
Abstract
Background:
Calcaneal fractures are among the most challenging foot injuries managed by orthopaedic surgeons. Given their high technical demand and inherent complication profile, calcaneal fractures are often, but not always, referred to subspecialists with fellowship training in either Foot and Ankle (FA) or Trauma surgery. The primary purpose of this study was to evaluate practice trends and to determine whether calcaneal fracture ORIF volume and early complication rates differ among early-career American orthopaedic surgeons (typically within their first 1-2 years of practice) by fellowship training type.
Methods:
The American Board of Orthopaedic Surgery (ABOS) Part II database was used to identify all calcaneal fracture open reduction internal fixation (ORIF) cases performed from 2003 to 2019. Candidates were grouped by fellowship training. The percentage of surgeons performing calcaneal fracture surgery and the average number of cases performed per surgeon were analyzed using linear regression; odds of early complications were estimated using multivariable logistic regression.
Results:
A total of 3809 calcaneal fractures were surgically managed by 1624 early-career orthopaedic surgeons from 2003 to 2019. FA surgeons comprised the largest proportion (35.0%) and performed the greatest number of these cases (42.5%). They were closely followed by Trauma (29.6%), who performed 35.6% of the reported calcaneal fracture ORIF cases. Of all early-career FA and Trauma fellowship-trained surgeons, 72.4% and 55.1% performed calcaneus surgery, respectively. The number of cases performed significantly decreased by 0.05 cases per year over the 17-year study period. The number of cases performed on patients aged ≥50 years increased by 0.024 cases per year per surgeon. Fellowship-trained FA or Trauma surgeons had 37% higher odds of reporting an early complication compared with generalists (OR = 1.37; 95% CI, 1.04-1.80; P = .027).
Conclusion:
This study identified trends in the surgical management of calcaneal fractures over the last 2 decades. These findings may inform fellowship selection and training curriculum.
Level of Evidence:
Level III, retrospective case review.
Introduction
Calcaneal fractures are among the most challenging foot injuries managed by orthopaedic surgeons. Tarsal fractures account for 2% of all fractures, whereas calcaneal fractures account for 50% to 60% of all fractured tarsal bones. 1 Because of the irregular bony anatomy, complex joint mechanics, and variety of injury patterns, these fractures carry significant controversy in their management techniques, and a gold standard has not been established despite advances in diagnostic and operative techniques.2,3 Given their high technical demand and inherent complication profile, calcaneal fractures are often, but not always, referred to subspecialists with fellowship training in either Foot and Ankle (FA) or Trauma. The most common mechanism of injury involves a high-energy trauma, such as a fall from height or a motor vehicle accident (MVA), and men are 4 to 5 times more likely to sustain this type of injury. 2 The goals of operative management with open reduction and internal fixation (ORIF) focus on achieving anatomic reduction, with particular attention to calcaneal height, length, and alignment, as well as restoration of the articular surface to limit the risk of post-traumatic arthritis.3,4
Three meta-analyses comparing operative vs nonoperative treatment of displaced intra-articular calcaneal fractures were not able to provide a recommendation for the most efficacious treatment; however, they did find that operative management was favored slightly if anatomic reduction was achieved.4 -7 This raises the question regarding current practice trends in early-career surgeons who need to synthesize published literature and use it to shape their own evidence-based practices. Understanding practice trends is vital as it can drive the adoption of evidence-based innovations in surgical technique, surgical indications, and even industry-related surgical instruments or implants, all of which can improve patient safety, surgical efficiency, and ultimately, patient outcomes. 8 Previous research has used the ABOS database to help answer questions concerning operative management trends in early-career surgeons based on fellowship training. 9
While the literature to date is unclear and does not provide clear operative indications for the best management of these fractures, there has not been any recent literature on the incidence of young surgeons choosing operative management for calcaneal fractures, nor has there been literature regarding recent practice trends. The purpose of this study was to determine if there is a difference in calcaneus open fracture fixation procedural volume, practice trends, and early complication rates among early-career orthopaedic surgeons based on the presence and type of fellowship training.
Methods
Data were compiled by extracting case logs from the American Board of Orthopaedic Surgery (ABOS) Part II Oral Examination Database from 2003 through 2019, as these were the data available for request through the ABOS. This database typically contains 6 months of all surgical cases performed by new orthopaedic surgeons in their first year of practice in the United States after completion of residency or fellowship training. Each of these cases undergo a high level of scrutiny, requiring each surgeon to diligently outline their cases and complications for a minimum of 6 months, making this data set an excellent resource for specific cases and their subsequent short-term outcomes.
