
Abstract
Background:
Hallux valgus can severely limit physical function in demanding professions like military service. Traditional open surgeries have shown limited success in achieving rapid recovery and full functional return. The primary objective of this study was to assess functional outcomes of active-duty service members who have undergone minimally invasive bunion surgery.
Methods:
Eighteen active-duty service members with mild to moderate hallux valgus deformities who underwent minimally invasive bunion correction between 2020 and 2022 were retrospectively reviewed.
Results:
Minimally invasive bunion surgery demonstrated significant improvements in self-reported outcomes of the Foot and Ankle Outcome Scores from pre- to post-procedure (total score: 57.0 vs 95.0 respectively, P > .001) including all subscales of symptoms, pain, activities of daily living, sports and quality of life. Additionally, radiographic analyses revealed marked corrections pre- to post-procedure in intermetatarsal angle (12.0 vs 7.5 degrees, P < .001), hallux valgus angle (25.5 vs 12.0 degrees, P < .001), and tibial sesamoid position (5.0 vs 2.0 degrees, P < .001), with 12 of 13 patients achieving full bone consolidation by their 6-month follow-up. Complications were minimal, with only 1 case requiring further intervention. Approximately half of the patients (8/18) did not require any limited duty, and 13 of 18 remained on active duty at final follow-up (median of 13 months).
Conclusion:
These findings underscore the potential of minimally invasive surgery in high-impact populations, although further research with larger cohorts is recommended to confirm long-term outcomes and functional durability in high-stress settings.
Level of Evidence:
Level III, retrospective comparative study.
Introduction
Hallux valgus, commonly known as a bunion, is a deformity that can severely impair function and mobility. Affecting up to 23% of adults, with higher rates observed in women, the condition often requires surgical intervention once conservative measures fail. 8 Traditional surgical approaches, such as Chevron, modified McBride, and Lapidus procedures, have been the standard methods for correcting bunions. 13 Although these techniques are effective in addressing the primary deformity, questions remain about their ability to fully restore functional capacity, especially for individuals engaged in high-impact activities. 10
Only 28% of active-duty service members (ADSMs) returned to full duty 1 year after hallux valgus surgery, as determined by their ability to complete a 1.5- to 2-mile run and perform military-specific tasks. 10 Achieving full functional recovery in high-demand populations is challenging and emphasizes the potential for lingering symptoms even after corrective surgery. In physically demanding professions such as the military, it raises important concerns about the procedure’s adequacy in supporting long-term recovery.
Minimally invasive surgery (MIS) for hallux valgus (MIS HV) has recently emerged as a promising alternative to traditional procedures. 1 MIS HV offers potential for reduced post-operative pain, faster recovery times, better cosmetic results, fewer complications, and improved functional outcomes compared with open techniques.6,7 Despite promising outcomes, there is limited knowledge examining the impact of MIS HV surgery on the return rate to high-impact activities, particularly in the military population. 6
The primary aim of this study was to establish and assess post-operative functional scores and return to duty (RTD) of ADSMs who have undergone MIS HV procedures to determine the success of this technique in restoring pre-injury levels of function.
Secondarily, we wished to compare our results to the percentage of ADSMs who returned to duty following the traditional hallux valgus procedures reported in Schroeder and colleagues’ 10 2022 study. We hypothesized that MIS HV would demonstrate distinct advantages in RTD, thereby maintaining the operational readiness of military service members.
Materials and Methods
Patient Selection
The local Institutional Review Board approved this single-center retrospective chart review of patients who underwent MIS HV performed by a single surgeon between September 2020 and July 2022. This study received no funding.
ADSMs 18 years or older, diagnosed with a mild to moderate bunion deformity, defined as a first intermetatarsal angle (IMA) from 8 up to 12 degrees (mild) or an IMA from 12 up to 15 degrees (moderate), who subsequently underwent MIS HV were included. The study included patients without restricting the hallux valgus angle (HVA), allowing a broad range of deformity severity. Because of the frequent strenuous requirements of physical training, patients had attempted various conservative therapies prior to surgical intervention, including bunion splints, wider shoes, and/or activity modification. All patients were required to have at least 3 months of follow-up.
