criteria. The mean radiographic follow-up was 29.8 months (12 months to 69 months range). With the numbers available, there were no statistically significant differences in age, weight, or sex between the 3 groups (Table 1).
Demographic Data.

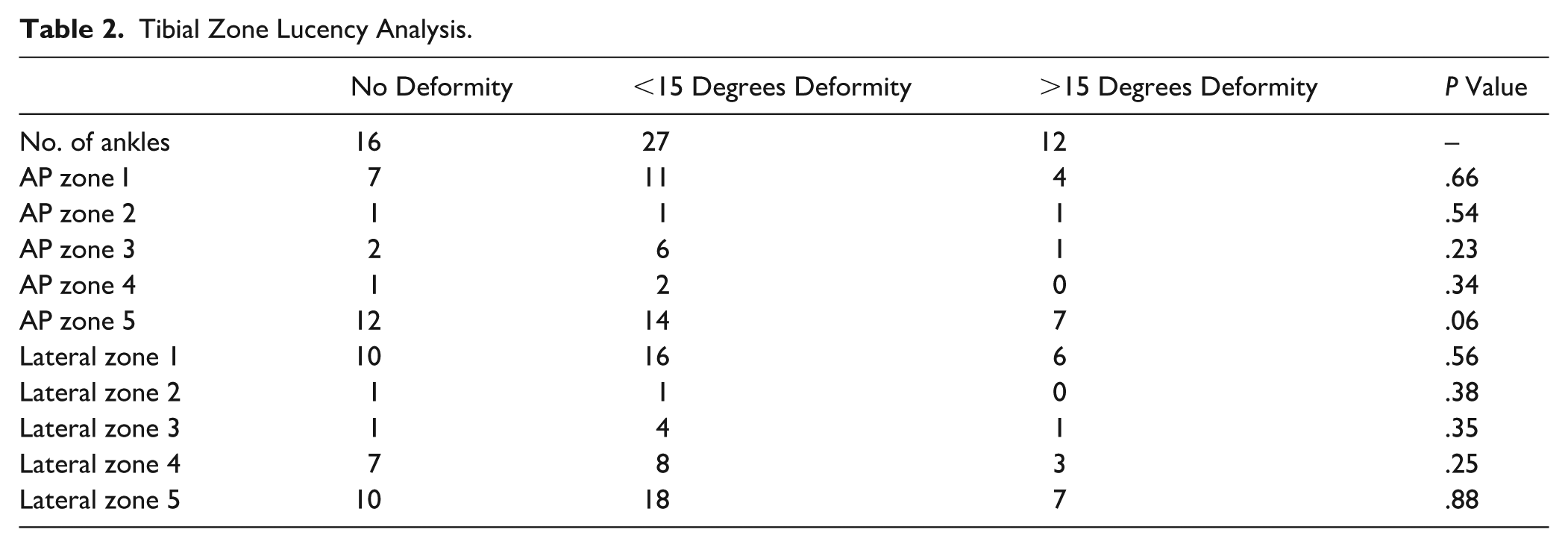
Sixteen patients (29%) had no preoperative deformity. Twenty-seven patients (49%) with a deformity of less than 15 degrees of angulation had an average of 5.4 degrees of varus and 6.6 degrees of valgus. There were 14 and 13 patients, respectively, in these groups. The remaining 12 patients (22%) had a preoperative tibiotalar angle of 15 degrees greater than neutral in either varus or valgus. There were 4 and 8 patients respectively in these groups. The mean amount of angulation was 20.3 degrees for varus ankles and 19.8 degrees for valgus ankles in this group. Tibial lucency analysis between the 3 groups showed no statistical significance in the amount of peri-implant lucency at any zone at final follow-up (Table 2).
Tibial Zone Lucency Analysis.
In the no deformity group, 2 of 16 patients (13%) had lucency in 1 zone, 1 of 16 patients (6%) had lucency in 2 zones, and 11 of 16 patients (67%) had lucency in 3 or more zones. In the <15-degrees deformity group, 6 of 27 patients (22%) had lucency in 1 zone, 4 of 27 patients (15%) had lucency in 2 zones, and 14 of 27 patients (52%) had lucency in 3 or more zones. In the >15-degrees deformity group 0 of 12 patients (0%) had lucency in 1 zone, 4 of 12 patients (33%) had lucency in 2 zones, and 5 of 12 patients (42%) had lucency in 3 or more zones (Table 3).
