
Abstract
Background:
Very few studies reported outcomes of common conservative surgeries with antibiotic-impregnated cement when treating diabetic foot osteomyelitis (DFO). The aim of this descriptive study is to report the results of the association of cement with a specific type of toe-sparing resection, combining total metatarsectomy/phalangectomy (internal pedal amputation) with partial bone excision, for acute on chronic forefoot DFO.
Methods:
Six patients with confirmed acute on chronic DFO were included. A probe-to-bone test was performed for open wounds. For all patients, radiographs, magnetic resonance imaging (MRI), and pathology were conducted in search of osteomyelitis signs. The level of resection was defined as 1 cm away from the contrast enhancement shown on MRI. The polymethylmethacrylate (PMMA) cement was prepared with 2 g of vancomycin before being placed in the defect. A minimum period of 6 months of clinical follow-up was set.
Results:
All patients demonstrated wound healing at last follow-up with normalized C-reactive protein. There were no clinical signs of osteomyelitis recurrence. One wound infection was recorded 4 weeks postoperatively and treated successfully with debridement and lavage. None of the cement had to be removed or exchanged. Subjectively, 5 patients were extremely satisfied scoring 5/5 on Likert scale, and 1 patient was moderately satisfied (3/5). All patients were able to walk with full weight using insoles.
Conclusion:
This preliminary report demonstrated that PMMA cement could be a viable option when used to locally control infection following an internal pedal amputation for acute on chronic DFO of the toes. In addition to the high rate of healing, the esthetical result was highly appreciated by the patients.
Level of Evidence:
Level IV, case series.
Keywords
Introduction
Diabetic foot ulcers (DFUs) and infections (DFIs) are difficult to treat and prone to recurrence. These complications could lead to high rates of amputation and mortality.8,21 When diagnosis is established early, acute DFI could be treated conservatively with a combination of antibiotics, in-office debridement, off-loading, and repeated topical dressings. 9 However, in chronic DFI and in particular when osteomyelitis (DFO) is present, conservative standard of care often fails. Surgery has been shown to yield good outcomes when treating hard-to-heal ulcers and chronic DFO.2,17-19 Depending on the status of the soft tissues, toe-sparing resection or amputation are suggested. 1 When the soft tissues could be preserved, toe-sparing resection based on infected bone resection, either partial or total (internal pedal amputation), has been shown to generate good outcomes in terms of infection control and ulcer healing.16,20
Compared with other foot locations, the forefoot bears the highest frequencies of DFU, DFI, and DFO that could reach 90%. 6 Very few published reports described the outcomes of bone resection associated with antibiotic-impregnated bone cement for mechanical support and local control of infection, at this location.4,7 These studies were mostly focused on the use of cement following metatarsophalangeal joint resection of the hallux.4,7 None included the results of cement use following total resection of metatarsals and/or phalanges in treating acute on chronic DFO.
This case series reports the outcomes of toe-sparing resection based on the combination of total and partial bone resection associated with antibiotic-impregnated cement, for the treatment of acute on chronic DFO.
Methods
Study Design
This is a prospective consecutive case series of patients treated in our institution approved from the Institutional Ethical Board of our university hospital. Electronic charts and radiologic images of patients diagnosed with acute on chronic DFO of the forefoot were checked. Written consent forms were obtained from patients who agreed to publish radiologic images of their cases. This study followed the guidelines of the Joanna Briggs Institute Checklist for case series studies. 11
Patient Selection
Patients with acute on chronic DFO of the forefoot distal to the tarsometatarsal joint were selectively included. Chronic DFO was defined as a DFO for more than 6 months diagnosed with either probe-to-bone test, radiographic / magnetic resonance imaging (MRI) signs, and/or pathology. Acute on chronic DFO was defined as cases with a history of treated or untreated chronic DFO having acute clinical signs of infection at presentation with positive MRI signal. Patients with healed ulcers or open wounds were accepted for inclusion. Patients treated with toe-sparing resection encompassing partial and total bone resection were candidate for inclusion only if cement was used as a space filler. Partial and total bone resection was limited to metatarsals and/or phalanges. The term internal pedal amputation refers to a type of toe-sparing excision of a whole phalanx (phalangectomy) or a whole metatarsal (metatarsectomy), with or without additional partial phalangectomy or partial metatarsectomy. It is usually indicated when the surrounding soft tissues are not, or mildly, affected, with infection and/or necrosis. Cases of chronic DFO without clinical or MRI signs of acute infection were excluded. Acute DFO with no history or MRI signs of chronic osteomyelitis were also disregarded. Figure 1 displays the flowchart of patient selection. In all cases, the peripheral arterial status was clinically evaluated by the vascular team prior to surgery coupled with an Ultrasound Doppler. Following the vascular appraisal, no arteriogram was required. A minimum period of 6 months of clinical follow-up after surgery was compulsory for inclusion.