Exclusion criteria consisted of patients who had an IMA greater than 15 degrees, first ray hypermobility, moderate to severe first metatarsophalangeal joint (MPJ) arthritis, prior bunion surgery, metatarsus adductus, or incomplete functional outcome scores.
Radiographic and Clinical Evaluations
Clinical evaluation involved assessment of pain, first MPJ range of motion, first ray hypermobility, hallux reducibility, and general foot evaluation to determine the need for surgery.
Preoperative weightbearing radiographs included anteroposterior, lateral oblique, and lateral views. Preoperative radiographic assessment of the first IMA, HVA, tibial sesamoid position (TSP), and presence of first ray hypermobility were measured and documented. The first IMA was measured by drawing a line down the mechanical axis of the first metatarsal as described by Siddiqui and colleagues. 11 Because the anatomic axis of the first metatarsal is changed by translation of the capital fragment, the mechanical axis was also used to measure postoperative IMA. 11 The mechanical axis was also used to assess pre- and post-operative TSP.
Radiographic evaluations were performed prior to surgery, and at 6-week, 12-week, and 6-month follow-up visits. Osseous consolidation was categorized as minimal bone growth (Figure 1), near complete osseous consolidation (Figure 2), or complete osseous consolidation (Figure 3).

Post-operative radiograph showing minimal bone growth on the left foot.

Post-operative radiograph showing near complete osseous consolidation on the left foot.

Post-operative radiograph showing complete osseous consolidation on the left foot.
Outcome Measures
The 10-point visual analog scale (VAS) and the Foot and Ankle Outcome Score (FAOS) were collected at preoperative evaluation to establish baseline values, and at each patient follow-up visit to establish patient outcomes.
The FAOS is a 42-item questionnaire consisting of 5 subscales used to evaluate the physical function and activities of daily living (ADL) from a patient-reported perspective in individuals with foot and ankle impairments. 9
RTD status of ADSMs was measured by limited duty (LIMDU) periods or medical board status (MEDBOARD). A LIMDU is a period during which an ADSM who cannot perform their duty because of health or injury reasons is given 6 months to seek medical treatment, undergo surgery, and to partake in a physical rehabilitation program as needed. If an ADSM has exhausted 2 LIMDU periods, or has an especially poor prognosis, they are assigned to a MEDBOARD, where a committee evaluates whether they will be medically discharged.
To RTD, ADSMs should be able to meet the physical fitness test set by their service, which includes a minimum goal of push-ups and/or pull-ups, forearm planks, and run times. Satisfactory minimum skills are based on biological sex and age category, where older adults have less stringent requirements than their younger peers.14,15
Surgical Technique
Procedures are performed with the patient under monitored anesthesia care in the supine position with a sterile bump under the knee allowing 35 to 40 degrees of plantarflexion.
Under fluoroscopic guidance, the planned osteotomy is marked, and a skin incision is made distally at the medial aspect of the first metatarsal neck. Blunt dissection is carried down to bone with a mosquito hemostat. An MIS elevator is advanced in a medial to lateral direction to dissect the periosteum off the metatarsal. Next, a 2.0 × 19.5-mm straight burr is used to complete an osteotomy at the metatarsal neck perpendicular to the mechanical axis. A curved hemostat is placed in the incision and into the medullary canal of the first metatarsal, causing lateral displacement of the capital fragment. A Kirschner (K)-wire is advanced proximally along the medial aspect of the hallux, bouncing off the hemostat and into the medullary canal of the metatarsal to hold translation of the capital fragment.
With the hallux rotated and held in the desired position, a K-wire is advanced medial to lateral through the capital fragment and into the second metatarsal head to hold correction in the frontal plane. A proximal stab incision is made near the base of the first metatarsal, and 2 guide wires for the desired screw size are advanced proximal, medial to distal, and lateral into the capital fragment with attention to insert each guide wire in a different plane. A 2-screw construct is achieved with a mix or combination of 3.5-mm and 4.0-mm screws (FT compression screw; Arthrex Inc, Naples, FL). Fluoroscopic assessment was used prior to and after final fixation.
