
Abstract
Background:
The optimal surgical procedures for chronic Lisfranc injuries are controversial. This study aimed to demonstrate the clinical outcomes of fiber tape fixation for chronic Lisfranc injuries under early full weightbearing protocols.
Methods:
This study included 11 feet from 10 patients who underwent fiber tape fixation for chronic Lisfranc injuries (undiagnosed for more than 6 weeks from injuries). All patients were allowed full weightbearing with normal shoes 4 weeks after the surgery. Clinical outcomes were evaluated with the Self-Administered Foot Evaluation Questionnaire. Radiographic outcomes were evaluated with a first cuneiform (C1)-second metatarsal (M2) distance from weightbearing anteroposterior plain foot radiography.
Results:
The median follow-up period was 12 months (IQR, 12-16). The median C1-M2 distance improved significantly from 3.3 mm (IQR, 2.9-5.2) to 1.6 mm (IQR, 1.5-2.2). The pain, physical functioning, social functioning, shoe-related, and general health subscales of SAFE-Q improved significantly after the surgery, whereas the sports subscale did not reach statistical significance (P = .063). Five patients, who regularly participated in sports activities, were able to return to their preinjury sport level by 12 months. There were no complications, such as infection, nerve or tendon injuries, or hardware-related discomfort, in the entire cohort.
Conclusion:
The fiber tape fixation device under early full weightbearing protocols led to short-term improvements in pain, function, and radiographic stability for chronic Lisfranc injuries, with no observed complications.
Level of Evidence:
Level IV, case series.

Introduction
Lisfranc joint injuries may present in several forms, ranging from subtle ligament damage to clear dislocations. Diagnosing subtle Lisfranc injuries remains challenging, and approximately 20% of cases are missed or diagnosed late, 1 potentially contributing to chronic midfoot instability, degenerative changes in the joints, and overall physical impairment. 2
Historically, tarsometatarsal (TMT) arthrodesis is considered the standard intervention in patients with chronic Lisfranc injuries. 3 However, it compromises joint mobility. Consequently, open reduction and internal fixation (ORIF) or ligamentous reconstruction with tendon grafts are being considered for chronic cases without secondary degenerative changes.1 -4
Recently, there has been growing interest regarding the use of flexible fixation devices for ligamentous Lisfranc injuries owing to their ability to prevent hardware breakage, and the need for its removal. 5 Although the available clinical data on suture button fixation for chronic Lisfranc injuries have shown promising results,2,3 there is a lack of relevant clinical data on fixation with a ligament reinforcement technique using a fiber tape. 5 As previous biomechanical studies have shown that this fiber tape fixation can provide superior stability to suture button fixation, 6 we hypothesized that the fiber tape fixation could achieve favorable outcomes under early full weightbearing (WB) in chronic Lisfranc injuries. The present study aimed to assess the clinical and radiographic outcomes of the fiber tape fixation for chronic Lisfranc injuries under early full WB protocols.
Methods
Study Population and Design
In this study, we reviewed the data for 13 feet from 11 patients who underwent InternalBrace (Arthrex, Naples, FL) fixation for chronic Lisfranc injuries between 2020 and 2024. Each patient underwent WB foot radiography, non-WB computed tomography, and ultrasonography. 7 For comparison, contralateral WB foot radiographs were obtained. The following criteria were used to diagnose an unstable subtle Lisfranc injury: (1) well-documented history of trauma; (2) a first cuneiform (C1)–second metatarsal (M2) distance greater than 2 mm observed on WB anteroposterior foot radiographs 7 ; and (3) the absence of definitive dislocation or osteoarthritic changes in a Lisfranc joint. 5 Subtle Lisfranc injuries were defined as chronic if they had occurred more than 6 weeks ago. 3 Patients with a prior foot surgery (1 foot) and those with a short follow-up period of less than 1 year (1 foot) were excluded from the study. Ultimately, 11 feet from 10 patients were included in the analysis.
Surgical Procedures
A 2-cm dorsal incision was made across the C1-M2 region and along the lateral edge of M2, whereas another 2-cm incision was performed medially at the inferior border of C1 (Figure 1A); scar tissue in the C1-M2 region was then excised. Next, adequate reduction was achieved with a large-size bone clamp placed between the base of M2 and the C1. A 1.2-mm K-wire was positioned from the base of M2 into the C1 in a medial and plantar direction (Figure 1B). A 2.7-mm cannulated drill was used to make a bone tunnel (Figure 1C), followed by the placement of a 3.4-mm cannulated drill from medial to lateral through C1 (Figure 1D). A 2-mm FiberTape (Arthrex) construct with a threaded elongated button was passed over a 1.6-mm guidewire from lateral to medial through the preformed tunnel (Figure 1E), and a 4.75-mm polyetheretherketone (PEEK) interference screw (Arthrex) was positioned into C1 between the two suture limbs with the same tension (Figure 1F). 5 Finally, the stability of the Lisfranc joint was confirmed under fluoroscopy with M2 valgus stress test, where no evidence of widening was present (Figure 1G).

