
Abstract
Background:
Isolated medial gutter arthritis is an uncommon subset of ankle arthritis characterized by complete loss of joint space within the medial gutter, without proximal tibiotalar joint surface narrowing or tilting. Although ankle arthrodesis and total ankle arthroplasty are conventional treatments, a promising alternative in addressing medial gutter arthritis is the combination of Dwyer calcaneal osteotomy, arthroscopic debridement, and hamstring allograft lateral ligament reconstruction. This study assesses the clinical and radiographic outcomes of this procedure with a minimum 2-year follow-up.
Methods:
Retrospective review was performed for cases done for isolated medial gutter arthritis (Takakura stage 3a) treated with a lateralizing (Dwyer) calcaneal osteotomy, anatomic lateral ligament reconstruction using hamstring allograft (ATFL/CFL), and ankle arthroscopy by a single surgeon between 2018 and 2022. Clinical patient-reported outcome measures (PROMs) were collected using Patient Reported Outcome Measurement Information System (PROMIS) and the Revised Foot Function Index Short Form (FFI-RS). Radiographic outcomes were evaluated by comparing pre- and post-operative joint space on weightbearing (WB) radiographs. Area of clear space ratio was examined on postoperative WB computed tomography (WBCT).
Results:
Six patients (mean age 64.2 years) completed follow-up at a mean of 3.9 years. Pre- and post-operative PROMs were available for 5 of 6 patients and showed significant improvement in pain and cumulative FFI-RS scores. On radiographs, tibiotalar varus tilt decreased by approximately 3 degrees, the lateral tibiotalar joint space decreased (4.7 ± 1.0 mm to 4.0 ± 1.2 mm; P = .033), and the medial clear space increased (median ~0.7 mm to 3.1 mm; n = 6; P < .05), whereas the lateral clear space modestly increased (2.2 ± 0.5 mm to 3.2 ± 0.9 mm; P = .005). The clear-space ratio (CSR) increased from 0.2 to 1.0 (n = 6; P < .05). Postoperative weightbearing CT (available in 5 of 6 patients) demonstrated a mean medial: lateral tibiotalar contact-area ratio of 0.61 ± 0.30.
Conclusion:
