
Abstract
Background:
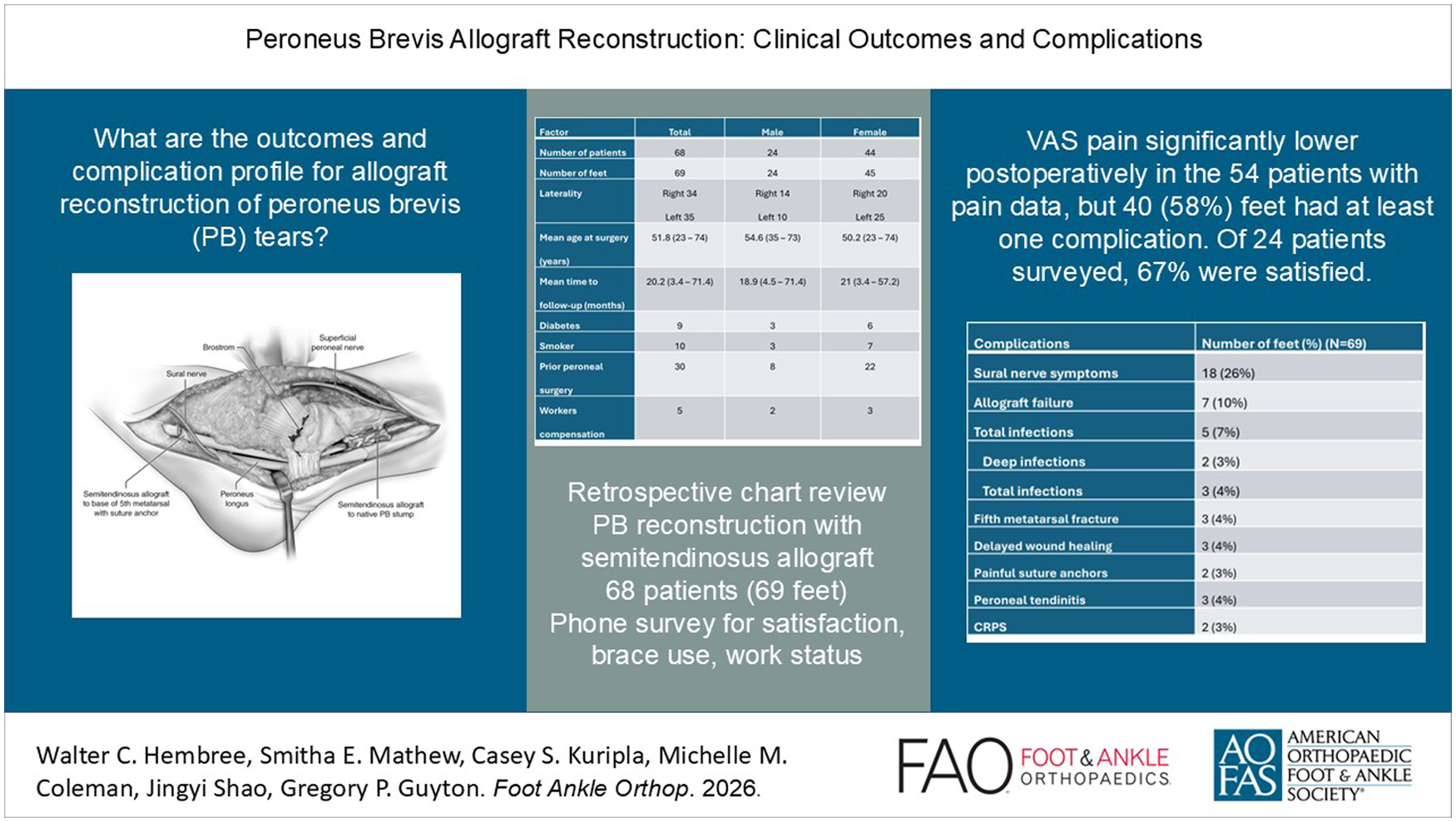
Clinical data are limited for allograft reconstruction of peroneus brevis tears, and its complication profile remains poorly defined.