(A) A 2-cm dorsal incision was made across the first cuneiform (C1)–second metatarsal (M2) region and along the lateral edge of M2, while another 2-cm incision was made medially at the inferior border of C1. (B) A large bone clamp was positioned between the base of M2 and C1 via the 2 incisions to attain reduction, and a 1.2-mm K-wire was placed from the base of M2 into C1 in a medial and plantar direction. (C) A 2.7-mm cannulated drill guided by a wire was used to create a bone tunnel, followed by (D) the placement of a 3.4-mm cannulated drill in a mediolateral direction through C1. (E) A 2-mm FiberTape construct with a threaded elongated button was passed over a 1.6-mm guidewire laterally to medially through the preformed tunnel. (F) A 4.75-mm polyetheretherketone (PEEK) interference screw was positioned into the C1 between 2 suture limbs with the same tension. (G) Finally, the stability of the Lisfranc joint was ensured with fluoroscopy.
Full WB on heel in a stiff-soled shoe was permitted from the first postoperative day; full WB with normal shoes was permitted 4 weeks after surgery.
Outcomes
The Self-Administered Foot Evaluation Questionnaire (SAFE-Q) 8 was used to assess clinical outcomes before the surgery and at the last visit.
Standard anteroposterior WB radiographs of the injured feet were obtained preoperatively and at the last visit; the distance between C1 and M2 was outlined as the C1-M2 distance. 7
Statistical Analysis