In this single-surgeon case series (n = 6) of Takakura 3a ankles, a lateralizing calcaneal osteotomy combined with hamstring allograft lateral ligament reconstruction and arthroscopic debridement was associated with improvements in pain, function, and radiographic alignment at a mean 3.9-year follow-up. Findings should be interpreted cautiously given the small sample size.
Level of Evidence:
Level IV, case series.
This is a visual representation of the abstract.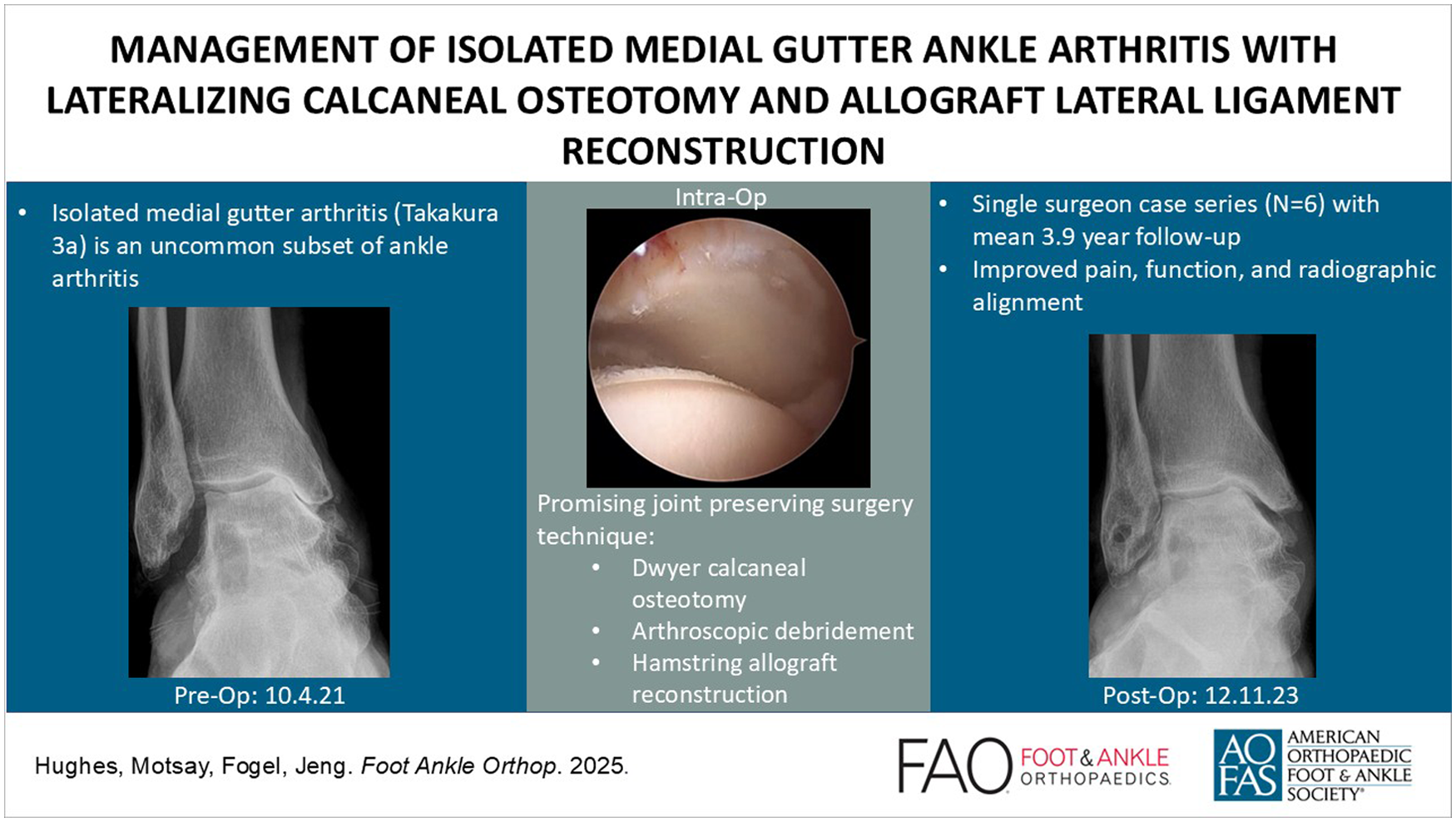
Introduction
Ankle arthritis that is isolated to the medial gutter of the ankle joint without involvement of the cartilage on the medial tibial plafond or dome of the talus is an uncommon finding. Takakura et al1,2 classified these patients with complete obliteration of the medial gutter joint space as stage 3a, whereas patients with arthritis that extended to the dome of the talus were classified as stage 3b (Table 1). Surgical indications for stage 3a ankle arthritis patients remain unclear. Modern total ankle prostheses do not resurface the medial gutter of the ankle, and ankle arthrodesis sacrifices healthy cartilage on the dorsal tibiotalar joint.
Takakura Classification: Varus-type Ankle Osteoarthritis.

Lee et al 3 reported on a case series of 11 patients with Takakura stage 2, 3a, and 3b ankle arthritis managed with joint debridement (arthroscopic or open), lateralizing calcaneal osteotomy, deltoid ligament release, and modified Broström lateral ligament reconstruction. At a mean follow-up of 22 months, American Orthopaedic Foot & Ankle Society (AOFAS) scores and the ratio of medial to lateral clear space were both significantly improved from their pre-operative values. They postulated that chronic lateral ankle instability caused these patients to have an internally rotated talus with a medially displaced heel that resulted in isolated injury to the cartilage on the medial side of the ankle joint.
The purpose of this study is to evaluate both the radiographic and patient-reported short-term outcomes of joint-preserving surgery for patients with Takakura stage 3a ankle arthritis consisting of arthroscopic debridement, lateralizing calcaneal osteotomy, and hamstring allograft lateral ligament reconstruction. We hypothesize that this surgical approach results in improved radiographic measurements and patient-reported outcomes.