Amount of Zones with Peri-implant Lucency.

With the numbers available, there were no statistically significant differences noted between these groups. One patient had complete global lucency in all zones on both the AP and lateral radiographs. This patient had 10.1 degrees of preoperative varus.
On the AP radiographs, zone 5 lucency was the most commonly identified, with 35 of 55 instances (64%). On the lateral radiographs, zone 1 and zone 5 lucencies were the most commonly identified, with 35 of 55 (64%) and 37 of 55 (67%), respectively.
There were no significant differences at final follow-up in the amount of lateral (zone 5) tibial lucency when comparing preoperative varus deformity ankles to patients without any deformity, or those with valgus preoperative ankle deformity. Similarly, there were no significant differences at final follow-up in the amount of medial (zone 1) tibial lucency when comparing preoperative valgus deformity ankles to patients without any deformity, or those with varus preoperative ankle deformity (Table 4).
Tension-Sided Lucency Analysis.

Discussion
Aseptic loosening in TAAs is a known and concerning mode of implant failure. It is typically described as a radiographic lucency between the bony surface and implant interface without evidence of underlying infection or trauma. In many cases, this lucency is considered a marker of potential aseptic loosening, and an eventual need for a revision surgery. This has been noted to occur in up to 6.3% of low-profile TAA systems. 3 Identifying what constitutes radiographically significant aseptic lucency can be a challenge. Past research has used multiple different criteria to identify what is truly lack of osseous integration with the implant vs “stable fibrous ongrowth,” a term that was initially used in the hip arthroplasty literature.3 -5,19,20 For this study, it is unclear if the lucencies identified are a lack of osseous integration or “stable fibrous ongrowth.” There have been a multitude of studies that report asymptomatic periprosthetic lucencies in up to 58% of patients that do not lead to revision surgeries, and who have equivalent PROMIS scores to patients without significant lucency.1,3 -5,7,20 In a study by Kooner et al, 20 specifically reporting on 69 patients undergoing TAA with the Cadence implant, 26% of patients that were labeled as having “stable fibrous ingrowth,” which would likely have been considered lucencies in our analyzed group, were asymptomatic and had a 100% implant survivorship at 2 years. In a recent article by Cody et al, 3 6.3% (36/554) of their low-profile TAA patients were found to have “global lucency” at 1 year postoperatively. This does not match our findings, where only 1 patient out of 55 had “global lucency” at a minimum of 1-year follow-up. Fifteen of the patients in the study by Cody et al required a revision surgery for symptomatic tibial loosening, but 6 other ankles that did not have global lucency underwent revision TAA for aseptic loosening. The results of these studies challenge the finding of periprosthetic lucency as a consistent marker of patients with tibial implant loosening. This challenge is further strengthened by our finding that there were no revisions in our cohort despite greater than 40% of all patients having 3+ zones of lucency. Our study provides additional evidence that radiographic lucency in isolation is not a predictor of revision surgery.
Past literature has also suggested that the amount of preoperative deformity, notably a preoperative coronal tibiotalar angle of greater than 15 degrees, may place the patient at a higher risk of failing their TAA.8 -10 However, more recent data have shown that large varus/valgus deformities can still have good clinical outcomes without any requisite increase in risk of failure when the deformity was corrected to neutral alignment with a TAA and meticulous ligament balance and hindfoot realignment.13,15,21,22 Of note, many of the above-listed studies, similar to our own, have a short follow-up of less than 3 years. Cody et al 3 reported on 60 patients with varus greater than 15 degrees and 45 patients with valgus greater than 15 degrees without an increased rate of failure compared to patients with less severe deformities. Likewise, Sung et al 23 reported on 24 patients with greater than 20 degrees of preoperative varus ankle deformity without an increased rate of failure compared to patients with less severe deformities. Our findings reflected the conclusions from both of the above studies, showing no significant difference in the amount of tibial component lucency between the 3 groups based on the severity of preoperative deformity. Our findings, albeit in a smaller group of patients, further challenges the past belief that minimal-resection TAA systems are not indicated in patients with larger coronal plane deformities. Despite this finding, lucency should always be monitored, and progression of lucency over time may be indicative of implant loosening. If taken in isolation, and in an asymptomatic patient, serial monitoring for stability is recommended.
