
Abstract
Background:
Progressive collapsing flatfoot deformity (PCFD) is a complex pathophysiologic condition, with many different treatment options. The complexity of the condition and variety of treatments can greatly impact patient-reported outcomes (PROs), along with individual patient characteristics. The purpose of this study was to examine PROs in patients receiving surgical treatment for PCFD and compare those outcomes with patients with ankle instability or hindfoot arthritis.
Methods:
The Orthopaedic Foot and Ankle Outcomes Research (OFAR) Network database was queried to identify all patients with flexible PCFD, ankle instability, or hindfoot arthritis procedures from October 2017 to October 2019 with at least 12 months of follow-up. Patient satisfaction was also measured at both 6 months and 12 months. Changes in PROs and satisfaction were assessed over time and compared between those with PCFD and those with ankle instability or hindfoot arthritis using generalized logistic regression and estimating equations.
Results:
After adjusting for age, sex, body mass index, hypertension, autoimmune conditions, and type 2 diabetes, there were significant improvements in average Global Physical Health (P < .0001), Pain Interference (P < .0001), Pain Intensity (P < .0001), and Physical Function (P < .0001) for both groups following surgery. Changes in Pain Intensity scores between the baseline and 12-month visits were significantly different between the 2 groups (P = .0286), with those receiving PCFD surgery reporting greater change. The odds of surgical satisfaction was significantly lower at 12 months compared to 6 months for both groups.
Conclusion:
This study found that patients who underwent surgical management of PCFD demonstrated significant improvements in their PROs and postoperative satisfaction; however, there were lower odds of satisfaction at 12 months compared with 6 months. Additionally, PCFD patients showed greater improvement in Pain Intensity from baseline to follow-up, whereas other PROMIS domains improved similarly between groups.
Keywords
Introduction
Progressive collapsing flatfoot deformity (PCFD), also known as adult acquired flatfoot deformity, is a 3-dimensional deformity of the foot that results in hindfoot valgus, forefoot abduction, and midfoot varus.8,10,11,16,23 The pathophysiology associated with the condition is complex and poorly understood and can involve misalignment or deformation of osseous and articular structures, including the subtalar posterior facet and calcaneocuboid joint, and dysfunction of soft tissue structures, including the gastrocsoleus complex, posterior tibial tendon, and the spring ligament complex.2,8,11,13,16,22 Given the complex pathophysiologic nature of the condition, many conservative and surgical treatment options have been suggested for the treatment of PCFD. These treatment goals frequently include preserving joint range of motion, relieving patient symptoms, restoring adequate foot alignment and balance, and/or preventing disease progression.1,3,7,12,16,17,21,25,28,29
Although multiple studies have focused on radiographic outcomes and complications associated with the various treatment options available for PCFD, very few have demonstrated how these treatment options affect patient-reported outcome (PROs).3,4,6,9,29 Given the increasing use of PROs in the assessment of the utility of a given treatment option, it is worth examining the effect of various factors and treatments associated with PCFD on patients' PROs. The purpose of this study was to evaluate the effects of comorbid conditions, types of treatment, and stage of disease on PROs, via the Patient-Reported Outcomes Measurement Information System (PROMIS), in patients with a diagnosis of PCFD, and to compare these PROs to those with ankle instability or hindfoot arthritis. These conditions were chosen for the comparison group because of similarities with PCFD, specifically the effect on the hindfoot with altered mechanics of the subtalar joint and overall gait mechanics for hindfoot arthritis and the soft tissue component to the disease process with posterior tibial tendon, gastrocsoleus complex, and spring ligament of ankle instability. We hypothesized that PROMIS Physical Function and overall quality of life PROs will be lower in PCFD patients who have an increased number of comorbidities or more invasive surgical treatments. Additionally, we hypothesized that those with PCFD treated surgically will have worse postoperative PROMIS scores and less improvement compared to those with ankle instability or hindfoot arthritis treated surgically.