A MIS Akin osteotomy is performed as needed in select cases with a 2.0 × 13-mm straight burr and fixated with one 2.5-mm screw (FT compression screw; Arthrex Inc).
Postoperative Care
Patients were placed in a forefoot offloading surgical shoe and allowed to weight bear as tolerated on the day of surgery. Transition to normal shoe gear started postoperative week 4. Patients returned to physical training at postoperative weeks 9-12 depending on radiographic healing and symptoms.
Statistical Methods
Data were analyzed using SPSS 28.0 (IBM Corp, Armonk, NY). Variables were reported in medians with first and third quartiles (IQR) or counts with frequencies as applicable. The differences in baseline and follow-up outcomes were analyzed with the Wilcoxon signed rank test for numeric measurements and Fisher exact for categorical measurements. P values less than .05 were considered significant. Missing data were treated as missing and not imputed.
Lewis et al 6 estimated pre-operative bunion pain to be an average of 31.4 (SD 22.7) on a 1-100 pain VAS. To have an 80% chance to detect a decrease in pain of 10.0, where P less than .05 is considered significant, we determined a priori that at least 18 patient observations were required.
Results
Of the 19 patients retrospectively reviewed, 18 were included in this observational study. One patient had not completed the FAOS at final follow-up and was excluded. Of the 18 patients, 11 were female (Table 1). Ten procedures were performed on the right foot and 8 on the left foot. No patients demonstrated prior hypermobility, and only 1 had a prior procedure (subtalar arthroereisis). Ten patients also underwent concurrent akin osteotomy.
Patient and Procedural Characteristics (N = 18).

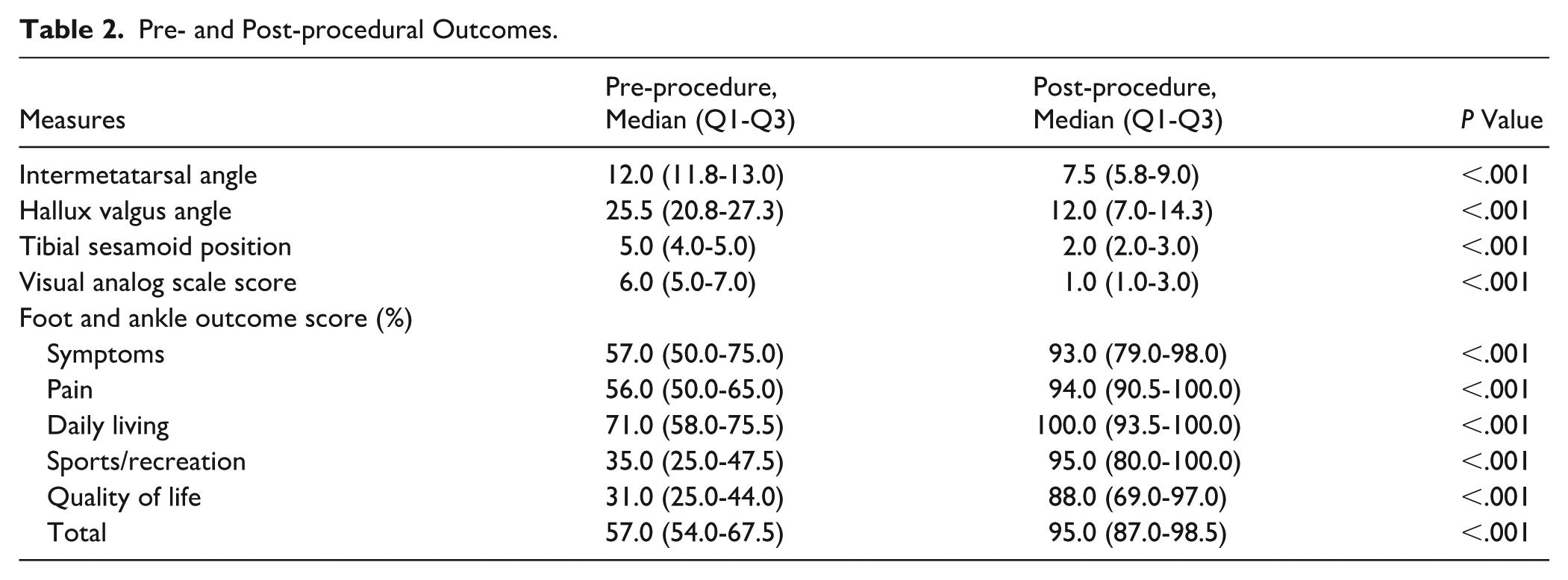
Postoperative radiographs (Figure 4) showed significant improvement over preoperative images (Figure 5) in IMA (12.0 vs 7.5 degrees, P < .001), HVA (25.5 vs 12.0 degrees, P < .001), and TSP (5.0 vs 2.0, P < .001, Table 2). Patients reported significantly reduced pain, from 6.0 to 1.0 (P < .001). On the FAOS tool, patients reported significant overall improvement, from 57% to 95% (P < .001, Table 2) as well as significant improvement on the subscales of Symptoms, Pain, Daily Living, Sports/Recreation, and Quality of Life.

Radiograph showing pre-operative hallux valgus on the right foot.

Radiograph of minimally invasive bunion correction of the right foot at 6 months postoperatively
Pre- and Post-procedural Outcomes.