Methods
Study Design
Institutional review board approval was obtained for this study. The surgical database for a single surgeon at a tertiary referral foot and ankle practice were reviewed to identify patients with Takakura stage 3a medial gutter ankle arthritis treated with a lateralizing calcaneal osteotomy, ankle arthroscopy and debridement, and hamstring allograft lateral ligament reconstruction between 2018 and 2022. This was a retrospective series with prospectively collected data. Exclusion criteria included patients whose ankle arthritis extended to the dome of the talus (stage 3b), patients with less than 2 years’ follow-up, patients with inflammatory arthritis, patients with Charcot arthropathy, and patients who had incomplete pre-operative weightbearing (WB) radiographs. A total of 6 patients were enrolled in the study. The patients signed informed consent and returned to clinic for final follow-up weightbearing radiographs of the ankle as well as clinical evaluation.
Demographic information on each patient was obtained through chart review, including age at the time of surgery, body mass index, smoking status, medical comorbidities, and any prior foot or ankle procedures. Clinical patient-reported outcome measures (PROMs) were collected pre-operatively in 5 of the 6 patients and post-operatively for all 6 patients. PROMs included both the Revised Foot Function Index Short Form (FFI-RS) and Patient Reported Outcomes Measurement Information System (PROMIS) physical function, global health, pain interference, and emotional distress forms.
Radiographic measurements were evaluated preoperatively and at the final postoperative visit on weightbearing radiographs of the ankle, including anteroposterior, mortise, and lateral views using the distance and Cobb angle tools on the MergePACS viewer. Measurements on anteroposterior radiographs made by an orthopaedic surgery fellow and a research assistant included the tibiotalar tilt angle (A, Figure 1a), medial tibiotalar joint space distance (B, Figure 1a), lateral tibiotalar joint space distance (C, Figure 1a), medial gutter and lateral gutter clear space distance at 10 mm distal to the talar dome (D and E, respectively, Figure 1a), medial gutter clear space distance obtained at both the proximal (F, Figure 1a) and distal (G, Figure 1a) third length of the medial malleolus, and the clear space ratio as described by Lee and Wapner (E:D, Figure 1a). 6 Weightbearing CT (WBCT) scans were also obtained on 5 of the 6 patients at final follow-up evaluation. The ratio of the medial gutter (2, Figure 1b) to lateral gutter (1, Figure 1b) clear space area was assessed using Curvebeam’s CubeVue software.

Radiographic measurements. (a) Measurements performed on anteroposterior view ankle radiograph: A, tibiotalar tilt angle (degrees); B, medial tibiotalar clear space (mm); C, lateral tibiotalar clear space (mm); D, lateral clear space at 10 mm distal talar dome (mm); E, medial clear space at 10 mm distal talar dome (mm); F, proximal medial clear space (mm) at one-third proximal length of medial malleolus (t); G, distal medial clear space (mm) at one-third distal length of the medial malleolus (1/3t). Clear space ratio = medial clear space (E) / lateral clear space (D). (b) Measurements performed on axial view WBCT: Slice determined at a point of established lateral and medial aspects of talus 1: lateral space clear area (mm2); 2: medial clear space area (mm2). Area of clear space ratio = medial clear space area (2) / lateral clear space area (1).