Methods
Sample Information
The Orthopaedic Foot and Ankle Outcomes Research (OFAR) Network database was queried to identify all patients included in the flexible PCFD, ankle instability, or hindfoot arthritis procedure pathways from October 2017 to October 2019.14,15 Among the 217 patients captured in the initial query, patients were excluded for the following: included in multiple procedure pathways (n = 6), missing information about the index procedure (n = 5), patients undergoing repeat or revision procedure(s) following an index procedure that was not initially included in the OFAR database (n = 9), or missing all postoperative patient-reported outcome measures (3-, 6-, and 12-month visits, n = 79). The flatfoot group included 23 patients, and the ankle instability/hindfoot arthritis group included 95 patients.
All patients from the OFAR network study completed a preoperative survey and postoperative surveys at 3, 6, and/or 12 months. Six PROMIS metrics were collected at each survey visit, including 3 computerized adaptive tests (CAT), Physical Function, Pain Interference, and Depression, as well as 3 short forms, Pain Intensity, Global Physical Health, and Global Mental Health. The primary outcome of this study was the difference in postoperative Physical Function scores between the 2 study groups. The other 5 PROMIS metrics were included as secondary endpoints. Patient satisfaction (yes/no) with the outcome of the procedure (Are you satisfied with the outcome of the procedure you underwent for your foot and/or ankle?) was also evaluated at the 6- and 12-month visits.
Power Analysis
The primary purpose of this study was to evaluate changes in self-reported Physical Function across the study visits (baseline, 3, 6, and 12 months) among patients with flat foot deformities (n = 23) vs patients with ankle instability or hindfoot arthritis (n = 95). We anticipated that self-reported Physical Function would be similar in the 2 groups at baseline (0% difference) but would differ between groups by at least 20% at the 3-, 6-, and 12-month visits. Based on these assumptions, the proposed study had greater than 92% power to reject the null hypothesis that changes in Physical Function across the visits do not differ by group (group × time interaction). The calculations assumed a common SD of 10, the correlation between consecutive visits was 0.25, and mean values in the reference group, ankle instability/hindfoot arthritis, were 41.0 at baseline, 44.5 at 3 months, 46.2 at 6 months, and 47.7 at 12 months. Mean values for the reference group were estimated based on average Physical Function scores by visit among all ankle/hindfoot disorders included in the OFAR database. Power calculations for this longitudinal design were calculated with GLIMMPSE. 20
Statistical Analysis
Descriptive statistics were used to summarize the demographics and clinical characteristics in each of the 2 groups. Linear mixed models were used for testing differences across study visits in both the primary PRO measurement, Physical Function, and the secondary PROMIS metrics. For each linear mixed model, the unstructured covariance structure was used to account for repeated measures. To address our primary hypothesis, we tested whether changes in PROMIS scores across the study visits differed between the groups (group × time interaction). Generalized logistic regression models were used to test for group differences in the proportion of patients who reported they were satisfied with the outcome of their procedure (extremely satisfied or moderately satisfied vs a little bit satisfied, neutral, a little bit unsatisfied, or moderately unsatisfied) at the 6- and 12-month postoperative visits. Generalized estimating equations were used to account for repeated measures. Age, sex, body mass index, hypertension, autoimmune conditions, and type 2 diabetes were adjusted for in all models; other patient characteristics were not included in models because of the low prevalence in the sample. Statistical analyses were performed with SAS Enterprise Guide, version 8.3 (SAS Institute, Cary, NC).
Results
Patient Population
A total of 118 patients met the inclusion criteria. On average, the PCFD group was older and was associated with higher self-reported Pain Intensity scores at baseline, as displayed in Table 1. Autoimmune conditions and type 2 diabetes were significantly more prevalent in the ankle instability/hindfoot arthritis group (Table 1). Additional information about the severity of conditions within the 2 groups as well as additional procedures performed during the index surgery are described in greater detail in Supplementary Tables 1 to 5.