Flowchart of patient selection.
Osteomyelitis diagnosis
A probe-to-bone test was performed for open wounds. For all patients, radiographs and MRI were conducted in search of osteomyelitis signs. The initial diagnosis of acute on chronic DFO was based on clinical and MRI findings. The final diagnosis was confirmed based on the pathology examination of bone specimens—acute reaction on chronic inflammation suggestive of acute on chronic DFO.
Procedure description
First, the open wound was excised or the healed scar was opened, and then the skin was enlarged for proper bone resection. The first step was bone excision involving one total bone (internal pedal amputation) with one partial bone. The level of resection was defined as 1 cm away from the contrast enhancement shown on MRI. This cut-off value for resection level has been used in our clinic since many years, based on the frequency of infection recurrence and the need for amputation when treating severe DFI. 22 The second step consisted in preparing the polymethylmethacrylate (PMMA; Gentafix [Teknimed, L’Union, Occitanie, France]) cement of 40 g mixed with 2 g of vancomycin. Care was taken to fill the space with a cement volume less than the void volume for easy skin closure. To achieve this, the volume of the cement was estimated intraoperatively as the half volume of the defect. Time was allowed for the cement to harden outside the surgical site. The third step is the cement implantation following excision of all suspected or infected soft tissues. Bone specimens were cut in half and sent to microbiology and pathology labs. The excised soft tissues were sent to microbiological examination. Postoperative antibiotic therapy was administered for 3 weeks and adjusted based on antibiograms. All patients were allowed for postoperative partial weightbearing using heel shoes for 6 weeks. Afterwards, full weightbearing was allowed using custom-made insoles as inserts for common diabetic shoes. Figures 2 and 3 illustrate one clinical case of acute on chronic DFO treated with internal pedal amputation and cement.

Case imagery of acute on chronic DFO of the metatarsal and first phalanx of the second ray. DFO, diabetic foot osteomyelitis.

Postoperative radiographs after internal pedal amputation with cement placement.
Data Extraction
The following information were retrieved: demographic data, ulcer duration, osteomyelitis duration, duration of antibiotics, previous microbiology results, C-reactive protein (CRP), creatinine, and HbA1c level. Radiographic and MRI findings were documented. Postoperative bacteria culture and pathology results were recorded.
Outcome Definition
Infection recurrence was defined as primary outcome. Reintervention and wound complications were set as secondary outcome. Infection resolution was assessed using clinical examination and CRP level. Patient satisfaction, based mainly on the ability to ambulate, was appraised by an independent assessor and rated on a Likert scale ranged from 1 (extremely dissatisfied), 2 (dissatisfied), 3 (moderately satisfied), 4 (satisfied), to 5 (extremely satisfied).
Statistical Analysis
The StatsDirect software (Cambridge, United Kingdom) was used to generate descriptive statistics.
Results
Characteristics of the Sample
Of the 122 forefoot DFO cases, there were 6 patients (5 males and 1 female) with a mean age of 63.5 ± 17.4 years (median = 67.5 years, IQR = 22), fulfilling the criteria and included in this series. There was similar side involvement, 3 on each foot side. The mean HbA1c was 7.2 ± 0.4 (median = 7.15, IQR = 0.7). The mean CRP level was 20.1 ± 14.6 mg/L with a cut-off ˂5 (median = 22, IQR = 10). The mean creatinine level was 1.1 ± 0.34 mg/dL. Four patients presented with an open wound while 2 had a healed wound at the time of presentation. The probe-to-bone test was positive in those with an open wound whereas the other 2 patients presented with signs of sausage toe. The involved rays, wound sites, and bone resection levels are shown in Table 1.