Statistical analysis was performed using JMP 17.0 (SAS Institute, Cary, NC). The differences between preoperative and postoperative (at the last visit) clinical outcomes and radiographic parameters were evaluated using the Wilcoxon signed-rank test.
Results
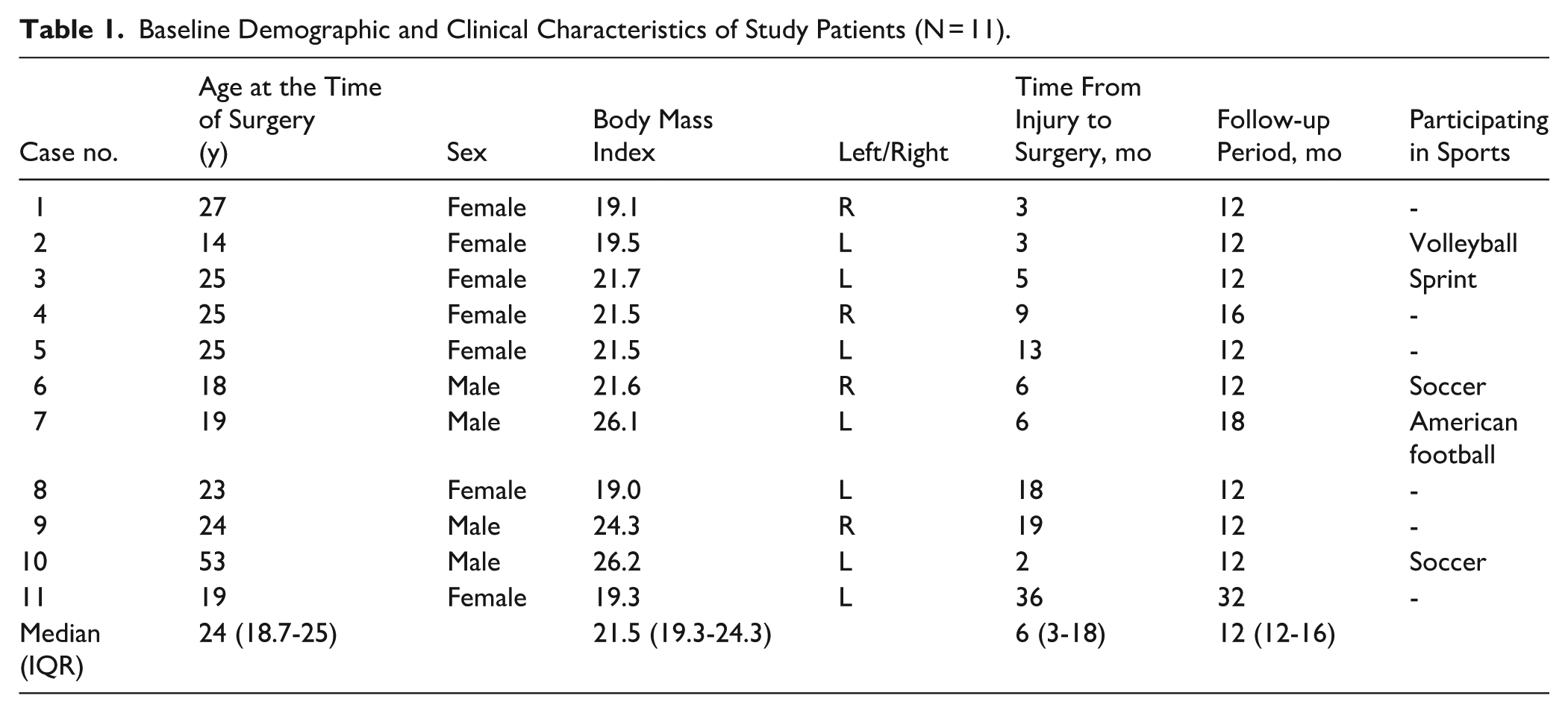
There were 7 female and 4 male patients in the study cohort (median body mass index = 21.5, IQR 19.3-24.3). The median age at the time of surgery was 24 years (IQR, 18.7-25). The median time from injury to surgery was 6 months (IQR, 3-18), and the median follow-up period was 12 months (IQR, 12-16) (Table 1).
Baseline Demographic and Clinical Characteristics of Study Patients (N = 11).
Postoperatively, the median C1-M2 distance improved significantly from 3.3 mm (IQR, 2.9-5.2) to 1.6 mm (IQR, 1.5-2.2) (Figure 2). Moreover, the scores in the pain, physical functioning, social functioning, shoe related, and general health subscales of SAFE-Q improved significantly after the surgery. Five patients, who regularly participated in sports activities, were able to fully return to sports; their scores in the sports subscale of SAFE-Q also improved after surgery (Table 2). There were no complications, such as infection, nerve or tendon injuries, or hardware-related discomfort, in the entire cohort.
Clinical and Radiographic Outcomes of Study Patients (N = 11).
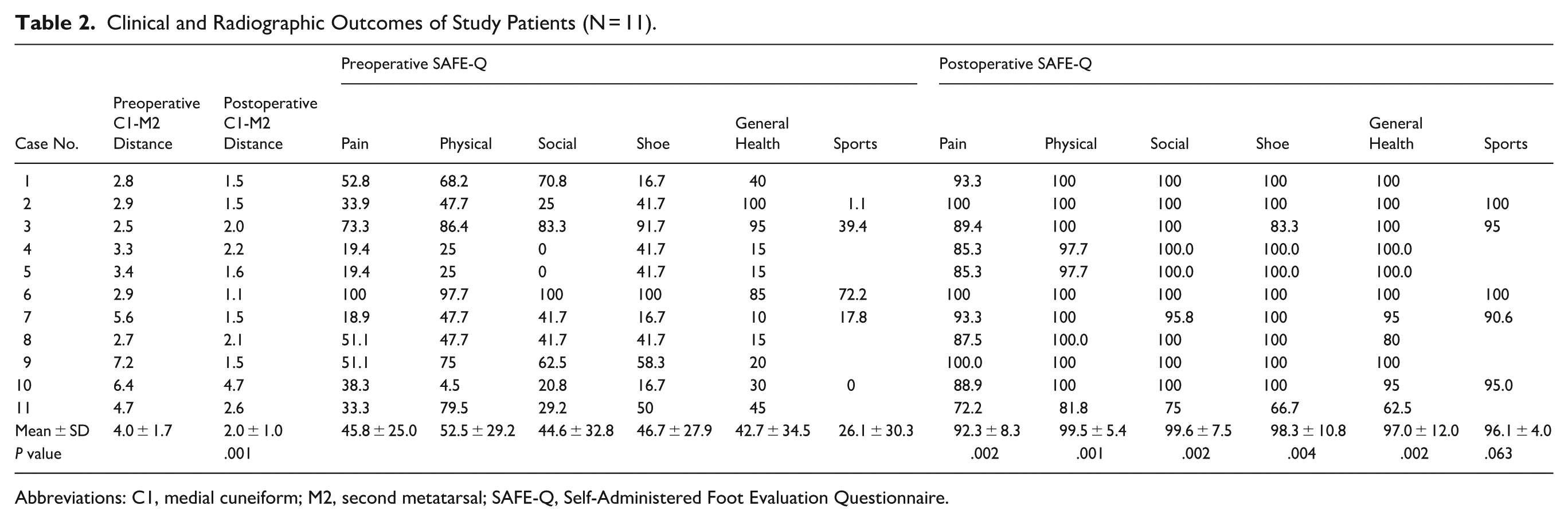
Abbreviations: C1, medial cuneiform; M2, second metatarsal; SAFE-Q, Self-Administered Foot Evaluation Questionnaire.

