
Abstract
Background:
Classically, the gold standard surgical management of recalcitrant plantar fasciitis has been plantar fasciotomy. Recent research has established a correlation between posterior leg tightness and plantar fasciitis. As a result, surgeons are increasingly performing a gastrocnemius recession to manage this condition. The purpose of this report was to assess clinical outcomes in patients undergoing a combined endoscopic partial plantar fasciotomy and a gastrocnemius recession for the treatment of plantar fasciitis.
Methods:
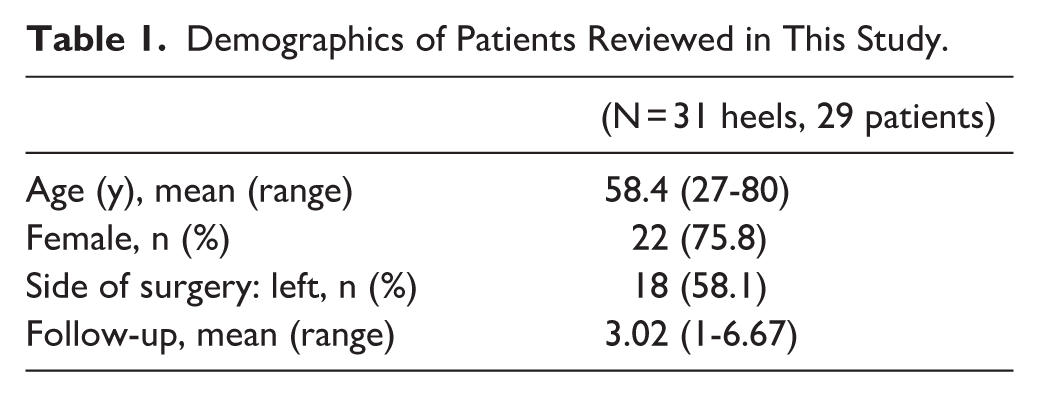
Surgery was performed on 37 feet (35 patients), of which 31 (29 patients) were retrospectively reviewed. Preoperative and follow-up measures of pain, limitations on daily activities, and maximum walking distance were assessed. Patient satisfaction, complications, and recovery time were recorded.
Results:
The mean follow-up was 3.02 (range, 1-6.67) years. The mean visual analog score for pain decreased from 9.3 preoperatively to 1.5 at final follow-up. At the most recent follow-up, 21 of 31 (67.6%) patients were completely pain free, and 28 of 31 (90.3%) were very satisfied or satisfied with the surgery. Twenty-eight of 31 patients (90.3%) returned to activity without any limitations. Complications were seen in 5 patients, including 3 patients with persistent pain.
Conclusion:
Our study demonstrated that endoscopic partial plantar fasciotomy combined with gastrocnemius recession was associated with improved pain and function in this case series. However these findings should be considered preliminary; prospective comparative studies are needed.
Level of Evidence:
Level IV, case series.
Introduction
Plantar fasciitis is the most common cause of heel pain, occurring in approximately 10% of the general population.7,13 Although most cases can be treated conservatively, 5% to 10% of patients develop persistent symptoms requiring surgery.4,10,26,30
The gold standard operative treatment for recalcitrant plantar fasciitis is plantar fasciotomy with either partial release of the medial one-third or a complete release of the plantar fascia. This may be done as an open procedure or endoscopically. Compared with the endoscopic technique, the open procedure is more invasive, painful, has a slower return to activity, and results in more complications.6,9,14,16,17,27 A concern with plantar fasciotomy is a change in the integrity of the medial longitudinal arch, which can alter foot biomechanics, and result in further complications.11,12 The literature shows that a partial, rather than a complete, release of the plantar fascia mitigates the risk of such complications.3,9 However, skeptics have sought out less traditional treatment options.