Summary of Demographics and Clinical Characteristics Across the Procedure Groups. a

Abbreviation: BMI, body mass index; PROMIS, Patient-Reported Outcomes Measurement Information System.
Boldface indicates significance.
P value based on Fisher exact test.
PROMIS scores were collected at baseline.
Patient Reported Outcomes
After adjusting for age, sex, BMI, hypertension, autoimmune conditions, and type 2 diabetes, there were significant improvements in average Physical Function (P < .0001) Global Physical Health (P < 0.0001), Pain Interference (P < .0001), and Pain Intensity (P < .0001) for both groups following surgery (Figures 1-6). There was no significant change in Global Mental Health (P = .6998) or Depression (P = .4509) scores following surgery. Average changes in PROMIS metrics between the baseline and 12-month visits are listed in Table 2. Although group differences were not significant (data not shown), all patients receiving surgical intervention reported significantly increased physical function and health and significantly decreased pain interference and intensity (Table 2).

Changes in PROMIS Physical Function scores by group and study visit. Error bars represent 95% CIs. All estimates were adjusted for age, sex, body mass index, high blood pressure, and the presence of an autoimmune condition and/or type 2 diabetes. AI/HA, ankle instability/hindfoot arthritis; FF, flatfoot; PROMIS, Patient-Reported Outcomes Measurement Information System.

Changes in PROMIS Global Physical Health scores by group and study visit. Error bars represent 95% CIs. All estimates were adjusted for age, sex, body mass index, high blood pressure, and the presence of an autoimmune condition and/or type 2 diabetes. AI/HA, ankle instability/hindfoot arthritis; FF, flatfoot; PROMIS, Patient-Reported Outcomes Measurement Information System.

Changes in PROMIS Depression scores by group and study visit. Error bars represent 95% CIs. All estimates were adjusted for age, sex, body mass index, high blood pressure, and the presence of an autoimmune condition and/or type 2 diabetes. AI/HA, ankle instability/hindfoot arthritis; FF, flatfoot; PROMIS, Patient-Reported Outcomes Measurement Information System.
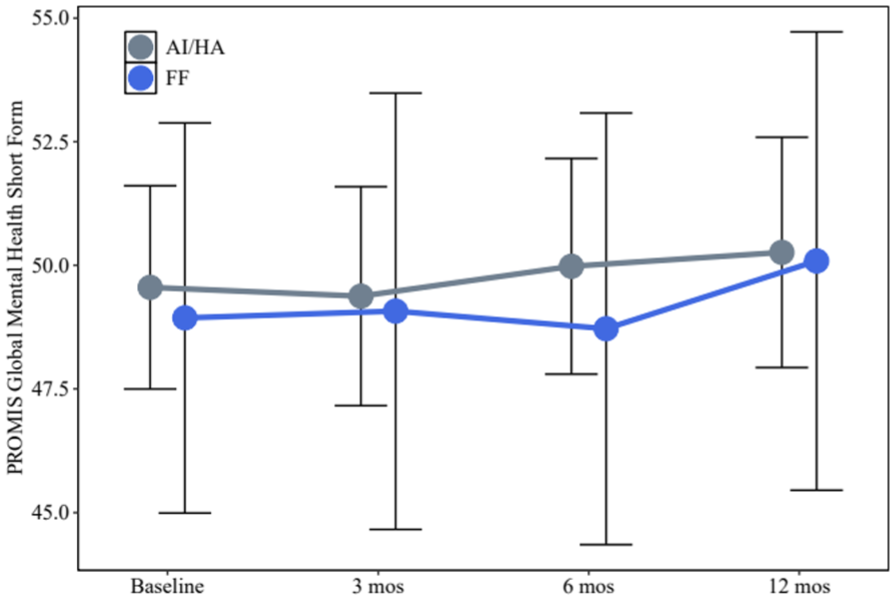
Changes in PROMIS Global Mental Health scores by group and study visit. Error bars represent 95% CIs. All estimates were adjusted for age, sex, body mass index, high blood pressure, and the presence of an autoimmune condition and/or type 2 diabetes. AI/HA, ankle instability/hindfoot arthritis; FF, flatfoot; PROMIS, Patient-Reported Outcomes Measurement Information System.