Methods:
Retrospective chart review was conducted for patients with peroneus brevis tears who underwent tendon reconstruction with semitendinosus allograft at a single tertiary center between March 2010 and July 2019. A total of 68 patients (69 feet), 24 men and 44 women, were identified with mean age at surgery 51.8 (range, 23-74) years and mean follow-up 20.2 (range, 3.4-71.4) months. At the time of chart review, patients were contacted by phone to assess satisfaction, brace use, and work status.
Results:
Visual analog scale (VAS) pain score was significantly lower postoperatively (4.0 ± 2.7 vs 2.4 ± 2.8, P = .0018) in the 54 patients with VAS pain data. A total of 40 (58%) feet had at least 1 complication. The most common complications were sural neuralgia in 18 (26%) feet and allograft failure in 7 (10%) feet. Fifteen feet (21%) required reoperation, including 7 for graft failure. In the 30 feet with prior peroneal tendon surgery, there was no association between prior surgery and complications (P = .21). Of the 24 (35%) patients available for phone survey, 20 (83%) were employed prior to surgery and 18 (90%) of these employed patients returned to work and 14 (58%) did not use an assistive device at final follow-up. Sixteen (67%) of the 24 patients contacted reported being very satisfied or satisfied with the procedure.
Conclusion:
This is the largest case series to date, demonstrating significant pain improvement and high return-to-work rates in complex cases, but also a 58% overall complication rate and 10% graft failure. Allograft reconstruction may be effective when few options exist, yet careful patient selection and awareness of technical challenges are essential.
Introduction
Surgical treatment is indicated for symptomatic peroneus brevis (PB) tendon tears that do not respond to nonoperative treatment. If the tear involves less than 50% of the width of the PB tendon, traditional teaching is to debride and tubularize the tear.2,3,6,9 One cadaveric study suggested that the PB tendon can be cut down to 33% of its native width and still withstand physiologic tensile forces.6,11 However, if the tendon tear is not repairable, then the surgeon can consider one of several options. The torn PB can be tenodesed to the peroneus longus (PL), assuming the PL is intact. 7 Alternatively, if the proximal PB muscle belly is not functional, and in particular if the PL is also torn beyond repair, then transfer of the flexor digitorum longus (FDL) or flexor hallucis longus (FHL) tendon to the base of the fifth metatarsal can be considered.1,6,8,12 If the muscle belly is still functional, then reconstruction with an allograft or autograft tendon is an option.
As opposed to tenodesis or tendon transfer procedures, reconstruction with allograft maintains the native anatomy and avoids the donor site morbidity of a transfer or autograft harvest. There is also biomechanical evidence that allograft reconstruction more effectively restores distal tension compared to tenodesis of the PB to the PL. 5 Despite the potential advantages of peroneal tendon allograft reconstruction, few studies have reported clinical findings. To date, the largest case series in the literature using allograft to reconstruct the PB tendon included 14 patients who underwent PB allograft reconstruction with either semitendinosus or peroneal tendon allograft. 4 The study reports overall good clinical outcomes after the procedure albeit with a 29% rate of sural neuralgia, which remains a concern particularly in revision cases when the nerve may already be embedded in scar tissue. More data are needed to confirm the clinical efficacy and safety profile of PB allograft reconstruction.
The purpose of this study was to report the clinical outcomes and complications for a large group of patients who underwent PB reconstruction with allograft tendon at a single institution. We hypothesized that the procedure would be associated with significantly lower pain and a low complication rate.
Methods
Study Design
After institutional review board approval, patients who underwent peroneus brevis reconstruction with allograft between March 1, 2010, and July 31, 2019, were identified in the electronic medical record using the appropriate Current Procedural Terminology (CPT) codes. Operative reports were reviewed to confirm the procedure. The primary indication for the procedure was an irreparable PB tendon tear. The primary contraindication was a nonfunctional PB muscle unit as assessed on examination and preoperative MRI. Relative contraindications included previous infection in the surgical wound bed and poorly controlled diabetes. Patient demographic information was recorded. The primary outcome measure was the change in visual analog scale (VAS) score for pain preoperatively to postoperatively. Complications including superficial infection, deep infection, graft failure, sural neuralgia, and reoperation related to the graft were recorded. Graft failure was defined clinically as recurrent pain along the course of the PB allograft and/or loss of active foot eversion. If graft failure was identified clinically, then MRI was sometimes used to assist with diagnosis and revision surgical planning, but was occasionally limited by postsurgical change/scarring along the wound bed. MRI utilization in the setting of graft failure was surgeon dependent. At time of chart review, an attempt was made to contact each patient by phone to obtain secondary outcome measures including patient satisfaction with the procedure, use of postoperative assistive devices, and work status. Depending on when the patient underwent surgery, the phone calls were made 1-9 years after the patient underwent the procedure.