A surgical alternative to plantar fasciotomy is a gastrocnemius recession. Recently, a strong relationship between gastrocnemius tightness and plantar fasciitis has been postulated.2,10,21 -24 Contracture of the gastrocnemius may result in excess tension on the Achilles tendon, limits in ankle dorsiflexion, and ultimately, increased strain on the plantar fascia.2,5,21 -24 This contracture of the gastrocnemius has been shown to induce pain, exacerbating the symptoms of recalcitrant plantar fasciitis.2,5,21 -24 Thus, lengthening the gastrocnemius should alleviate tension and result in less symptomatic pain postoperatively. Despite growing popularity, the literature is relatively sparse regarding outcomes of gastrocnemius recession for this disease process. However, previously published studies have demonstrated strong results in regard to postoperative pain and satisfaction.1,10,18,25,26 Additionally, the hypothesized effects on calf strength were found to be insignificant in postoperative patients after gastrocnemius recession according to Chimera et al. 8
To address the entirety of pathology, the authors advocate for a surgical treatment that combines a plantar fasciotomy and a gastrocnemius recession to optimize patient satisfaction and elimination of pain in the postoperative time frame. Performing both procedures at the time of surgery has the potential to also increase patients’ functional outcomes, and thus warrants investigation as a proposed standard of care. Release of the plantar fascia paired with gastrocnemius recession, in theory, should extinguish symptomatic pain without contributing to altered mechanics or increased complication rates. There is a scarcity of literature that exists regarding the outcomes of this combination treatment. The purpose of this study is to assess pain, satisfaction, limitations on activity, and complication rates following an endoscopic partial plantar fasciotomy and an open gastrocnemius recession for patients with recalcitrant plantar fasciitis.
Results from this study offer positive outcomes in favor of combination treatment with partial plantar fasciotomy and gastrocnemius recession, but not superior or inferior to other mainstay treatments of isolated fasciotomy or recession. Although this particular single-surgeon study only included patients receiving combination treatment, it would be beneficial to have control groups for direct comparison to further refine treatment recommendations.
Methods
Patient Selection
Thirty-five patients (37 heels) had both an endoscopic partial plantar fasciotomy and an open gastrocnemius recession at our institution between the years 2017 and 2023. All surgeries were completed by a single, fellowship-trained foot and ankle surgeon. All patients had a clinical diagnosis of recalcitrant plantar fasciitis with at least 6 months of failed conservative treatment and received a combined endoscopic partial plantar fasciotomy with an open gastrocnemius recession. Patients were excluded if they had prior foot and ankle surgery or if follow-up was less than 1 year. Twenty-nine (31 heels) patients presented for follow-up postoperatively. Six patients were lost to follow-up and could not be contacted via phone. The mean final follow-up time was 3.02 (range, 1-6.67) years. The patient-reported outcomes at the most recent follow-up were used for the results of this study.
Surgical Technique and Postoperative Protocol
The patient was laid in the supine position and induced under general anesthesia. The operative extremity was prepped and draped in standard fashion, and a thigh tourniquet was incorporated to ensure exsanguination of the foot. A 3-cm incision was made over the medial calf through skin and subcutaneous tissue. After identifying and incising the deep fascia, the interspace between the gastrocnemius and soleus was bluntly developed and a vaginal speculum was introduced. With the foot in the dorsiflexed position, a long-handle No. 10 blade was used to transversely release the deep gastrocnemius fascia. This resulted in the addition of 1 cm of dorsiflexion. The wound was then irrigated copiously with normal saline. Next, a 1-cm incision was made just distal to the plantar medial calcaneal tubercle. Blunt dissection was performed in a transverse fashion, superficial to the plantar fascia, and a trocar was advanced to create the lateral portal incision. A rasp and q-tip were used to remove the fat off the inferior surface of the plantar fascia. The endoscope was introduced from the lateral portal, and with this, the width of the plantar fascia was measured. An endoscopic hook blade was inserted and used to release the medial one-third of the plantar fascia, exposing the underlying muscle belly. Attention was paid to ensure full-thickness division of the fascia. The wounds were infused with 2% lidocaine and irrigated. All wounds were closed, a sterile dressing was applied, and the patient was placed in a controlled-ankle motion (CAM) boot. Patients were allowed to immediately bear weight as tolerated and remained in the boot for 2 weeks. Patients began physical therapy for Achilles and plantar fascia stretching and transitioned to shoes after suture removal.