With use of the zone mapping as seen in Figure 1, this study is positioned well to identify exact locations of tibial component loosening, which is underreported. This granularity in identifying specific locations of peri-implant lucency allowed us to evaluate if preoperative deformity, either varus or valgus, led to specific areas of lucency postoperatively. Given the tension forces placed on the ligamentous structures in either a varus or valgus ankle deformity, we hypothesize that in the event of postoperative lucencies, varus preoperative deformities would have a greater number of zone 5 lucencies, as this is the most lateral zone. Similarly, we would expect the opposite for preoperative valgus deformities; they would have a greater number of zone 1 lucencies. After evaluating the varus, valgus, and no deformity groups against one another, there were no statistically significant differences in zones of postoperative lucency. This finding further highlights that minimal resection TAA systems such as the Cadence can be used in patients with large amounts of preoperative varus and valgus deformity without an increased risk of tension-sided lucency postoperatively.
The present study is strengthened by its large number of patients receiving the same implant, conducted by a single surgeon. This allows for consistency of surgical technique, eliminating a potentially confounding factor for postoperative radiographic outcome. In addition, this study includes a ‘no deformity’ group for analysis. By isolating this particular group, the study can truly evaluate those patients with deformity, while simultaneously providing a valuable baseline for comparison. There are notable weaknesses with this study as well. Primarily, there are no clinical outcome data for these patients in the form of patient-reported outcomes. These data would help us identify if an increasing amount of lucent zones is related to clinical outcomes. Also, the lack of revision across all patients may be reflective of an underpowered study or too short a follow-up period. An a priori sample size calculation was not conducted for this study. Our post hoc analysis showed an achieved power of approximately 60%, which falls below the generally accepted 80% power threshold for significance. Our follow-up is also short, preventing us from making more substantive claims regarding the longer-term effects of our identified tibial component lucency. Our radiographic analysis was limited by poor final follow-up radiographs, which eliminated 10 patients from inclusion in the study. Comorbidities of patients were also not controlled for, which can lead can systemic effects on recovery and long-term durability of the implant. Finally, more research is needed on the consensus of what determines a periprosthetic radiographic lucency in order for future research to be consistent in its reporting. Computed tomography may be beneficial in further classifying what constitutes lucency in future studies.
Conclusion
In this short-term follow-up study of a cohort of patients with varying preoperative deformity before low-profile TAA ankle arthroplasty, preoperative deformity was not associated with a significant change in periprosthetic tibial component lucency. These findings suggest that, when neutral alignment is achieved, larger preoperative varus/valgus angles may not independently increase early tibial lucency with this low-profile system; however, longer-term, adequately powered studies with standardized lucency definitions and clinical outcomes are needed.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251413240 – Supplemental material for Association of Preoperative Coronal Plane Deformity With Postoperative Tibial Bone–Prosthesis Interface Lucency in the Cadence Total Ankle
Supplemental material, sj-pdf-1-fao-10.1177_24730114251413240 for Association of Preoperative Coronal Plane Deformity With Postoperative Tibial Bone–Prosthesis Interface Lucency in the Cadence Total Ankle by Max Coale, Patrick Maloney, Jessa Fogel and Clifford Jeng in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
This study received ethical approval from the Mercy Medical Center IRB (approval no. 2318843) on June 13, 2025.
Consent to Participate
This is an IRB-approved retrospective study; all patient information was deidentified, and patient consent was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Clifford Jeng, MD, reports disclosures relevant to manuscript of Smith and Nephew, consulting fees, $13,000. Disclosure forms for all authors are available online.
Data Availability Statement
Patient data will not be shared with third parties.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.