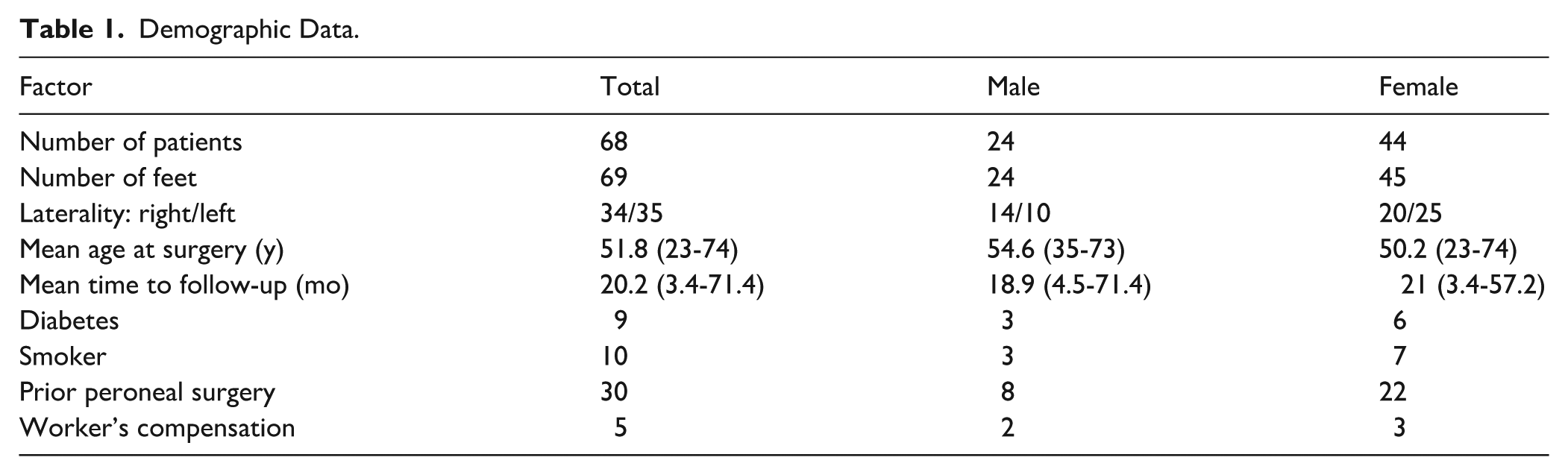
A total of 68 patients (69 feet) including 24 men and 44 women were identified. Mean age at surgery was 51.8 years (range, 23.0-74.0) and mean time to follow-up was 20.2 months (range, 3.4-71.4). The average length of follow-up was determined by the length of time (in months) from date of surgery to final follow-up in clinic or via phone survey, whichever was later. Demographic data are shown in Table 1, and concomitant procedures are shown in Table 2.
Demographic Data.
Concomitant Procedure.

Surgical Technique
Surgeries were performed by 4 attending surgeons, all fellowship trained in foot and ankle surgery. An extensile incision is made along the posterior margin of the distal fibula, curving gently toward the base of the fifth metatarsal. The peroneal tendon sheath and superior peroneal retinaculum were released in line with the skin incision, leaving a cuff for repair. When possible, the sural nerve was identified in the distal portion of the incision, dissected free of surrounding soft tissues, and gently retracted for protection. Scar tissue in some of the revision cases precluded exact identification of the nerve, but tissues in the vicinity of the nerve were protected where possible. The diseased PB tendon was excised from the wound, truncating proximally at a point approximately 4 cm proximal to the tip of the fibula. Distally, the tendon was released along its insertion at the base of the fifth metatarsal, or the tendon was truncated in a way that left a small portion of native PB tendon attached to the fifth metatarsal. A semitendinosus allograft tendon was then thawed per standard technique. Depending on the surgeon, the allografts were secured distally with either suture anchors in the base of the fifth metatarsal (n = 58), a Pulvertaft weave to the remnant PB stump (n = 10), or an interference screw in the base of the fifth metatarsal (n = 1). The tendon allografts were then routed behind the fibula along the course of the native PB tendon. In the authors’ experience, the grafts tend to stretch substantially over time and demonstrate better clinical function when slightly over-tensioned at the time of surgery. In the current series, tension was set with the foot in neutral dorsiflexion and slight eversion. While an assistant held maximal distal pull on the proximal PB stump and muscle unit, the primary surgeon secured the allograft to the proximal PB stump with a Pulvertaft weave. The superior peroneal retinaculum was imbricated and secured through drill holes in the posterior edge of the fibular using 2-0 Ethibond suture. The proximal tendon sheath was closed with 2-0 Vicryl suture. A representative final construct is shown in Figure 1.