Surgical Intervention Technique
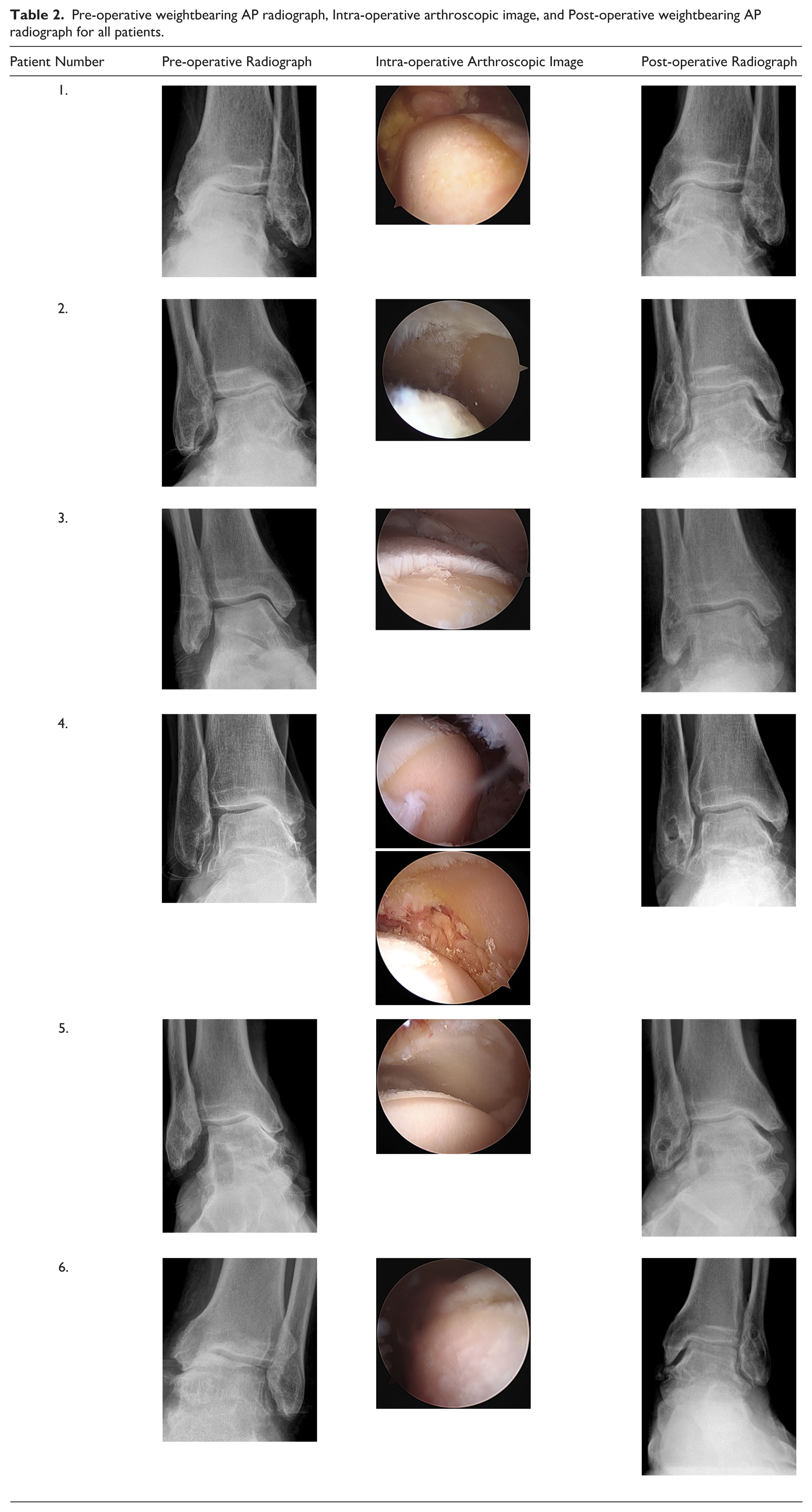
A standard diagnostic ankle arthroscopy was performed as part of the surgical procedure. The degree of chondromalacia in the medial gutter was documented (Figure 2; Table 2). A lateral based incision over the calcaneal tuberosity was used for the calcaneal osteotomy. A sagittal saw was used to perform an oblique osteotomy, and the posterior tuberosity was translated laterally and fixed with a single 7.0-mm cannulated screw.
Pre-operative weightbearing AP radiograph, Intra-operative arthroscopic image, and Post-operative weightbearing AP radiograph for all patients.

