
Abstract
Background:
Modified oblique Keller capsular interposition arthroplasty (MOKCIA) is a treatment for hallux rigidus that has been shown to have similar long-term outcomes compared with metatarsophalangeal (MTP) arthrodesis. The purpose of this study was to evaluate differences in the level of sport and other activity following MOKCIA or first MTP arthrodesis.
Methods:
From 2005 to 2020, 58 MOKCIA and 112 arthrodesis patients were identified. Patients completed a sports-specific questionnaire (SSQ) along with the visual analog scale (VAS) pain/satisfaction, Foot and Ankle Ability Measure (FAAM), and Patient-Reported Outcomes Measurement Information System (PROMIS) instruments, which yielded 14 MOKCIA and 15 arthrodesis subjects.
Results:
At an average 13 years’ follow-up, the MOKCIA group participated in a mean of 3.4 ± 1.7 sport activities preoperatively and 3.4 ± 1.9 postoperatively, whereas arthrodesis patients participated in 3.5 ± 1.7 activities preoperatively and 2.9 ± 1.4 postoperatively (P = .22). Compared with preoperative, the MOKCIA group rated sporting activities as less difficult (10/12) and same difficulty (2/12). Hundred percent of patients in the MOKCIA group were satisfied with their overall level of activity following surgery, whereas 87% patients (13/15) in the arthrodesis group were satisfied. Patients in the MOKCIA group were able to participate in similar numbers of activities postoperatively, but arthrodesis patients had decreased activities. PROMIS, VAS pain/satisfaction, and FAAM Sports scores were similar between the groups.
Conclusion:
We found that MOKCIA compared similarly with MTP arthrodesis in sports physical function at long-term follow-up. These results must be interpreted in light of the very low follow-up and retrospective recall of preoperative activities.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
Hallux rigidus is the most common arthritic disorder of the foot and can affect up to 2.5% to 7.8% of patients >50 years of age. 7 The prevalence of symptomatic hallux rigidus increases with age, and the symptoms affect sports participation in those older patients because of pain and reduced function. Nonoperative treatment options for early-stage hallux rigidus can help reduce pain and improve function, but these are not always a definitive solution. 4 Cheilectomy has shown improved outcomes in restoring function and reducing pain, leading to improved sports participation with 95% pain relief in early stage (Coughlin-Shurnas grade 1 or 2) hallux rigidus; however, this procedure is not as effective in grade 3 and 4 disease. 11
For advanced hallux rigidus (Coughlin-Shurnas grade 3 and 4), first metatarsophalangeal (MTP) joint arthrodesis has been considered the standard option to alleviate pain with recent literature supporting its efficacy even in patients under 50 years old. 13 MTP arthrodesis enables some level of physical activity, and patients are often able to adapt to lower-impact activities, such as swimming or cycling. However, high-impact sports are often still limited postsurgery. 12
Motion-sparing arthroplasty procedures using silicone polymers, metal, polyvinyl alcohol hydrogel, and biologic materials have been used by various authors. Because of the lack of reproducible long-term results, implant failures, and soft tissue complications, many MTP arthroplasty options have been associated with poor or less-predictable clinical outcomes. 6 Modified oblique Keller interposition arthroplasty (MOKCIA) is a motion-sparing procedure with improved outcomes maintained up to 15 years postsurgery. 8 In patients desiring retained MTP motion, and high level of function, MOKCIA is a potential option for more advanced arthritis where cheilectomy alone may not be sufficient, including patients with more advanced grade 3 or 4 hallux rigidus. The aim of this study was to examine the patient’s ability to return to sport and activity following MOKCIA in comparison to MTP arthrodesis for advanced-stage hallux rigidus. We hypothesized that MOKCIA patients would have similar or improved return to activities and sports postoperatively in comparison to MTP arthrodesis.
Methods
Following institutional review board (IRB) approval, a retrospective review was performed for patients aged 18-60 years old who underwent MOKCIA or first MTP arthrodesis for advanced hallux rigidus. From 2005 to 2020, there were 58 MOKCIA and 112 arthrodesis patients who were identified from the medical record using respective CPT codes. Study participants were recruited according to the recruiting flowchart (Appendix 1) with up to 3 attempts to contact the patient by phone, followed by 1 mailing for all subjects who had accurate contact information, which yielded 14 MOKCIA and 15 arthrodesis subjects for the full study. All data collection and subject testing occurred between September 2023 and March 2024. Inclusion criteria included age between 18 and 60 years at the time of surgery. Exclusion criteria included neuropathy at the time of surgery, neurologic disorders affecting gait at the time of surgery or currently (eg, Parkinson, stroke with motor deficits, cerebral palsy, myelopathy), patients with current dementia that would affect patient-reported outcome measures, and patients who underwent a MOKCIA or arthrodesis for any diagnosis other than hallux rigidus. The decision for which procedure was performed was made preoperatively based on a diagnosis of hallux rigidus rated as grade 3 or 4 and surgeon-patient preference based on a preoperative discussion of the risks, goals, and expectations for each procedure. The MOKCIA procedure was offered for patients with at least a 30-degree arc of metatarsophalangeal motion and no significant angular deformity or prior surgery. The MOKCIA and arthrodesis procedures were performed by fellowship-trained surgeons.