Clinical Evaluation
All data was collected retrospectively from medical records. Patient age at the time of surgery, sex, side of operation, and history of complications were recorded. Questionnaires were administered at routine follow-up visits postoperatively at 6 weeks, 6 months, 1 year, and at 1-year increments. The results from the most recent follow-up were incorporated in this study. Preoperative and follow-up heel pain on a visual analog scale (VAS) of 0 to 10 was collected. Additionally, patients categorized their heel pain preoperatively and at follow-up as none, mild, moderate, or severe. A subjective assessment of overall satisfaction with the procedure was administered by the study coordinator at follow-up in yearly increments, with a mean follow-up of about 3 years in clinic. Further, each patient was asked whether they were very satisfied, satisfied, slightly satisfied, or unsatisfied with the procedure. Patients were also asked if they would do this surgery again, and if they would recommend it to others. At standard preoperative and follow-up visits, patients categorized their limitations on daily activities as none, mild, moderate, or severe. The maximum walking distance the patient was able to walk until pain forced them to stop was recorded in a similar fashion. This was categorized into 3 groups: (1) less than 100 m, (2) 101 m to 1 km, and (3) greater than 1 km. To assess recovery time, patients were asked how long it took to reach complete resolution of pain following surgery. Patients with persistent pain at final follow-up were not included in the analysis of pain recovery time.