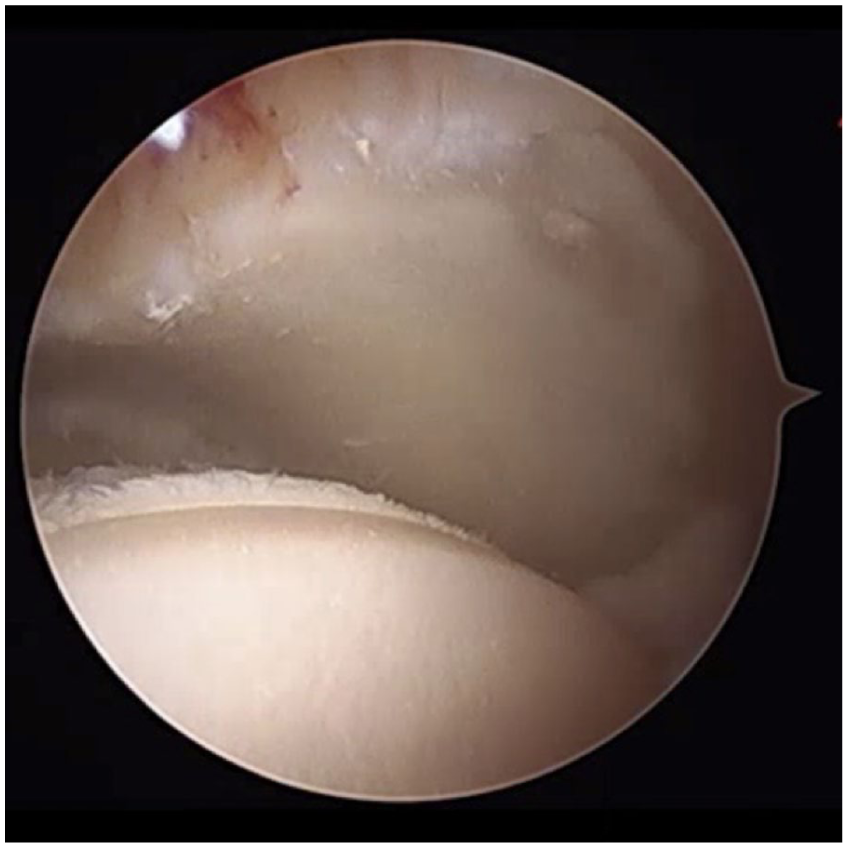
Ankle arthroscopy view of medial gutter arthritis.
A longitudinal incision was made from the front of the lateral malleolus extending distally over the lateral talar neck. Drill tunnels were made through the talar neck, lateral malleolus, and calcaneus distal to the osteotomy. We elected to use a hamstring allograft to reconstruct both the anterior talofibular and the calcaneofibular ligaments as this would be robust enough to provide stability and externally rotate the talus away from the medial malleolus. This was secured into the talar neck tunnel using a 5.5-mm interference screw. The allograft was then passed through the tunnel in the lateral malleolus. With a bump behind the ankle, maximal tension on the allograft, and maximal eversion and external rotation of the talus, the allograft was sutured to the periosteum on the front of the lateral malleolus with 2-0 non-absorbable sutures. The posterior limb of the hamstring allograft was then passed through the calcaneal tunnel and fixed with a 6.25-mm interference screw while holding maximal tension on the graft and with the ankle in maximal eversion.
Statistical Analysis
The patient characteristics were described as means with SDs, counts with percentages, or descriptive statistics depending on the data distribution. Statistics were performed using Microsoft Excel. The threshold for statistical significance was set at P <.05. PROMs and radiographic outcomes were checked for normality of the sample using a Shapiro-Wilk test. Continuous variables were expressed as mean ± SD for variables with a normal distribution or sample size. Wilcoxon signed rank (W) was used for continuous variables that did not have a normally distributed sample. Differences in pre-operative and post-operative PROMs and radiographic data were determined using paired t test for normally distributed data and the 2-tailed Wilcoxon signed rank test for non-normally distributed data. Categorical variables are expressed as counts and relative frequency (%). The average of the medial and lateral clear space area seen on WBCT was calculated and compared via the medial-lateral ratio.