Characteristic of the patients with acute on chronic DFO.
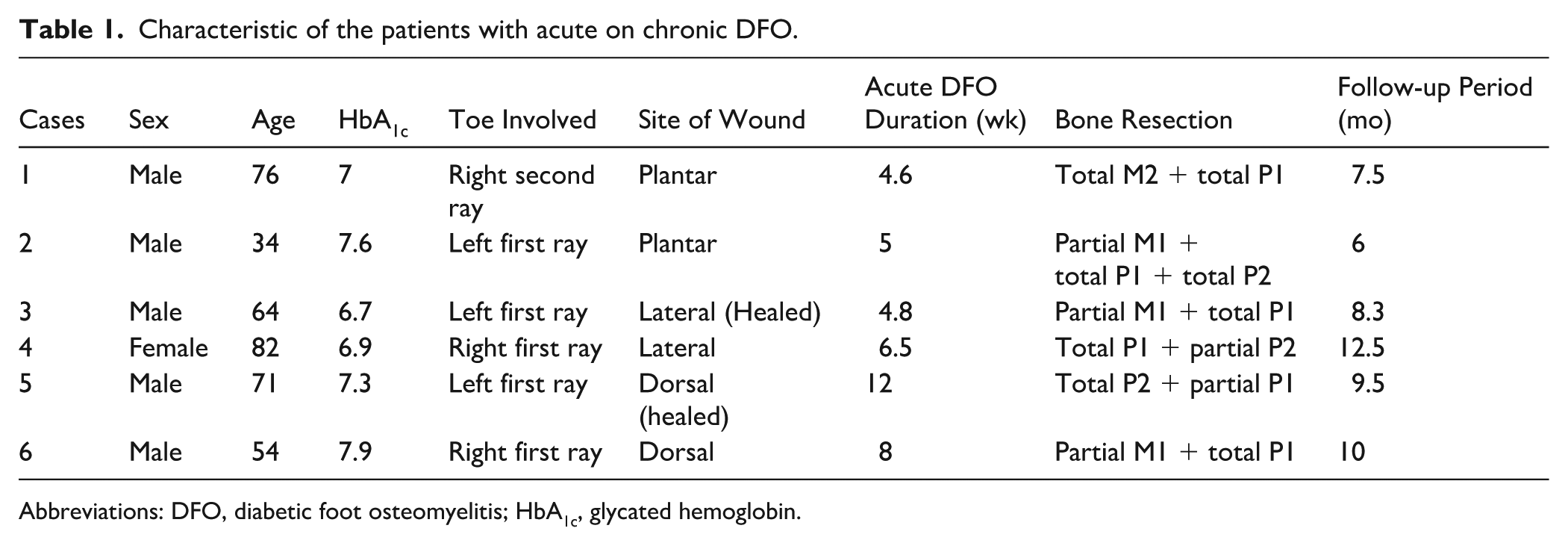
Abbreviations: DFO, diabetic foot osteomyelitis; HbA1c, glycated hemoglobin.
Imagery Findings
Five cases (83.3%) presented clear radiologic signs of chronic osteomyelitis, mostly irregularity, sclerosis, and fragmentation. All cases showed signs of acute on chronic osteomyelitis on MRI. The extent of postcontrast enhancement of the bone marrow was used for the level of resection; the bone cut was performed 1 cm away.
Micro-organism and Pathology Results
A bacterial micro-organism was found in all cases. All specimens showed signs of acute on chronic inflammation on pathologic examination of the resected bones with free margins.