Statistical Analysis
A paired t test was employed to compare VAS scores for pain between preoperative and follow-up reports. Descriptive statistics were calculated for age, length of follow-up, VAS scores for pain, and recovery time. All statistics were computed using Microsoft Excel. Categorical data for pain, satisfaction, limitations on daily activities, and maximum walking distance was reported in tables or charts.
Results
Demographic data including age, sex, and laterality of the procedure are outlined in Table 1.
Demographics of Patients Reviewed in This Study.
The difference in VAS score for pain between preoperative (mean = 9.32, SD = 0.79) and follow-up (mean = 1.54, SD = 2.43) was statistically significant (paired t test, t = 18.3, df = 30, P < .001). At follow-up, 67.7% (21/31) heels had no pain at all, 22.6% (7/31) heels had mild pain, and 9.7% (3/31) had moderate or severe pain (Figure 1).
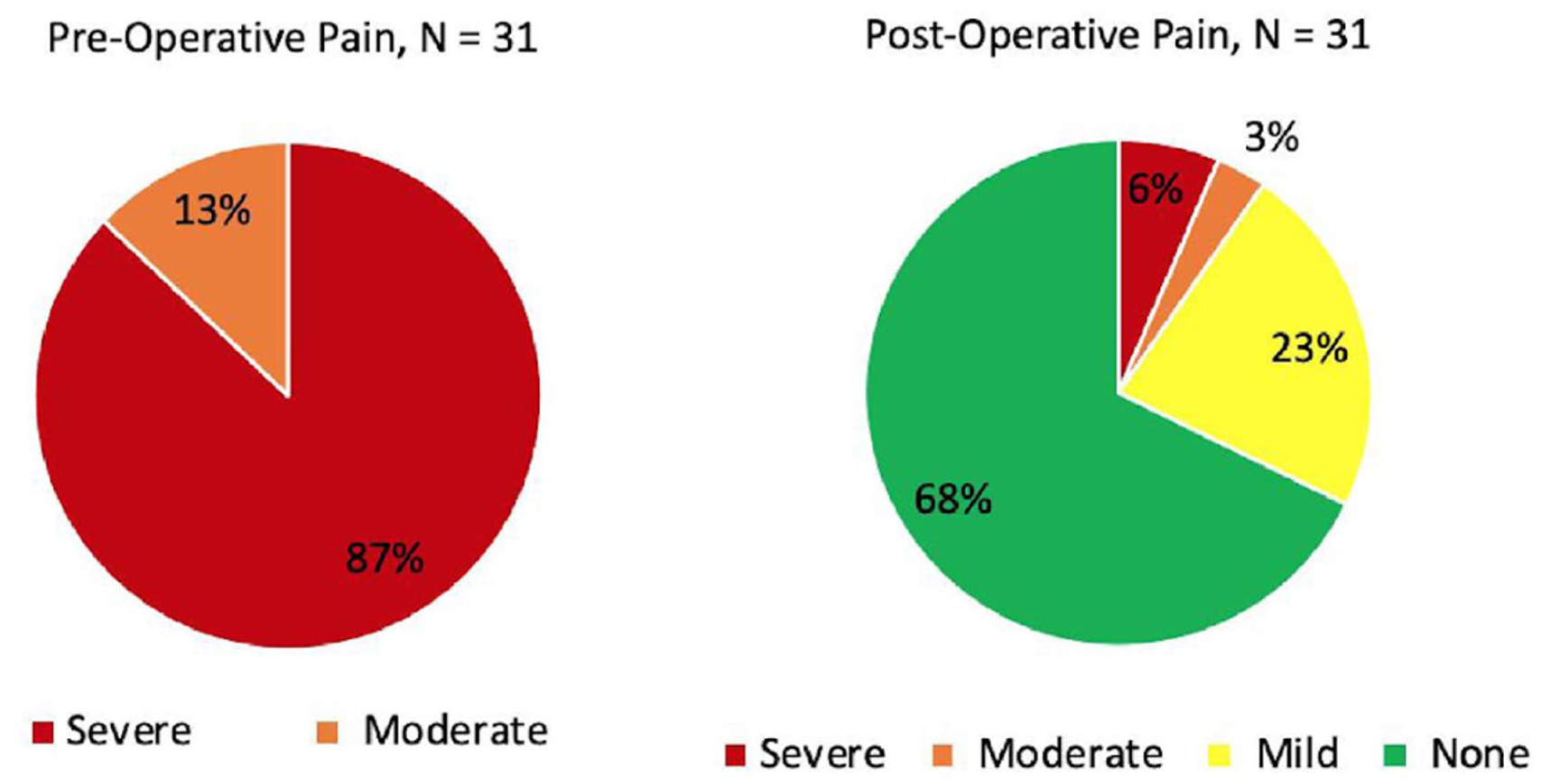
The level of pain reported by patients preoperatively and at final follow-up.
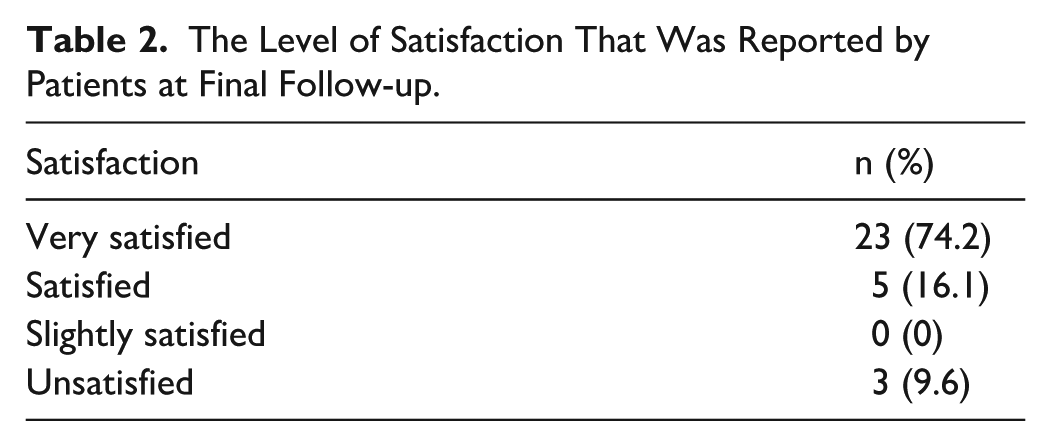
Patients had a strong subjective assessment of the procedure, with 90.3% (28/31) being very satisfied or satisfied (Table 2). All patients who were very satisfied or satisfied with the procedure said they would do it again and would recommend it to others, whereas all patients with moderate or severe pain answered on the contrary.