Results
Six patients were identified who qualified for inclusion in this study, and all 6 agreed to participate. Five were male and 1 was female. The average age was 64.2 years (range: 52-68 years). Four patients had cardiovascular disease (1 patient had atrial fibrillation, 2 patients had hypertension, and 1 patient had hyperlipidemia). One patient had hypothyroidism, and 1 of the patients with hypertension also had a history of prostate cancer, chronic kidney disease stage 2, and multiple sclerosis. Three patients had prior ipsilateral ankle procedures (lateral ligament reconstruction/peroneal tendon repair, ankle scope with debridement, and an isolated lateral ligament reconstruction). One patient had a contralateral ankle fusion. The average follow-up time was 3.9 years after surgery (range: 2.0-6.2 years).
All patients had complete pre-operative and post-operative WB ankle radiographs (Figure 3; Table 2). The medial gutter clear space data was found not to be normally distributed. Thus, Wilcoxon signed-rank test was used for analysis. There was a statistically significant increase in the medial gutter clear space from 0.7 to 3.1 mm between pre-operative and post-operative measurements (n = 6, W = 0, P < .05). The lateral gutter clear space measurements, which were normally distributed, also demonstrated a small but statistically significant increase (2.2 mm ± 0.5 to 3.2 mm ± 0.9; P = .005). The clear space ratio (ratio of medial clear space to lateral clear space) measured 10 mm distal to the talar dome significantly increased from 0.2 to 1.0 (n = 6, W = 0, P < .05).

Example of pre-operative and post-operative anteroposterior and mortise weightbearing radiographs. Panel A demonstrates patient images at 2 years post-op. Panel B demonstrates long-term results of a different patient’s images with follow-up to 5 years 9 months post-operation.
There was a statistically significant decrease in pre-operative to post-operative tibiotalar tilt angle (5 ± 0 degrees of varus to 2 ± 2 degrees of varus; P = .016). The lateral tibiotalar joint space decreased significantly at final follow-up (4.7 mm ± 1.0 to 4.0 mm ± 1.2; P = .033). The other measurements recorded did not change significantly.
Five of the 6 patients had a post-operative WBCT. The average medial clear space area was 69 mm2. The average lateral clear space area was 113 mm2. The ratio of the average medial to lateral clear space area as calculated on WBCT was 0.6 ± 0.3.
Five of the 6 patients completed PROMs pre-operatively. These were statistically analyzed with their post-operative values. FFI-RS pain score and cumulative score both improved significantly. The FFI-RS pain score decreased from 18.6 ± 3.7 to 13.0 ± 5.9 (P = .046). The FFI-RS cumulative score decreased from 94.6 ± 22.5 to 68.0 ± 31.0 (P = .011). None of the PROMIS scores reached statistical significance.
Discussion
Isolated medial gutter arthritis (Takakura stage 3a) is an uncommon subset of ankle arthritis characterized by loss of joint space within the medial gutter. 7 Patients with hindfoot varus malalignment from chronic ankle instability are particularly prone to developing medial gutter arthritis.4-6 The altered alignment results in internal rotation and possible varus tilt of the talus within the mortise, changing joint contact pressure and increasing the risk for degenerative changes.3,7,8 The aim of this study was to assess short-term outcomes of joint-preserving surgery using hamstring allograft lateral ligament reconstruction in conjunction with a lateralizing calcaneal osteotomy in this population. In our 6-patient series, pain and cumulative FFI-RS scores improved, tibiotalar varus tilt decreased, and medial clear space and CSR increased, consistent with off-loading the medial gutter.