Outcomes
All patients demonstrated wound healing at last follow-up with normalized C-reactive protein with a mean of 2.1 ± 2.5 mg/L at last follow-up. There were no clinical signs of osteomyelitis recurrence. One wound infection was recorded 4 weeks postoperatively and treated successfully with debridement and lavage. The mean healing time for the remaining patients was 20 ± 5.5 days. In 1 patient, there was profuse oozing from the wound for the first 2 weeks because of the cement presence; multiple cultures came negative. None of the cement had to be removed or exchanged during the follow-up period. Subjectively, 5 patients were extremely satisfied scoring 5/5 on Likert scale; 1 patient was moderately satisfied (3/5). All patients were able to walk with full weight after 6 weeks of surgery. Micro-organisms found in culture were as follows: Enterococcus faecalis, Escherichia coli, Enterobacter cloacae, Proteus mirabilis, Staphylococcus aureus, and Proteus hauseri.
Discussion
Our results showed good outcomes when compared to those reported by the recent meta-analysis of Yammine et al 23 following bone resection with cement void filling space in DFO. Although the weighted healing rate has been reported to be 85.2% in their review, our series showed 100% infection healing. In addition, we did not encounter some of the complications noted in this systematic review, such as cement exchanged (8.2%), cement removal (24.4%), or minor amputation (13.4%). 23 On the other hand, one additional surgery in the form of debridement and lavage was encountered in our series.
There are 2 objectives when using an antibiotic-impregnated cement following infected bone resection: dead space filling and local infection control. Although various methods are available to fill bone defects such as autologous/autogenous bone graft or synthetic bone, 5 bone cement particularly PMMA demonstrated great efficacy when managing osteomyelitis.13,15 In addition to its role in local infection control,3,14 the mechanical properties of PMMA demonstrated enough stiffness when filling the void after bone resection. 12 This property may help load transfer that could authorize a form of weightbearing. 14
In contrast to the commonly used metatarsal head resection and resection arthroplasty, internal pedal amputation combined with partial resection of another adjacent bone in the forefoot usually result in significant bone void. Although most studies reporting the outcomes of such toe-sparing resection procedures did not use cement as a complementary surgical step, we believe that bone defects following more extensive bone resection such as performed in the forefeet of our patients would be better filled with cement for enhanced functionality of the foot. In our diabetic foot clinic, we extended the indication of cement filling to cases where the needed bone excision was extensive.
Furthermore, the cement may allow motion and could function as a pseudo-joint between the resected bones. 10 Long-term functional results seem to be promising as reported by Elmarsafi et al 7 ; patients who received a permanent or temporary cement spacer maintained ambulation with the aid of inserts, bracing, or other assistive devices. In addition, the internal pedal amputation could leave great psychological impact; by leaving the outer soft tissues of the toe, the esthetical results were highly appreciated by the patients.
Lastly, when ankle equinus is associated with neuropathic ulceration, lengthening of the Achilles through its tendon or via gastrocnemius recession could be indicated, 12 in concomitance with internal pedal amputation.
Several limitations are to be acknowledged. The descriptive type of study design and the sample size would be major restrictions to validate the results. However, stating this study as a preliminary report goes with the recognition of limitations in terms of inference and generalizability. Some elements should be noted in order to put other limitations into context. The internal pedal amputation type of toe-sparing surgery has narrow indications and is rarely practiced by foot and ankle surgeons. Few reports included acute on chronic DFO and few reported cement use to fill bone defect following bone resection in DFO. In this high-risk and frail population, every effort should be made to improve their functionality when aiming for limb-sparing approach in treating diabetic foot infection.
Conclusions
This preliminary report demonstrated that PMMA cement could be a viable option when used to locally control infection following an internal pedal amputation for acute on chronic DFO of the toes. In addition to the high rate of healing, the esthetical result was highly appreciated by the patients.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251394009 – Supplemental material for Acute on Chronic Diabetic Forefoot Osteomyelitis Treated With Internal Pedal Amputation and Cement: A Preliminary Report
Supplemental material, sj-pdf-1-fao-10.1177_24730114251394009 for Acute on Chronic Diabetic Forefoot Osteomyelitis Treated With Internal Pedal Amputation and Cement: A Preliminary Report by Kaissar Yammine, Joseph Mouawad, Youssef Jamaleddine and Chahine Assi in Foot & Ankle Orthopaedics
Footnotes
Acknowledgements
Not applicable
Ethical Considerations
Ethical approval was obtained from the institutional review board (LAUMCRH.KY2.25/Nov/2020).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Informed consent
Informed consent statements were obtained from the patients.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.