Illustration shows final PB allograft reconstruction though an extensile incision. Proximally, the graft is attached to the native PB stump with a Pulvertaft weave. Distally the graft is secured to the base of the fifth metatarsal with a suture anchor. Care must be taken to protect the sural nerve, which crosses over the distal part of the graft.
Postoperative Protocol
Patients were splinted for 10-14 days postoperatively. If the tendon reconstruction was performed in isolation, then patients were allowed to start weightbearing in a boot at the first postoperative appointment, with gentle active eversion exercises started at 2 weeks. At 6 weeks, the patients were weaned to a lace up ankle brace and formal physical therapy started for strengthening. Most patients were able to return to full activity by 4 months postoperatively. If concomitant osteotomies were performed, patients were generally kept nonweightbearing in a boot until approximately 6 weeks postoperatively, when they were allowed to walk in the boot. Patients with osteotomies were generally weaned to a lace-up ankle brace by 8-10 weeks postoperatively.
Statistical Analysis
The differences between preoperative and postoperative VAS pain scores were approximately normally distributed based on the Shapiro-Wilk test (P = .16), supporting the use of a paired t test for comparison. Sensitivity analysis for the missing VAS data (n = 14 patients) was performed. Kruskal-Wallis test was used to compare change in VAS scores across 3 different fixation subgroups. Fisher exact test was used to compare rate of complication across the 3 different fixation subgroups. χ2 test was used to assess whether there was a statistically significant association between prior peroneal surgery and complications. Demographic data were compared between patients with (n = 54) and without (n = 14) complete VAS data. For continuous variables, age was approximately normally distributed and analyzed using an independent t test. BMI was not normally distributed and was analyzed using the Wilcoxon rank-sum test. For categorical variables, χ2 test was used when numbers were sufficient and Fisher exact test when numbers were small. Significance was set at P <.05.
Results
Pain
There was significant improvement in VAS pain scale preoperatively to postoperatively (4.0 ± 2.7 vs 2.4 ± 2.8, P = .0018), although 12 of 54 patients with complete VAS data had increased pain after the procedure. Ten of 12 patients with increased pain suffered a complication (4 sural neuritis, 2 allograft failure, 2 fifth metatarsal fracture, 1 complex regional pain syndrome, and 1 peroneal tendinitis). Four complications involving increased pain required reoperation. With sensitivity analysis for the missing VAS data (n = 14 patients), the improvement in VAS remained statistically significant (P < .05), indicating that the findings are robust to missing data assumptions.
Complications
Of 69 feet, 40 (58%) had at least 1 complication. The 3 most common complications were sural neuralgia (18 feet, 26%), allograft failure (7 feet, 10%), and infection (5 feet, 7%) (Table 3). Most of the sural neuralgia cases were transient, and only 2 required surgical intervention. There was no association between the feet that had prior PB surgery (n = 30) and presence of a complication (P = .21). Fifteen feet (21%) underwent reoperation (Table 4). The most common reoperation procedure was revision surgery for allograft failure (7 feet). Revision surgery details including concomitant procedures and time from index allograft procedure are specified in Table 5. Nerve-related procedures (3 feet) were the next most common reason for reoperation. These included 1 sural nerve grafting, 1 common peroneal neurolysis, and 1 sural nerve burial. There were 2 deep surgical site infections that required formal debridement in the operating room.
Complications (N = 69).

Abbreviation: CRPS, complex regional pain syndrome.
Reoperations (n = 15).

Revision for allograft failure excluded cases of deep infection.