Changes in PROMIS Pain Interference scores by group and study visit. Error bars represent 95% CIs. All estimates were adjusted for age, sex, body mass index, high blood pressure, and the presence of an autoimmune condition and/or type 2 diabetes. AI/HA, ankle instability/hindfoot arthritis; FF, flatfoot; PROMIS, Patient-Reported Outcomes Measurement Information System.

Changes in PROMIS Pain Intensity Scores by group and study visit. Error bars represent 95% CIs. All estimates were adjusted for age, sex, body mass index, high blood pressure, and the presence of an autoimmune condition and/or type 2 diabetes. AI/HA, ankle instability/hindfoot arthritis; FF, flatfoot; PROMIS, Patient-Reported Outcomes Measurement Information System.
Average Change in PRO Measures Between the Baseline and 12-Month Visit (Baseline to 12-Month Visit) After Adjusting for Age, Sex, BMI, High Blood Pressure, Presence of Autoimmune Condition, and Type 2 Diabetes.

Abbreviations: BMI, body mass index; CAT, computer-aided test; PRO, patient-reported outcome.
Positive values (+) represent deterioration, negative (–) values represent improvement.
Positive values (+) represent improvement, negative (–) values represent deterioration.
We also tested whether changes in PRO scores between the baseline and 12-month visit differed by group (visit × group interaction). Physical Function (visit × group P = .0836) and Global Physical Health (visit × group P = .2782) increased in both groups, remaining slightly higher in the AI/HA group until the12-month visit (Figures 1 and 2). Depression (visit × group P = .9008) and Global Mental Health (visit × group P = .9245) scores improved across the study period in both groups, with the ankle instability/hindfoot arthritis group maintaining slightly better scores than the flatfoot group throughout (Figures 3 and 4). Pain Interference (visit × group P = .4043) scores decreased in both groups, with the flatfoot group starting at a more severe pain level and ending at a similar point as the other group (Figure 5). However, changes in Pain Intensity scores between the baseline and 12-month visits were significantly different between the two groups (visit × group P = 0.0286). The flatfoot group started with substantially higher pain intensity, but they decreased to similar levels as the ankle instability/hindfoot arthritis group at 3- and 12-month visits, demonstrating a higher magnitude of improvement (Table 3 and Figure 6).
Average Change From Baseline in PROMIS Pain Intensity Scores Within the 2 Groups After Adjusting for Age, Sex, BMI, High Blood Pressure, Presence of Autoimmune Condition, and Type 2 Diabetes. a

Abbreviations: BMI, body mass index; PROMIS, Patient-Reported Outcomes Measurement Information System.
Positive values (+) represent improvement, negative (–) values represent deterioration
Satisfaction
On average, there was no difference in the odds of being satisfied with outcome of their foot and ankle procedure among patients in the PCFD group compared to patients in the ankle instability/hindfoot arthritis group (odds ratio: 0.71, 95% CI: 0.22-2.33). In both groups, the odds of being satisfied with the outcome of the procedure was significantly lower at the 12-month visit compared to the 6-month visit (odds ratio 12-month vs 6-month: 0.39, 95% CI: 0.18-0.84). Although changes in satisfaction across the study visits were not statistically significant for either group (P = .0637), satisfaction remained constant in the flatfoot group whereas it tended to decrease between the 6- and 12-month visits in the ankle instability/hindfoot arthritis group (data not shown).