All cases with Current Procedural Terminology (CPT) codes for open reduction internal fixation (ORIF) of calcaneal fracture (CPT 28415) from 2003 to 2019 were requested from the ABOS Case Logs submitted by examinees for the ABOS Part II Examination. Percutaneous or primary fusion cases were not included. These data also included the overall case volume and the overall number of candidates per year for the examination. The year reported throughout the manuscript represents the year of the examination, rather than the actual year the surgery was performed.
Both patient demographics (age, sex) and surgeon demographics (examination year, fellowship subspecialty, and region) were obtained. Candidates were grouped by fellowship training (FA, Trauma, Both, None, or Other). The average number of calcaneal ORIF cases performed by each subspeciality was calculated per year, demonstrating annual trends in surgeon volume per specialty. The percentage of overall and fellowship-trained surgeons who performed calcaneus surgery was calculated by dividing the number of surgeons per year who performed calcaneus surgery by the total number of surgeons in each respective year. The average number of calcaneal cases performed per surgeon per region, with regions divided into Midwest, Northeast, Northwest, South, Southeast, and Southwest, was also calculated to determine which regions averaged the largest number of calcaneal cases. Patient age-specific analyses were also performed for 2 different age brackets (≤50 years, >50 years).
Rates of early complications were also compared between those surgeons who were fellowship trained in FA and Trauma vs those trained in other orthopaedic subspecialties and those who did not complete a fellowship. Early complications included any surgical or medical complication reported by the examinee. Raw rates of reported complications were also calculated for the following categories: all complications, wound complications, infection, loss of reduction, implant failure, delayed nonunion/malunion, and other.
Simple linear regression was used to compare trends in case volume over time and trends in percentages over time. Multivariable logistic regression was used to compare rates of complications between FA and Trauma surgeons, other fellowship-trained surgeons, and those surgeons who did not complete a fellowship. Variables included in the regression model were patient age, sex, and surgeon subspecialty. A P value <.05 was considered significant across all statistical analyses. All statistical analyses were performed using Stata (version 18.5; StataCorp LLC).
Results
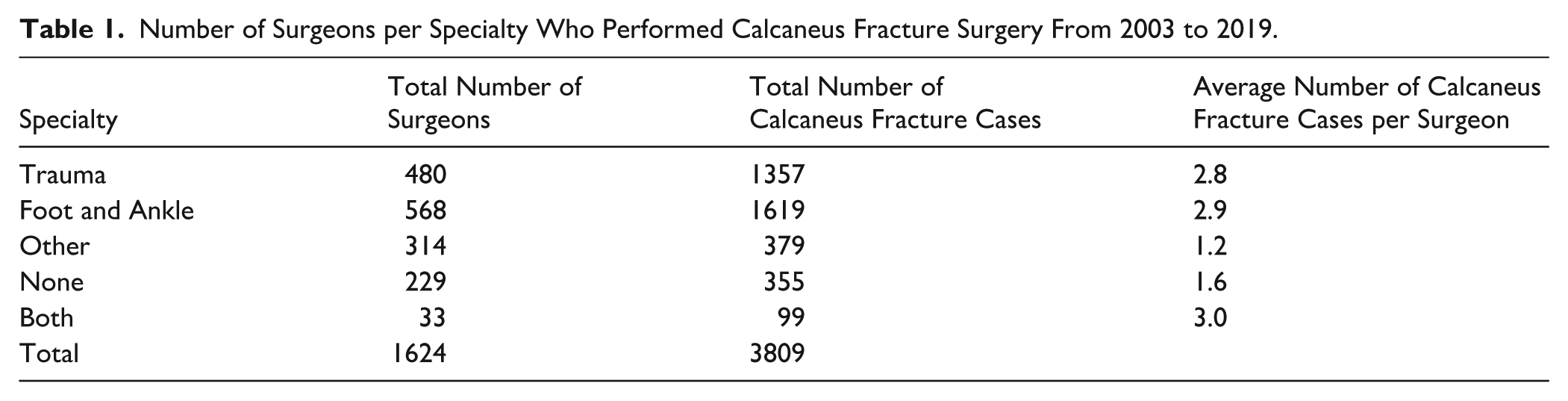
There were a total of 11 924 ABOS Part II examinees from 2003 to 2019. Of that total, 1624 surgeons performed an ORIF on 3809 calcaneal fractures. The mean age of those patients was 43.8 ± 14.9 years, with the majority (71.2%) being male. During the 17-year study period, FA surgeons comprised the largest proportion of surgeons who operated on calcaneal fractures (35.0%) and performed the largest proportion of the total number of calcaneal fracture cases (42.5%). They were closely followed by Trauma surgeons, who made up 29.6% of all surgeons performing calcaneal fracture surgery and performed 35.6% of the reported cases (Table 1). Of all FA- and Trauma-trained surgeons, 72.4% and 55.1%, respectively, performed ORIF. These proportions stayed largely steady throughout the study period, with a larger percentage of FA surgeons performing calcaneal fracture surgery compared to Trauma surgeons, except in year 2010.