The MOKCIA procedure was performed as initially described by Mroczek and Miller, modified from Hamilton technique, consisting of a dorsal cheilectomy, oblique resection of the phalanx base, and interposition of either autogenous dorsal capsule (n = 11) or human acellular dermal allograft (n = 3) (see Figure 1).2,8 -10 Dermal allograft was used when the host dorsal capsule was inadequate for interposition. For the MTP arthrodesis group, a standard MTP approach and fixation technique was used as previously described. Intraoperative photographs illustrating the MOKCIA technique have been previously reported. 8
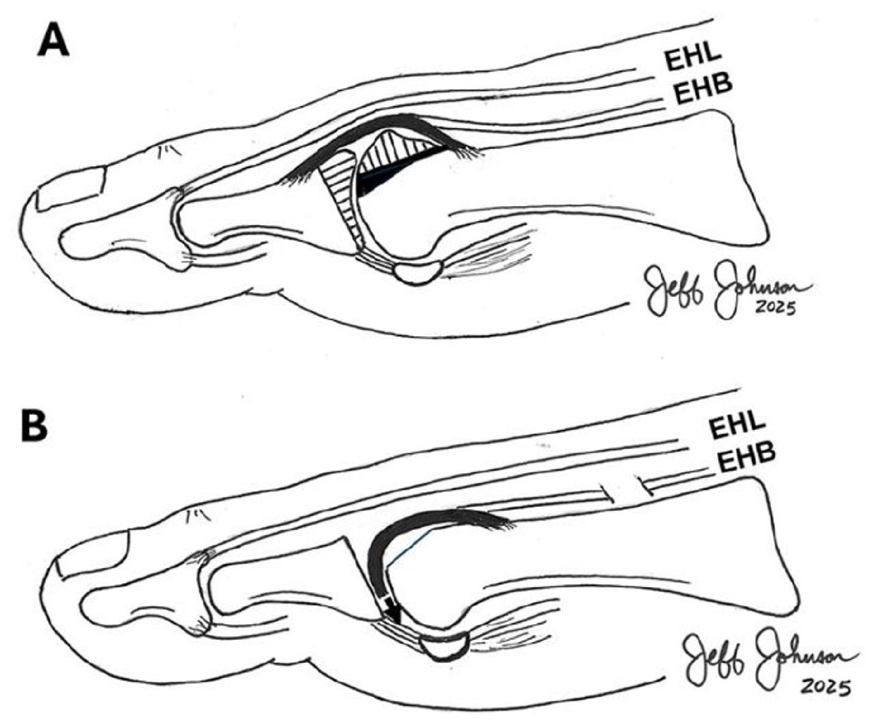
(A) A dorsal cheilectomy and an oblique resection of the articular surface of the base of the proximal phalanx. (B) Insertion of the capsular interposition graft. Image from Johnson et al.8
Outcome Measures
Primary outcome measures
Patients were then contacted and asked to complete a physical activity and sports-specific questionnaire (SSQ). The SSQ queries the patients on their participation in any of 15 common sports and physical activities preoperatively and postoperatively. These included a mixture of low-, medium-, and high-impact activities. Participant was allowed to report activities not listed in the query. Visual analog scale satisfaction and pain scores were obtained from each participant (0 = extremely unsatisfied/no pain, 10 = extremely satisfied/worst possible pain).
Secondary outcome measures
Clinical outcome measures using the Foot and Ankle Ability Measure and Patient-Reported Outcomes Measurement Information System physical function, pain interference, anxiety, and depression scores were also obtained from each patient to determine their current clinical status.
Two-sample t tests, χ2, or Mann-Whitney U tests were used to compare groups, with the significance level set at .05. The significance level was not adjusted because our analyses were exploratory. We did have missing data in the reports; the patient report of difficulty with activity postoperatively was missing in 2 of the MOKCIA patients, which is reported as the percentage per group.
Results
There were no differences in the demographic data between the 2 groups (Table 1).
Participant Demographics and Clinical Outcomes in MOKCIA and MTP Arthrodesis Group.

Abbreviations: FAAM, Foot and Ankle Ability Measure; MOKCIA, Modified oblique Keller capsular interposition arthroplasty; MTP, metatarsophalangeal; PROMIS, Patient-Reported Outcomes Measurement Information System; VAS, visual analog scale.
Significance levels are not adjusted in this report because they are exploratory analyses. There were no missing data (question without a response).