(A) Preoperative weightbearing radiographs from Case 2. (B) Postoperative weightbearing radiographs. On the anteroposterior view, the C1-M2 distance improved from 2.9 mm preoperatively to 1.5 mm postoperatively.
Discussion
This retrospective preliminary study revealed short-term improvements in radiographic alignment (C1-M2) and patient-reported outcomes with fiber-tape fixation for chronic Lisfranc injuries, with no complications observed during the 12-month follow-up, even with early full WB.
In the biomechanical study, although screw fixation demonstrates excessive stiffness, which could prevent normal joint motion, fiber tape fixation exhibits stiffness comparable to the anatomical Lisfranc joint and superior to that achieved with suture button fixation. 6 Another study revealed that the fiber tape fixation had comparable biomechanical stability to screws. 9 Therefore, the fiber tape fixation can provide better stability than suture button does while maintaining satisfactory joint flexibility.5,6 To date, only a single case series has documented the use of the fiber tape fixation for acute Lisfranc injuries and demonstrated promising short-term results. 10 The present study further corroborates the use of the fiber tape fixation for chronic Lisfranc injuries in the form of good clinical and radiologic outcomes.
There are several studies reporting the use of different surgical procedures for chronic Lisfranc injuries. Some studies have reported good clinical outcomes with ORIF with screws or plates in achieving full WB at 6-8 weeks postoperatively.1,2 Ligament reconstruction with tendon autografts has also exhibited satisfactory results, allowing full WB at 8-12 weeks. 4 Likewise, suture button fixation also allowed for full WB at 8 weeks. 2 In this regard, the most important finding of the study is that the fiber tape fixation can improve clinical and radiographic outcomes under earlier full WB even at 4 weeks.
A major concern about the present study was the lack of C1-C2 (second cuneiform) fixation. Previous biomechanical investigations showed that the fiber tape fixation involving both C1-M2 and C1-C2 achieves stability comparable to screw fixation, 9 whereas the construct involving only C1-M2 fixation showed lesser stability than screws. 6 However, the present results suggest that the fiber tape fixation for C1-M2 alone provides favorable clinical results. As no comparative study has yet been conducted, further research performing the direct analysis of the 2 fixation techniques—C1-M2 alone vs C1-M2 plus C1-C2—is warranted.
This study had several limitations. First, this is a retrospective study with a relatively short follow-up duration and small sample size. Notably, a follow-up duration limited to 1 year is inadequate to evaluate the requirement for hardware removal and the potential development of arthritis. Thus, a long-term study with a larger sample size study comparing the efficacy of other surgical procedures is needed to provide stronger evidence. Second, the fiber tape fixation device used in this study is different from the original one 5 because this product is not commercially available in Japan. To address this concern and ensure consistency, we applied the same procedure with the same anchors and tape as in the original technique. Third, this study did not include the patients with high BMI. Therefore, our results may not be generalizable for this category.
Conclusion
The fiber tape fixation was associated with short-term improvements in radiographic alignment and patient-reported outcomes, with no complications observed during 12-month follow-up in this small case series. Early full weightbearing at 4 weeks was feasible in this cohort; however, sports subscale improvement did not reach statistical significance. Further prospective, comparative studies with longer follow-up are necessary before recommending this technique as a standard treatment for chronic subtle Lisfranc injuries.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251388428 – Supplemental material for Clinical Outcomes of Fiber-Tape Flexible Fixation for Chronic Lisfranc Injuries
Supplemental material, sj-pdf-1-fao-10.1177_24730114251388428 for Clinical Outcomes of Fiber-Tape Flexible Fixation for Chronic Lisfranc Injuries by Kensei Yoshimoto, Mitsuki Kumaki, Takumi Koseki, Masahiko Noguchi, Ayako Tominaga and Ken Okazaki in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
The responsible institutional review board approved this study (IRB number: 148).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Informed Consent
Informed consent was obtained from all patients.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.