Number of Surgeons per Specialty Who Performed Calcaneus Fracture Surgery From 2003 to 2019.
Although the percentage of FA and Trauma surgeons performing calcaneal fracture surgery did not significantly change over the study period, there was a small annual decrease of 0.22% from 2003 to 2019 of all surgeons performing calcaneal ORIF (Figure 1). Although the percentage of FA and Trauma surgeons who performed these surgeries did not change, the number of cases performed per surgeon per year significantly decreased over the 17-year study period (Figure 2). FA and Trauma surgeons performed 0.05 fewer calcaneus cases per year (P < .05 for both). However, the number of calcaneal fracture cases per surgeon for the Generalist remained unchanged over the study period.

Percentage of foot and ankle, trauma, and all surgeons who perform calcaneus fracture surgery.

Average number of calcaneus fracture cases performed per surgeon per year with the overlaid linear regression model.
When looking at rates per patient age group (Figure 3), the number of calcaneal fracture cases performed on patients aged <50 years slowly declined, with a rate of change of −0.020 per surgeon per year (P = .006). The opposite was seen for patients aged ≥50 years, where there was an average increase in cases per surgeon by 0.024 annually (P < .001).

Average number of cases performed over time by patient age bracket with the overlaid linear regression model.
Regionally, Trauma surgeons performed the largest average calcaneal fracture case volume in the Northwest (3.7 cases/surgeon/year) and the lowest in the Northeast (2.3 cases/surgeon/year). For FA surgeons, the largest calcaneal fracture case volume was performed in the Midwest and Northwest (3.1 cases/surgeon/year) and the lowest in the Southwest (2.4 cases/surgeon/year). Generalists’ greatest volume of calcaneal fracture surgeries was in the Northeast (2.2 cases/surgeon/year) (Table 2).
Average Number of Calcaneus Fracture Cases per Surgeon per Year by Region and Fellowship.

Regarding early postoperative complications, FA, Trauma, and other fellowship-trained surgeons reported increased rates when compared to Generalists (Table 3). The raw rates of early surgical complications for each fellowship category can be seen in Table 4.
Multivariable Regression Model for Surgical Complications Following Surgical Management of Calcaneus Fractures.
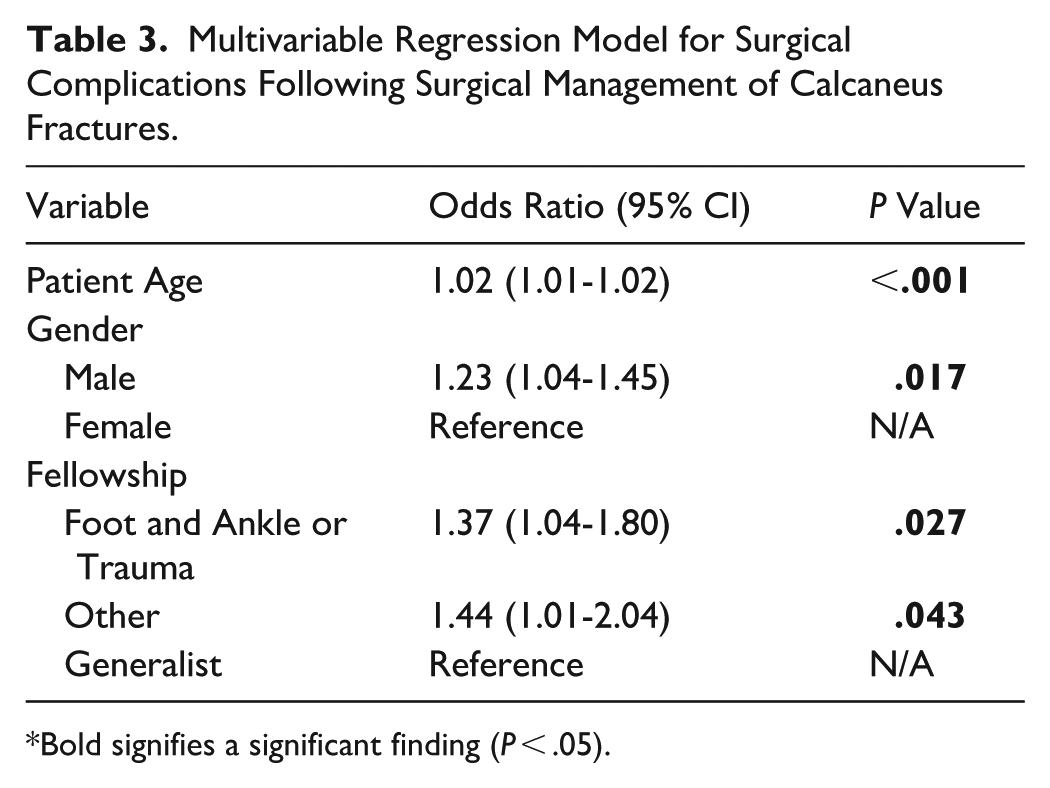
Bold signifies a significant finding (P < .05).