Discussion
The effect of surgical treatment on PROs for PCFD has previously been investigated in a limited fashion. de Cesar Netto et al, 6 Nayak et al, 24 and Conti et al 4 found that patients treated surgically for flexible PCFD experienced significant postoperative improvements in multiple PROs, particularly Pain Interference and Physical Function scores; nevertheless, Conti et al found no significant improvement in postoperative Depression scores. It should be noted these studies did not control for potential confounding factors, except Conti et al, 4 who controlled for the type of reconstruction performed. When controlling for multiple confounding factors, this study found those undergoing surgical treatment for PCFD significantly improved in their postoperative Global Physical Health, Pain Interference, Pain Intensity, and Physical Function scores compared with their preoperative values. Between-group differences were not detected for most domains; the only significant group × visit effect was for Pain Intensity, reflecting greater improvement in PCFD from higher baseline pain. Similar to the results of Conti et al, this study also found those treated surgically for PCFD did not experience a significant improvement in their postoperative Depression scores. These findings, in conjunction with the previous studies, suggest that surgical treatment for PCFD may lead to significant improvement in multiple PROs, but may not significantly improve PROs related to Depression. This is likely due to the fact that depression is multifactorial and not necessarily dependent on surgical treatment for PCFD.19,27,31
Although the effect of surgical management on the improvement of PROs for PCFD has been previously investigated, it has not been determined if such an effect is significantly different than that which is observed in patients undergoing surgical treatment of other chronic, degenerative foot and ankle conditions such as ankle instability or hindfoot arthritis.5,6,24 This study found that those with PCFD had higher baseline Pain Intensity scores (more reported pain) but demonstrated a greater degree of improvement in postoperative Pain Intensity scores at 3, 6, and 12 months compared to those with ankle instability/hindfoot arthritis. Such a trend was not observed in other PROs. This suggests that surgical treatment for PCFD may have a greater impact on patient-reported Pain Intensity compared with surgical treatment for ankle instability/hindfoot arthritis. This may represent the respective differences regarding the impact of each condition on overall foot function and gait, but more research is needed to evaluate such differences and improve treatment options, accordingly.
In addition, a notable finding was the decrease in Pain Intensity observed from baseline to 3 months postoperatively for both the flatfoot and the ankle instability/hindfoot arthritis group. The decrease was larger for the flatfoot group. We hypothesize that this is due to the combination of both bony and soft tissue procedures that occur with a flatfoot reconstruction. Additionally, because of the transfer of the flexor digitorum longus tendon, which has less strength than the posterior tibial tendon, we hypothesize that patients would have not been able to adequately hypertrophy that muscle tendon unit yet and accordingly not be able to perform as well physically in the initial post-operative period.
Satisfaction scores following surgical intervention for PCFD have been found to be generally positive. Saraiva et al 26 found that 93.3% of patients were satisfied following posterior tibial tendon tendoscopy and medializing calcaneal osteotomy, Smith et al 29 found 69% of patients were satisfied following isolated gastrocnemius resection, Kim et al 18 found 88.5% of patients were satisfied following spring ligament reconstruction, and Traynor et al 30 found a postoperative patient satisfaction score of 82.5 following isolated talonavicular arthrodesis. Despite these positive findings, no studies have directly compared postoperative satisfaction scores of patients undergoing surgical treatment for PCFD compared with those undergoing surgical treatment for ankle instability or hindfoot arthritis. The current study found no significant difference in the overall satisfaction rates between patients undergoing surgical treatment for PCFD or ankle instability/hindfoot arthritis. However, the odds of satisfaction were lower at 12 months compared with 6 months postoperative in PCFD patients. These results suggest that although those with PCFD or ankle instability/hindfoot arthritis have similar rates of satisfaction shortly after surgical intervention, the odds of satisfaction rates may decrease over time. It is also possible that 6 months is too early to accurately measure patient satisfaction, because all of these surgeries have long recovery periods, with patients often nonweightbearing for at least 6-10 weeks and in progressive weightbearing protocols through a boot and/or brace until 12-16 weeks. Therefore, 12 months may be a more suitable time to assess outcomes like patient satisfaction.4,5,9 Future studies should seek to evaluate longer-term postoperative satisfaction scores among PCFD patients and compare survivorship of such interventions in order to determine the most effective treatment for this condition, as well as the most appropriate timing to assess surgical satisfaction.