Median follow-up was 13.0 months (IQR: 5.8-18.3, Table 3). At 6 weeks, 94% (17/18, Table 3) patients completed their follow-up radiography, 8 of which showed minimal bone growth. At 12 weeks, complete or near complete osseous consolidation was evident for 73% (11/15) of patients who had received their follow up radiography, and at 6 months, 14 of the 15 patients who had undergone the follow-up radiography had complete consolidation. There were 2 reported patient complications: 1 delayed union and 1 hardware irritation requiring hardware removal.
Procedural Follow-up and Outcomes (N = 18).

Abbreviation: LIMDU, limited duty.
No LIMDU period was required by 8 of 18 patients (Table 3). As of final follow-up, 72% (13/18) were still active duty whereas 18% (5/18) either underwent a planned separation or retirement from the military. Of note, all 5 of separated or retired patients had completed the RTD fitness test required for separation eligibility.
Excluding ADSMs who were expected to separate or retire during study follow-up, as per Schroeder et al 10 study exclusion criteria, 92.9% (13/14) of our patients returned to duty, which is a significantly higher rate than the 28% (18/64) who returned to duty after open bunion correction (P < .001) in that study.
Discussion
MIS HV is highly effective in ADSMs, who require rapid recovery and full functional return to meet the high physical demands of their job. Our results showed significant improvements in both pain and functional outcomes, as evidenced by FAOS scores and postoperative radiographs, following MIS HV. This suggests MIS HV offers more efficient structural correction and pain relief, which is critical for ADSMs who need to return to full operational capacity as quickly as possible.
Results in literature comparing MIS HV to open procedures vary. Multiple meta-analyses have consistently found no significant difference in radiologic outcomes or complication rates.1,5,12 Post-operative pain and AOFAS scores were either similar between procedures or significantly improved with MIS HV.1,5,12 Patient satisfaction was either similar between procedures or significantly improved with open procedures.5,12 These discrepancies may be due to the wide variety of surgical techniques and lack of high-quality, level 1 evidence.1,4 However, when compared directly to open distal chevron osteotomies, MIS HV led to quicker rehabilitation, improved patient satisfaction, and superior pain relief outcomes. 2
None of our patients exhibited hypermobility, which is notable because joint laxity can complicate surgical outcomes, necessitate alternative procedures, and prolong recovery. The need for structural integrity and pain-free mobility is paramount in the military, as ongoing pain and functional limitations could result in decreased performance and the inability to meet the physical demands required for service.