Nerve procedures included sural nerve burial, common peroneal neurolysis, and sural nerve graft.
Incision and drainage for deep infection.
Reoperations for Graft Failure (n = 7).
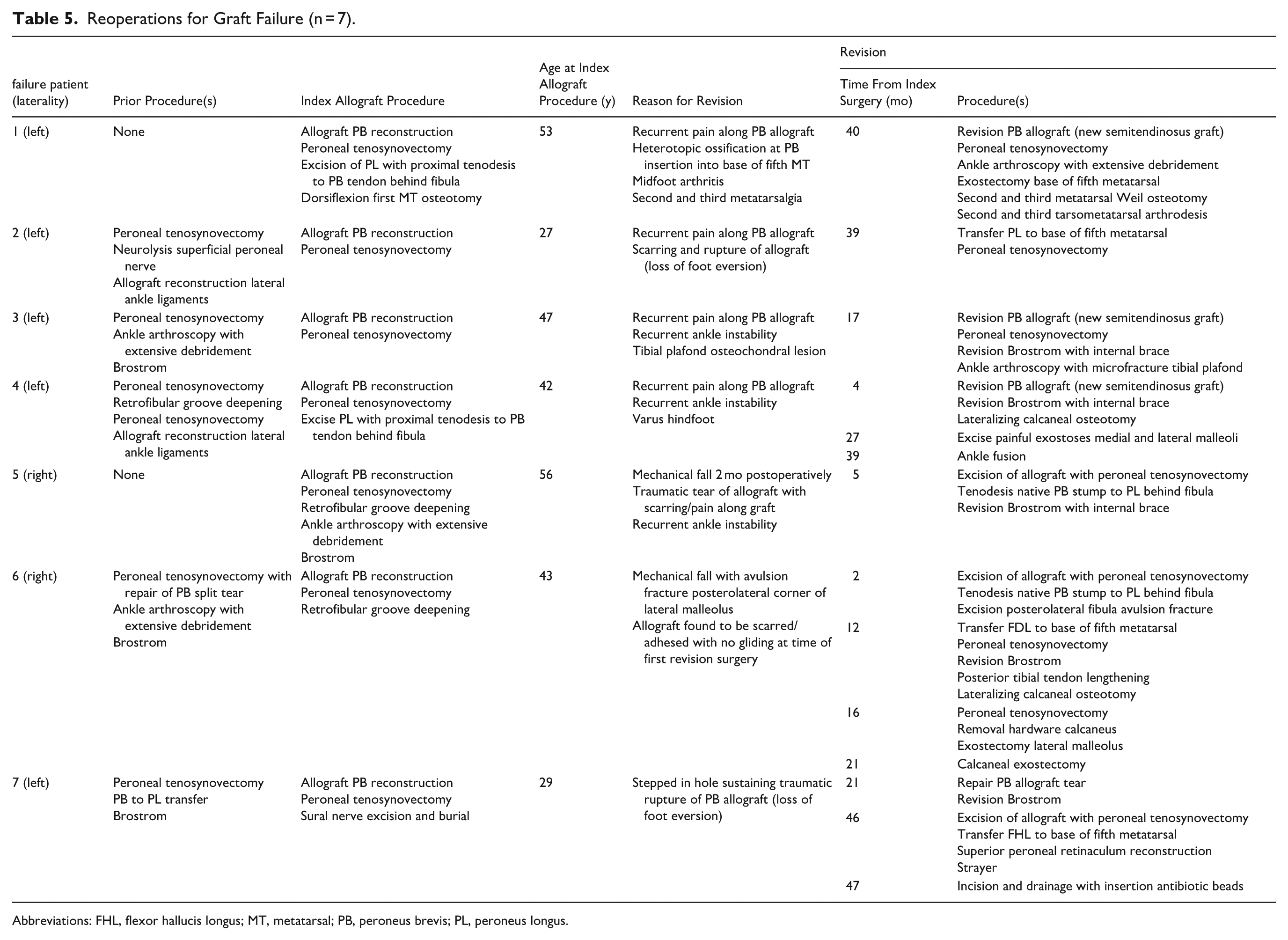
Abbreviations: FHL, flexor hallucis longus; MT, metatarsal; PB, peroneus brevis; PL, peroneus longus.