Average Complication Percentage for Various Types of Reported Complications per Each Fellowship Category.

Discussion
This study demonstrates which American surgeons perform calcaneal fracture surgery in their first few years of independent practice and highlights trends in case volumes over time, as well as patterns in surgical management among specific age groups. Although the percentage of FA- and Trauma-trained surgeons performing calcaneus surgery remained >70% and >50%, respectively, throughout the study period, this study demonstrated a statistically significant decrease in the percentage of all surgeons performing these surgeries. This study was also the first, to our knowledge, that highlights the annual decrease in the quantity of calcaneal fracture surgeries performed by new surgeons since 2003 and further delineates which age brackets surgeons were more or less likely to operate on over the 17-year study period.
This study provides insight into what specialties are performing the largest case volume of calcaneal fracture surgery, and it comes as no surprise that the FA and trauma-trained surgeons are the 2 subspecialties within Orthopaedics that perform the largest proportion of calcaneus surgery. FA and Trauma surgeons performed approximately 150% more calcaneal fracture procedures than those surgeons with different subspecialty training, and approximately 80% more than “Generalists.” This information can help inform residents of the subspecialty within Orthopaedics that may be of most interest to them, as roughly 3 of every 4 early-career FA surgeons and 1 of every 2 early-career Trauma surgeons surgically manage calcaneal fractures. If part of their perceived practice includes calcaneal fracture surgery, it may be most beneficial for them to pursue a fellowship in FA or Trauma. This study also demonstrates which part of the United States performs the greatest percentage of calcaneal fracture surgery (Table 2). The data from this study identified the region with the largest volume of calcaneus surgery to be the Northwest for both FA and Trauma surgeons, closely followed by the Midwest for FA surgeons and the Southeast for Trauma surgeons. However, these geographical differences are small in magnitude and are likely clinically insignificant when it pertains to overall case volume.
Regarding the treatment of displaced intra-articular calcaneal fractures, this remains controversial. Several studies have demonstrated that surgical management can provide improved anatomical reconstruction and joint restoration, but also highlight the high incidence of postoperative complications compared with those patients managed nonoperatively.5,10 -12 Many of these postoperative complications were the result of wound healing complications after use of an extensile lateral approach to the calcaneus, including superficial wound sloughing, deep surgical site infections necessitating inpatient admission for intravenous antibiotics, and often surgical debridement with or without hardware removal. 13 However, after the landmark article published by Buckley et al 14 in 2002, there was significant evidence to suggest equivalent outcomes in patients treated nonoperatively compared to those treated operatively. Although they did allude to improved outcomes in patients managed surgically when considering several patient factors that would make them good surgical candidates, such as smoking status, occupation, Sanders Classification, and unilateral involvement. 14 Similarly, as the less invasive sinus tarsi approach was more widely adopted in the early 2010s, surgical management has been associated with lower rates of postoperative complications and promising clinical and radiographic outcomes in select fracture patterns and patient populations.15 -17 Although speculative, this may explain why the percentage of FA and Trauma surgeons performing calcaneus surgery stayed similar over the study period (Figure 1), but the number of ORIF cases performed by an individual surgeon gradually declined (Figure 2). Surgeons may have become more selective in who they offer surgical management. Similarly, as the criteria for offering calcaneus surgery became more nuanced, the number of generalists performing said surgery would intuitively decrease as well, possibly electing for more nonoperative management.