There are several limitations to this study. First, the study uses the OFAR database, a foot and ankle–specific database.14,15 This study is inherently dependent on the quality of the data, and the radiographs for a specific patient cannot be reviewed. Second, this database encompasses patients from across the country. This makes the data more generalizable; however, a specific surgeon’s technique for the surgery cannot be analyzed or controlled for. In addition, patients were excluded if they did not have follow-up PROs at all visits and only 70% of patients had associated satisfaction scores. Also, subgroup analyses with different surgical techniques and/or by flatfoot staging was not possible because of small numbers. Finally, this study only examined outcomes in patients at 1 year postoperatively so that longer-term satisfaction and changes in PROs cannot be analyzed; however, the OFAR database is specifically for assessing short- and midterm outcomes following common foot and ankle procedures.
Conclusion
PCFD represents a challenging condition for foot and ankle surgeons given the complexity of its pathophysiology and numerous treatments therein. However, this study found that patients who underwent surgical management of PCFD demonstrated significant improvements in their PROs and postoperative satisfaction. Additionally, compared with patients who underwent surgical management of ankle instability or hindfoot arthritis, PCFD patients demonstrated greater improvement in Pain Intensity, whereas other PROMIS domains improved similarly between groups, with no overall difference in satisfaction between groups at 12 months. Future studies should further evaluate the relative effects of surgical options of PCFD in a larger sample to allow for comparisons between surgical techniques as well as flatfoot severity, given that operative intervention has been shown to improve PROs for this condition, specifically related to pain.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251393649 – Supplemental material for A Retrospective Comparative Analysis of Demographics and Patient-Reported Outcomes in Patients With Progressive Collapsing Foot Deformity and Ankle Instability or Hindfoot Arthritis
Supplemental material, sj-pdf-1-fao-10.1177_24730114251393649 for A Retrospective Comparative Analysis of Demographics and Patient-Reported Outcomes in Patients With Progressive Collapsing Foot Deformity and Ankle Instability or Hindfoot Arthritis by Heidi C. Ventresca, Jack M. Ayres, Chase Gauthier, Patrick Carry, William Kelly, Harley T. Davis, Tyler A. Gonzalez and J. Benjamin Jackson in Foot & Ankle Orthopaedics
Footnotes
Appendix
Summary of Staging Within the Flatfoot Group.

| n | % | |
|---|---|---|
| Flatfoot stage | ||
| Stage I: No hindfoot valgus, PTT intact | 5 | 21.7 |
| Stage II-A-1: Flexible hindfoot valgus with minimal/reducible forefoot supination | 3 | 13.0 |
| Stage II-A-2: Flexible hindfoot valgus with fixed forefoot supination | 1 | 4.3 |
| Stage II-B: Flexible hindfoot valgus with forefoot abduction | 7 | 30.4 |
| Stage III: Rigid hindfoot valgus | 1 | 4.3 |
| Stage IV: Ankle valgus with talar tilt | 1 | 4.3 |
| Not applicable | 5 | 21.7 |
ORCID iDs
Ethical Considerations
Ethical approval was obtained from the authors’ Institutional Review Board.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Patrick Carry, PhD, reports disclosures relevant to manuscript of paid consultant for American Orthopaedic Foot & Ankle Society. Tyler A. Gonzalez, MD, MBA, reports disclosures relevant to manuscript of Stryker, consultant; Exatech, consultant; Enovis, consultant, royalties; Treace, consultant, royalties; Vilex, consultant, royalties (no funding is specific to this manuscript)]. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.