The Level of Satisfaction That Was Reported by Patients at Final Follow-up.
An improvement in function and limitations on activities of daily living from the preoperative state to final follow-up is demonstrated in Table 3. Before surgery, more than half of the patients could not walk more than 100 m, whereas at final follow-up, 87.1% (27/31) of patients reported the ability to walk more than 1 km (Table 4).
Limitations on Activities of Daily Living.

Maximum Distance Each Patient Was Able to Walk Before Pain Forced Them to Stop.

Patients reported a mean time of 4.2 (range, 1-12) months after surgery to reach their current level of symptoms. Patients with persistent pain were not asked about a timeline for recovery. Complications were noted in 5 patients (16%). This included 3 patients with persistent pain, 1 with a superficial wound infection at a portal site, and 1 with sensation alteration in the distribution of the sural nerve. The superficial wound infection resolved with local wound care and a course of oral antibiotics. For the patient with sural nerve symptoms, sensation returned completely by the 2-month mark following surgery.
Discussion
There is debate whether plantar fasciotomy or gastrocnemius recession alone addresses the full pathology of plantar fasciitis. Although plantar fasciotomy and gastrocnemius recession have each shown relatively promising outcomes when performed independently, the potential benefit of combining them remains uncertain. This case series suggests improved pain and satisfaction, but findings should be interpreted cautiously given the retrospective design and absence of a control group.
Results for pain and satisfaction vary across the literature among patients undergoing an isolated plantar fasciotomy. There are subtle inconsistencies in surgical technique for plantar fasciotomy that should also be considered. We advocate for a partial vs complete release of the plantar fascia. Studies show that a partial release reduces the rate of certain complications associated with plantar fasciotomy.3,9 The risks to consider with plantar fasciotomy include a decrease in height of the medial longitudinal arch and alterations in foot biomechanics, namely, an excessively pronated foot.11,12,20 As such, iatrogenic flat foot, compromise of the windlass effect, and lateral column overload due to a shift in the center of pressure of the foot are all possible outcomes of isolated plantar fasciotomy.10,12,19,20,22,28,29 Additionally, we recommend an endoscopic vs an open technique due to reports of shorter recovery time, higher patient satisfaction, and lower complication rates.6,14,16,17 When considering plantar fasciotomies, in isolation or combination treatment, our aim is the greatest reduction of symptoms postoperatively using the least invasive techniques. Davies et al 9 performed an open partial plantar fasciotomy and found a reduction in overall VAS score for pain from 8.5 to 2.5; however, 24.4% of patients continued with moderate to severe pain, and 47.7% remained with limitations on activities. Further, in that study, less than 50% of patients were totally satisfied with the surgery. Similarly, Wheeler et al 30 performed an open complete fasciotomy and found a reduction of 79% in pain measured by VAS, yet only 50% of patients were completely pain free at follow-up. These studies demonstrate an overall improvement in symptomology, yet a large percentage of patients are left without complete resolution in pain and function. Gibbons et al 11 found 44% of patients continued with ongoing pain, swelling, or tenderness at long-term follow-up after complete plantar fasciotomy, but the overall satisfaction rate was 72%. Jónás et al 15 found 77% of patients were satisfied or very satisfied with a partial fasciotomy, and 85% would do it again. The consensus across the literature appears to be that plantar fasciotomy alone provides both a reduction in pain and reasonable satisfaction rates for most patients; however, a fair portion of patients report some extent of persistent symptomology. Although our patients reported similar reduction in pain using the VAS score compared to patients undergoing complete fasciotomies, we did find greater reported satisfaction among our cohort compared with those in past literature.