Supramalleolar osteotomies (SMOs) have been used to treat asymmetric ankle arthritis with varying success as reported in the literature.1,2,9-11 Tanaka et al 1 evaluated the impact of a low tibial osteotomy for varus ankle osteoarthritis. Based on their findings, patients whose arthritis had advanced to the upper surface of the dome of the talus (stage 3b) had inferior results. Although our study did not use an SMO, their findings highlight the importance of patient selection when choosing joint-sparing procedures for the management of asymmetric ankle osteoarthritis. Only patients with ankle arthritis isolated to the medial gutter, stage 3a, were included in this current study. Knupp et al 9 also looked at the impact of SMO for early and mid-stage asymmetric varus and valgus ankle arthritis. In their study, 7 ankles were Knupp Type III with joint space narrowing found mainly in the medial gutter, the equivalent of Takakura stage 3a. They found that these patients had worse outcomes and concluded that indications for SMO in this difficult subset of patients were very limited. Knupp et al 9 specifically described degenerative changes located in the medial gutter of the ankle joint as a risk factor for failure with SMO-type procedures. Lee et al’s 3 series of medial ankle osteoarthritis due to chronic lateral ankle instability evaluated the results of patients after undergoing joint debridement, cheilectomy, calcaneal osteotomy, deltoid release, and modified Broström lateral ligament reconstruction. There were 11 patients of various Takakura stages included in the study (stage 2 n = 4; stage 3a n = 2; stage 3b n = 5) who were followed for an average of 22.3 months. They found a statistically significant improvement in the AOFAS score at final follow-up. The radiographic results showed a significant decrease in mean tibiotalar tilt angle, increase in mean medial clear space, decrease in lateral clear space, and an improvement in the medial to lateral clear space ratio. Our study demonstrates similar findings with decreased tibiotalar tilt angle, increase in the mean medial clear space, and improvement in the medial to lateral clear space ratio. Interestingly, our data show a small but significant increase in the lateral clear space of 1 mm. This discrepancy from Lee et al’s findings could in part be due to measurement error with the small sample size or might also be explained by a change in the projection of the lateral wall of talus within the mortise as it is externally rotated by the anterior limb of the hamstring allograft used for ligament reconstruction in our study.
To our knowledge, this is the largest case series of Takakura stage 3a ankles managed by lateralizing calcaneal osteotomy, arthroscopic debridement, and hamstring allograft ligament reconstruction reported in the literature. By analyzing a single-surgeon database, the surgeries performed as part of this study used a standard technique. Further, using the hamstring allograft for a robust lateral ligament reconstruction rather than imbricating degenerative native tissue allows for improved external rotation of the talus away from the medial malleolus to offload the arthritic area. This study also used validated patient-reported outcome measures (FFI-RS and PROMIS) to assess the results of the surgery compared with AOFAS scores previously reported in the literature. This study has notable limitations, however. Our small sample size is a significant limitation. Additionally, our cohort is predominantly male. Furthermore, there were no pre-operative WBCTs obtained in our cohort. In the future, it would be valuable to have both pre- and post-operative WBCTs to assess the amount of correction obtained.
Conclusion
The combination of a lateralizing calcaneal osteotomy, hamstring allograft lateral ligament reconstruction, and arthroscopic ankle debridement may be an effective joint-sparing treatment option to address isolated medial gutter ankle arthritis with an associated hindfoot varus deformity. Based on our cohort of 6 patients, this approach was associated with significant improvement in patient-reported pain, overall functional status, and radiographic outcomes at a mean of 3.9 years. Future studies would benefit from pre-operative WBCT scans, a larger number of subjects, and prospectively collected data.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251394726 – Supplemental material for Management of Isolated Medial Gutter Ankle Arthritis With Lateralizing Calcaneal Osteotomy and Allograft Lateral Ligament Reconstruction
Supplemental material, sj-pdf-1-fao-10.1177_24730114251394726 for Management of Isolated Medial Gutter Ankle Arthritis With Lateralizing Calcaneal Osteotomy and Allograft Lateral Ligament Reconstruction by Meghan Hughes, Morgan Motsay, Jessa Fogel and Clifford L. Jeng in Foot & Ankle Orthopaedics
Footnotes
Acknowledgements
We would like to recognize Dr. John Campbell for his support with editing this manuscript. We greatly appreciate his time and effort.
Correction (June 2026):
This article has been updated to include an Acknowledgment.
Ethical Considerations
This study was approved by the institutional review board at Mercy Medical Center.
Informed Consent
Informed consent was obtained from each patient. This explained the goals of the study. Participation was voluntary and individuals could withdraw without penalty or change in the standard of care.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data Availability Statement
De-identified data are available if needed.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.