Demographic Comparison
Demographic data were compared between the patients who had complete (n = 54) and incomplete (n = 14) VAS pain scores. There were no significant differences between the 2 groups (Table 6). Similarly, demographic data was compared between patients who responded to the phone survey (n = 24) and those who did not respond (n = 44). No differences were found between the 2 groups (Table 7). Additionally, there was no significant difference in the concomitant procedures performed between patients with and without complete VAS pain scores. There were more peroneal tubercle excisions performed in the survey responders (n = 3) vs the nonresponders (n = 0) (P = .039). Otherwise, no differences were found in the concomitant procedures performed between the 2 survey response groups.
Demographic Comparison Between Complete and Incomplete VAS Data.

Abbreviations: BMI, body mass index; PB, peroneus brevis; VAS, visual analog scale.
Demographic Comparison Between Survey Responders and Nonresponders.

Abbreviations: BMI, body mass index; PB, peroneus brevis.
Subgroup Analysis
Subgroup analysis was performed for the 3 different fixation types used to secure the allograft to the base of the fifth metatarsal. There was no significant difference in the change in VAS scores across the 3 fixation subgroups (P = .175). Similarly, there was no significant difference in the rate of complications between the 3 fixation subgroups (P = .496).
Telephone Survey
Of the 24 (35%) patients available for the phone survey, 20 (83%) were employed prior to surgery and 18 (90%) of these employed patients returned to work postoperatively. Ten patients (42%) used an assistive device at final follow-up, which included orthotics/support shoes (n = 6), ankle braces (n = 3), and a cane (n = 1). Sixteen (67%) of the 24 patients contacted reported being very satisfied or satisfied with the peroneal tendon allograft reconstruction, and 7 (29%) reported being dissatisfied or very dissatisfied. None of the 7 dissatisfied or very dissatisfied patients experienced an infection, 1 experienced allograft failure requiring revision, and 3 experienced sural nerve symptoms not requiring surgery.
Discussion
To our knowledge, this study represents the largest case series to date on peroneus brevis allograft reconstruction. Although VAS pain scores improved significantly, the procedure was associated with a high overall complication rate (58%), including sural neuralgia and graft failure. Most sural neuralgia cases were transient, but 2 required nerve-related surgery. In a subset of patients who completed a final phone surgery, there was a high rate of return to work, low rate of assistive device use, and overall good patient satisfaction after the procedure. Though the complication rate must be considered, these findings suggest that allograft reconstruction of the PB tendon represents an effective treatment option for the complex problem of irreparable PB tendon tears.
With regard to postoperative pain, the results of the current study corroborate the smaller case series (n = 14) reported by Mook et al, 4 demonstrating that allograft reconstruction effectively reduces pain in patients with irreparable peroneal tendons tears. However, the average postoperative VAS pain score in our study (n = 54 patients) was slightly higher (2.4 ± 2.8 vs 1.0 ± 1.4) than that reported by Mook et al. Mook et al also reported that no patients had an increase in postoperative VAS scores whereas 12 of 54 (22%) patients in the current study experienced increased pain. Of the 12 patients in the current study with increased pain postoperatively, 10 experienced 1 or more postoperative complications, and 4 of these underwent a reoperation. The reason for the different pain outcomes in the current study is unclear, although the larger sample size might provide a more accurate representation of the types of complications that can occur and contribute to pain after the procedure.
The rate of sural neuralgia (26%) in the current study was similar to that reported in the previous series (28.6%). 4 Most of the sural neuralgia in the current study was transient, with only 2 (11%) requiring a sural nerve–related procedure. These findings are overall in line with those of Mook et al, who reported that 50% of their cases of sural neuritis were transient and no reoperations were required for the patients who remained symptomatic. Nonetheless, these data emphasize the need for careful dissection and protection of the sural nerve when performing allograft PB reconstruction. As indicated in the surgical technique section, the authors of the current study make an attempt in every case to identify the nerve and protect it. Given the high rate of postoperative sural neuralgia in the current series, one might theorize that the act of dissecting and retracting the nerve could itself contribute to nerve irritation. The alternative of not identifying the nerve would likely be worse, leading to complications such as nerve laceration and/or nerve impingement from suture material in the base of the fifth metatarsal or errant placement of the graft over the top of the nerve as opposed to underneath it. Sural nerve identification is not always possible when there is significant scar tissue present, especially when there has been prior surgery along the peroneal tendons. Nonetheless, we found no association of previous PB tendon surgery and the presence of a postoperative complication, suggesting that scar tissue in the area of the distal peroneal tendons does not appear to increase the risk of postoperative sural neuralgia.