More recently, a relationship between limited ankle dorsiflexion, secondary to tightness in the posterior compartment of the leg, and plantar fasciitis has been established.2,5,10,21,22,24 Such findings have highlighted the importance in evaluating and treating posterior leg tightness as a root cause of plantar fasciitis. To combat this finding, gastrocnemius recession is increasingly being used for more comprehensive treatment. Systematic reviews conducted by Pickin et al 25 and Arshad et al 2 showed large reductions in postoperative pain with minimal complications for patients undergoing gastrocnemius recession. Riiser et al 26 found statistically significant improvements in pain measured by VAS and in American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot scores for patients undergoing gastrocnemius recession with stretching vs stretching alone. Impressive satisfaction rates reported by patients receiving gastrocnemius recession and significantly improved VAS pain scores in patients following plantar fasciotomy offer promise in a combination treatment employing both surgical techniques. However, with various studies showing more than 2-point improvement in VAS scores postoperatively with recession alone, perhaps a combination treatment is not necessary for every patient.
Our study demonstrated strong outcomes for patients undergoing both an endoscopic partial plantar fasciotomy and a gastrocnemius recession. We demonstrated an 83% reduction in mean VAS scores for pain between preoperative and follow-up states. More than two-thirds of patients were completely pain-free at follow-up, and 90.3% were either satisfied or very satisfied with the surgery. Gamba et al 10 tested a similar idea comparing outcomes between an open plantar fasciotomy and a proximal medial gastrocnemius release, but not in combination. The results showed strong improvements in postoperative pain and function for both groups, but no significant differences between each other. The study yielded strong satisfaction rates of 85.8% and 89.5% with the gastrocnemius recession and plantar fasciotomy, respectively. Our results offer slightly higher satisfaction rates than those collected with plantar fasciotomy in the Gamba et al study. To our knowledge, little to no other studies have demonstrated a higher rate of pain-free patients following the surgical management of plantar fasciitis. The overall satisfaction rate we report is among the best when compared to alternative studies. About 90% of our patients returned to activity without any limitations. Further, only 3 of 31 heels had an unsuccessful outcome characterized by persistent pain, and the overall complication rate was minimal. In total, these results are promising and indicate strong performance in patients who undergo both plantar fasciotomy and gastrocnemius recession for the treatment of plantar fasciitis. Although all the postoperative VAS scores in this and the comparative studies remain within the lowest pain level, the combination procedure boasts a remarkably high satisfaction rate and still noteworthy decrease in pain postoperatively. It is worthwhile for surgeons to consider this surgical treatment plan as it produces great satisfaction and elimination of symptoms, does not affect complication rates, and addresses the full pathology.
We acknowledge several limitations to the current investigation, primarily those inherent to retrospective reporting including selection and reporting biases. The sample size may be a limiting factor although the authors feel it is consistent with previous reports and an appropriate representation of case frequency. The lack of validated outcome measures and use of only the pain VAS score limits the study and highlights the need for more thorough outcome reporting in future trials and limits interpretation. Lastly, the omission of a control group prevents from directly comparing outcomes of those undergoing the combined procedure vs those undergoing gastrocnemius recession or plantar fascia release independently.
Conclusion
In conclusion, this case series demonstrated improved pain and function following combined endoscopic partial plantar fasciotomy and gastrocnemius recession for recalcitrant plantar fasciitis. However, given the retrospective design, lack of control group, and limited outcome measures, these findings should be considered preliminary. Prospective comparative studies are needed to determine whether combination surgery offers advantages over isolated procedures.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251412894 – Supplemental material for Combination Endoscopic Plantar Fasciotomy and Gastrocnemius Recession in the Treatment of Recalcitrant Plantar Fasciitis: Clinical Outcomes From a Case Series
Supplemental material, sj-pdf-1-fao-10.1177_24730114251412894 for Combination Endoscopic Plantar Fasciotomy and Gastrocnemius Recession in the Treatment of Recalcitrant Plantar Fasciitis: Clinical Outcomes From a Case Series by Andrew G. Beauperthuy, Lauren Homolka, Patrick Waldron, Peter A. Falgiano, Robert J. Rowland, Gino Mercadal and Alejandro Pino in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
Ethical approval was not sought for the present study because all information was gathered from retrospective chart review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.