This study also highlights some of the changes in patient demographics of those who underwent ORIF. Previous literature has emphasized the importance of considering nonoperative treatment options for patients aged ≥50 years, as these patients are more prone to wound healing complications and subsequent poor outcomes.13,18 However, new literature has highlighted the recent efficacy of managing calcaneal fractures in older populations.19 -21 Gaskill et al 19 demonstrated improved clinical outcomes in patients aged ≥50 years compared with those aged <50 years, with great improvements in the average adjusted American Orthopaedic Foot & Ankle Society Score, average Foot Function Index, and mean calcaneal fracture scoring system scale (P < .05 for all). This study also noted similar rates of early complications in both groups. Reed et al, 21 in a retrospective review published in 2022, further corroborated these data and emphasized that with the shift toward the less invasive sinus tarsi approach to the calcaneus, leading to decreased rates of wound healing complications. In their study, they demonstrated similar rates of complications in patients younger and older than the age of 50 years. These recent data explain the trend seen in the number of patients managed surgically in each age group in the present study. The number of calcaneus surgeries performed on patients aged ≥50 years increased over the study period (P < .05), which aligns with the current literature and continued adoption of the less invasive sinus tarsi approach associated with decreased rates of wound healing complications and subsequent poor outcomes (Figure 2).
Lastly, using the data available through the ABOS database, this study showed that patients whose calcaneus surgery was performed by an FA or Trauma surgeon were significantly more likely to encounter a postoperative and early complication than those performed by generalists (Table 3). Speculatively, this may be the result of more complex calcaneus injuries being managed by surgeons specifically trained in foot and ankle trauma. 22 However, this study cannot eliminate the possibility that the fellowship-trained surgeons have worse surgical technique or have a greater likelihood of detecting and reporting complications. This study has several important limitations inherent to the use of the ABOS Part II Oral Examination database. First, the data reflect only the practice patterns of American-only orthopaedic surgeons within the first 2 years of independent practice. As such, the trends reported here may not represent later practice patterns or the case volumes of more established surgeons. Second, the potential for case selection and reporting bias exists as cases are derived from those that each candidate selects over a 6-month period. Surgeons may preferentially include or exclude certain cases or complications, and complications are self-reported, raising the possibility of underreporting or variability in how adverse events are captured. Additionally, the ABOS only captures, on average, 6-month outcomes, so the data collection can miss late events (eg, nonunion, malunion, and hardware breakage). Fourth, because of the nature of the database and lack of granularity to account for differences in fracture severity (open vs closed injuries, intra-articular vs extra-articular patterns, and the complexity of each pattern) and operative approaches (extensile lateral vs sinus tarsi), this study was unable to capture all the potential surgical confounding variables that could influence postoperative complications in patients undergoing calcaneal fracture surgery. Similarly, the available CPT codes in the database did not allow us to differentiate between ORIF alone and primary subtalar arthrodesis nor concomitant superior peroneal retinacular and/or peroneal tendon repair performed as part of the index procedure. These concomitant procedures would indicate a more complex injury pattern and therefore may affect the complication rate. Furthermore, although basic patient demographics are included, the database lacks key clinical variables such as comorbidities, smoking status, injury mechanism, and compliance with postoperative protocols, all of which may influence complication rates. Finally, the database captures only surgically treated cases, precluding assessment of the overall incidence of calcaneal fractures, the proportion treated nonoperatively, and comparative outcomes between surgical and nonsurgical management. Together, these limitations mean our findings should be interpreted with caution and understood as reflecting the practice patterns and outcomes of newly certified surgeons rather than the broader population of orthopaedic surgeons or patients.
Conclusion
Of all early-career surgeons, FA surgeons consistently perform the largest proportion of calcaneal fracture cases, closely followed by Trauma surgeons. In the first few years of practice, approximately 3 of every 4 FA surgeons and 1 of every 2 Trauma surgeons surgically manage calcaneal fractures. Despite higher reported early complication rates, these trends may reflect greater case complexity and evolving surgical indications. FA and Trauma surgeons in the Northwest had the largest calcaneal fracture case volumes, though the noted differences are small in magnitude. Lastly, the rate of ORIF for calcaneal fractures in patients older than 50 years has slowly increased over the study period. Collectively, these observational findings may inform fellowship selection and training priorities but should not be overinterpreted for regional workforce planning, given the small magnitude of geographic differences and the fact that complication data reflect only early postoperative events rather than long-term outcomes.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251412841 – Supplemental material for American Fellowship-Trained Foot & Ankle and Trauma Surgeons Fix the Majority of Calcaneal Fractures in the First Years of Independent Practice
Supplemental material, sj-pdf-1-fao-10.1177_24730114251412841 for American Fellowship-Trained Foot & Ankle and Trauma Surgeons Fix the Majority of Calcaneal Fractures in the First Years of Independent Practice by J. Alex Albright, James D. Baker, Bailey Keith, Thomas Lynch, Thomas C. Dowd and Jeannie Huh in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
Ethical approval was not sought for the present study as this study uses a deidentified, accessible database maintained by the American Board of Orthopaedic Surgery, which is consistent with previous published literature using these data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.