All of the allograft failures in the current study underwent reoperation, and none of these were related to infection. The 2 deep infections in the current series underwent formal incision and drainage in the operating room. These findings directly contrast with those of Mook et al, who reported no allograft failures, no infections, and no reoperations. The reason for this discrepancy is unclear, although the sample size in the current study was 5 times larger, which might have introduced a wider variation of patient factors contributing to complications.
In the current investigation, 90% of surveyed patients who were employed before the surgery returned to work. These results support the findings by Steel and DeOrio 10 who found that 90% of the employed patients in their case series were able to return to work after repair or tenodesis for a peroneal tendon tear. Only 1 of the 7 dissatisfied or very dissatisfied patients in the current investigation required revision surgery (allograft failure). These findings suggest that the 3 most common reasons for reoperation (allograft failure, sural nerve symptoms, and infection) did not impact the patient experience to the point of surgery dissatisfaction.
There are no clear criteria in the literature that define which patients with irreparable PB tendon tears do better with an allograft reconstruction vs a tenodesis or tendon transfer. The age range in the current study was 23-74 years, suggesting that young and old patients with varying physical demand levels can benefit from the procedure. If allograft is being considered, it is important that the patient have a functioning PB muscle belly as assessed by examination and preoperative MRI. Allograft reconstruction is the preferred technique at our institution because it maintains the native anatomy, but it should not be considered standard of care. The literature also supports tenodesis 7 and tendon transfer procedures.1,6,8,12
This study has several limitations including its retrospective design and lack of a control group. Complete VAS data were available for only 79% of patients, and more than half could not be reached for satisfaction assessment. This study did not include any validated patient-reported outcome measures specific to physical function. Surgical technique varied slightly between surgeons, particularly as pertains to the distal attachment of the allograft. However, subgroup analysis showed no difference in complications or VAS scores between the different types of fixation to the base of the fifth metatarsal. Although all surgeons in the study followed the same general graft tensioning technique, the ultimate tension achieved was not measured. Variability in tension could have affected the clinical outcomes. More than half of patients were unable to be reached by phone to obtain information regarding satisfaction, brace use, and work status. Given that in some cases the phone survey was conducted 9 years after the procedure, recall bias may also have affected the results.
Conclusion
In conclusion, this study is the largest case series to date reporting clinical outcomes of PB allograft reconstruction. Although there was a significant improvement in pain in most patients and a high rate of return to work in the subgroup of patients who completed a phone survey, the study demonstrated a high complication rate, with the most common complication being transient sural neuralgia. Allograft reconstruction of the PB tendon was clinically effective in these complex cases, where few good options exist, but the procedure was not as universally successful as previously reported in a smaller series.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251412848 – Supplemental material for Peroneus Brevis Allograft Reconstruction: Clinical Outcomes and Complications
Supplemental material, sj-pdf-1-fao-10.1177_24730114251412848 for Peroneus Brevis Allograft Reconstruction: Clinical Outcomes and Complications by Walter C. Hembree, Smitha E. Mathew, Casey Kuripla, Michelle M. Coleman, Jingyi Shao and Gregory P. Guyton in Foot & Ankle Orthopaedics
Footnotes
Acknowledgements
We thank Joyce Lavery Hall, MFA, of Lavery Illustration, Reisterstown, Maryland, for medical illustration and Lyn Jones, MA, of the Department of Orthopaedic Surgery, MedStar Union Memorial Hospital, Baltimore, Maryland, for editorial support.
Ethical Considerations
Ethical approval for this study was obtained from the MedStar Health Research Institute Review Board (approval number MOD00021344).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Walter C. Hembree, MD, acknowledges research support from Smith and Nephew, Inc, Paragon28, Inc, and Zimmer Biomet, Inc, and consulting fees from Tigon, Inc. Gregory P. Guyton, MD, acknowledges serving as consultant for Paragon28 and Exactech, receiving royalties from Stryker and Arthrex, and having stock options from Pace Surgical. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.