Primary Outcomes
No significant differences were found between groups in VAS satisfaction and pain (Table 1) and did not exceed the minimal clinically important difference. All patients in the MOKCIA group were either satisfied (14%, 2/14) or very satisfied (86%, 12/14) in their activity level following surgery. Two (13%) patients in the arthrodesis group were dissatisfied with their activity and the remaining were satisfied (30%, 3/15) or very satisfied (67%, 10/15). MOKCIA group patients participated in a mean of 3.4 ± 1.7 sport activities preoperatively and 3.4 ± 1.9 postoperatively (P > .99), whereas arthrodesis patients participated in 3.5 ± 1.7 activities preoperatively and 2.9 ± 1.4 postoperatively (P = .22). Compared with preoperative, patients in the MOKCIA group (n = 12 reported) rated sporting activities as of less difficulty (83%, 10/12) and same difficulty (17%, 2/12). One arthrodesis patient reported more difficulty (7%), 10 of 15 patients less difficulty (67%), and 4 of 15 same difficulty (27%). MOKCIA patients were able to participate in similar level of activities postoperatively whereas arthrodesis patients had decreased activities (Table 2). All patients in the MOKCIA group would recommend the procedure to a friend or family whereas 2 patients in the MTP arthrodesis group would not recommend the procedure.
Preoperative and Postoperative Sports and Physical Activities by MOKCIA and Arthrodesis Group. a

Abbreviation: MOKCIA, Modified oblique Keller capsular interposition arthroplasty.
There were no missing data (question without a response) in the reported data above. Yoga and Hiking were participant-listed common activities. Hockey and Lacrosse that were in the query are not listed in the table as no subjects participated in those activities pre- and postsurgery.
Order based on preoperative to postoperative change in MOKCIA group.
Positive values: increased postoperative. Negative values: decreased postoperative.
Secondary Outcomes
No significant differences were found between groups using the Foot and Ankle Ability Measure and Patient-Reported Outcomes Measurement Information System scores (Table 1) and did not exceed the minimal clinically important difference.
Discussion
According to these data, MOKCIA patients were able to return to a similar level of function and sporting activities (total 47 activities pre- and postsurgery) but the nonrandom, indication-driven treatment selection (≥30 degrees preoperative range of motion for MOKCIA) limits causal comparisons. MTP arthrodesis patients reduced 18% of total level of participation in sports activities followed by the surgery (total 53 activities presurgery and 43 activities postsurgery). Brodsky et al 3 found that after MTP arthrodesis, patients were able to return to hiking (92%), golfing (80%), and jogging/tennis (75%) which is similar to our current findings with MOKCIA outcomes. Da Cunha et al 5 evaluated return to sports and physical activities following MTP arthrodesis in young (mean 49.7 years old) patients and found similar results including maximal level of participation in 88.6% of physical activities and 96% satisfaction regarding return to sports and physical activities. Similar to our findings, they also found that some patients (21.4%) undergoing MTP arthrodesis noted increased difficulty with activities postoperatively. In this current study, MOKCIA patients all reported the same or less difficulty with activities postoperatively. A previous long-term study with 5-year follow-up noted a failure rate of 3.8% (5/133 patients) and 4.5% (6/133 patients) rate of cock-up toe deformity with interpositional arthroplasty. 1 There were no failures and no cock-up toe deformities in this study. A radiographic analysis was not performed in this study, but a recent long-term study of MOKCIA by our group reported similar radiographic measures to arthrodesis except for a lower proximal phalanx angle following MOKCIA. 8
The small, nonrandomized, sample very low follow-up/response (<20% of eligible), and retrospective recall of preoperative activity could all introduce bias to the conclusions. In addition, patients desiring a motion-sparing procedure may have sought out our institution, which thus introduced some selection bias. Given the lengthy period from date of surgery, there may also be inherent recall bias present. However, MOKCIA is not a commonly performed procedure and this 13-year outcome data focused on sports activity is reported previously.
Conclusion
At an average of 13 years of follow-up, in this limited study, MOKCIA patients had similar clinical outcome and pain scores and were able to participate in a similar number of sporting activities postoperatively compared with MTP arthrodesis patients. Most patients in both groups found participation in sporting activities less difficult than preoperative; however, more MOKCIA patients maintained their level of sport participation postoperatively than did arthrodesis patients. MOKCIA compares favorably with MTP arthrodesis in sports physical function at long-term follow-up and is a reasonable alternative to arthrodesis for patients who wish to maintain their prior sporting activity level following surgery for advanced hallux rigidus and preserve MTP motion.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251386022 – Supplemental material for Long-term Return to Sports After Modified Oblique Keller Capsular Interposition Arthroplasty vs Arthrodesis for Advanced Hallux Rigidus: A Retrospective Cohort
Supplemental material, sj-pdf-1-fao-10.1177_24730114251386022 for Long-term Return to Sports After Modified Oblique Keller Capsular Interposition Arthroplasty vs Arthrodesis for Advanced Hallux Rigidus: A Retrospective Cohort by Andrew P. Thome, Jonathon D. Backus, Hyo-Jung Jeong, Jeremy J. McCormick and Jeffrey E. Johnson in Foot & Ankle Orthopaedics
Footnotes
Appendix
Ethical Considerations
Ethical approval for this study was obtained from the Washington University Institutional Review Board (ID: 202103252).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jonathon D. Backus, MD, reports general disclosures of being on the scientific advisory board and stock options in Sparta Medical; is a consultant for and receives royalties from Medline UNITE. Jeremy J. McCormick, MD, reports general disclosures of consulting fees and royalties from Stryker, Inc (none relevant to this manuscript). Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.