The comparison between this study and Schroeder and colleagues’ reveals notable differences in outcomes, emphasizing the potential advantages of MIS HV over traditional open surgical approaches in high-demand populations. The significantly lower RTD rate (28%) found with open surgeries 10 suggests that traditional open surgery may not be as effective in facilitating a rapid return to high-impact activities. Additionally, a large proportion of their patients experienced ongoing discomfort and an inability to perform critical military tasks, reflecting less favorable overall recovery.
This study has several limitations as a retrospective study where patients who underwent MIS HV were specifically chosen with radiographic parameters consistent with a mild to moderate bunion deformity. We purposely excluded severe deformities with hypermobility because of the initial instability of the capital fragment at the osteotomy site despite internal fixation and delayed osseous integration seen in MIS HV procedures. The principal surgeon felt the degree of shift required to achieve clinically significant radiographic reduction would be too unstable to resist the amount of axial load sustained in high-impact exercise in the early postoperative period. Second, we also acknowledge the relatively small sample size used in our cohort. Further research with larger samples is necessary to explore the long-term durability of these outcomes. The selection of patients from a military treatment facility can introduce bias because of the high proportion of healthy, active working adults 3 ; however, it aligned with our goal to examine patients with high activity demands.
Comparisons to Schroeder and colleagues’ study were made to a similar population of military personnel with surgical treatment of mild to moderate bunion deformity and using a similar RTD metric, but were done by different surgeons, at a different institution, in a different military service with different RTD qualifications. Follow-up required 1-year post-operative radiographs, whereas we accepted 6-month radiographs. 10 However, high turnover amongst military personnel makes it difficult to standardize follow-ups at set time intervals, although all patients included in our study made their final follow-up and completed outcome assessments.
We believe the findings in our study can be applied to civilians with high activity demands and even elite athletes. Return to activity is a priority for athletes and is typically addressed during the preoperative discussion. In our study, patients were permitted to begin low-impact activities, such as using a stationary bike or elliptical, starting at postoperative week 4, with resistance increased gradually each week. At postoperative week 9, those demonstrating minimal bone integration on radiograph at postoperative week 6 could progress to high-impact activities—including running, jumping, and agility drills—if tolerated, with running limited to ½ mile per day for the first week and increased by ½ mile per day each subsequent week until reaching 2 miles with minimal or no pain. Patients without evidence of osseous integration at week 6 were instructed to avoid high-impact exercise until week 12. By the 12-week postoperative visit, all patients who attended demonstrated some bone growth. Given the positive results, the protocol appears suitable for high-activity patients and elite athletes, but future studies with control groups are needed to determine if the timeline can be safely shortened.
Conclusion
Our findings suggest that MIS HV is associated with favorable outcomes in terms of pain relief, functional improvement, and faster recovery times. MIS HV for mild to moderate deformities may be better suited than open surgery for active populations such as military personnel and even elite athletes where rapid recovery and functional improvements are paramount. The active-duty population, with its specific physical demands, represents an important group for ongoing research in the context of surgical interventions for foot deformities.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251394729 – Supplemental material for Functional Recovery and Return to Duty Following Minimally Invasive Surgery for Hallux Valgus: A Retrospective Review in Active-Duty Military Personnel
Supplemental material, sj-pdf-1-fao-10.1177_24730114251394729 for Functional Recovery and Return to Duty Following Minimally Invasive Surgery for Hallux Valgus: A Retrospective Review in Active-Duty Military Personnel by Colin Mizuo, Liliya Parkman, Ashley Adams and Alyson Boudreau in Foot & Ankle Orthopaedics
Footnotes
Author Note
The views expressed in this article are those of the author and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, nor the US Government.
Ethical Considerations
Naval Medical Center Camp Lejeune’s IRB reviewed this study protocol (ID NMCCL.2022.0008) and determined it to be IRB exempt.
Author Contributions
This manuscript has not been published elsewhere, nor is it currently up for consideration at any other publication. Each author has participated in the design of the study, has contributed to the collection of the data, has participated in the writing of the manuscript, and assumes full responsibility for the content of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data Availability Statement
Permission has not been granted from the DOD to allow data sharing.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.