
Abstract
Background:
Trimalleolar ankle fractures pose a challenge for surgical management, especially in high-risk populations such as the elderly and patients with comorbidities. Surgeons traditionally employ open reduction internal fixation (ORIF) to manage these injuries; however, some recent studies advocate for tibiotalocalcaneal arthrodesis (TTCA) as an alternative that minimizes soft tissue disruption and facilitates earlier weightbearing. This study compares complication and readmission rates associated with ORIF and TTCA in managing trimalleolar fractures, providing insight on complication risks throughout this patient population.
Methods:
A retrospective analysis was performed using the 2016-2021 Nationwide Readmissions Database. Adult patients (≥18 years) diagnosed with trimalleolar ankle fractures who underwent either ORIF or TTCA were identified. To balance the cohorts, propensity score matching based on key comorbidities (defined as diabetes, hypertension, chronic kidney disease, osteoporosis, obesity, morbid obesity, or heart failure), age, and sex was performed. Primary outcomes included 30- and 90-day readmissions and complication rates; secondary outcomes were specific complications, including infection, nonunion, and malunion, assessed only in patients with ≥90 days’ follow-up.
Results:
A total of 602 patients were analyzed after propensity score matching (307 ORIF, 295 TTCA). TTCA patients experienced significantly higher overall complication rates compared to ORIF patients (35% [95% CI: 30.67%-41.56%] vs 13% [95% CI: 9.15%-16.53%], P < .001). Specifically, TTCA was associated with increased nonunion (10% [95% CI: 8.37%-15.67%] vs 2% [95% CI: 1.11%-4.63%], P < .001) and malunion rates (13% [95% CI: 9.53%-17.19%] vs 1% [95% CI: 0.06%-1.82%], P < .001). TTCA patients also demonstrated higher 30-day readmission rates (25% [95% CI: 21.42%-31.40%] vs 13% [95% CI: 10%-17.62%], P < .001) and 90-day readmission rates (20% [95% CI: 15.83%-24.94%] vs 10% [95% CI: 7.21%-13.98%], P < .001). In multivariable analysis, TTCA remained independently associated with higher complication risk (adjusted odds ratio: 4.10, 95% CI: 2.29-7.33, P < .001). Complication rate differences persisted across both high- and low-risk patient subgroups.
Conclusion:
In this national database analysis, ORIF was associated with significantly lower complication and readmission rates compared with TTCA for trimalleolar ankle fractures. Despite theoretical advantages of TTCA in high-risk populations, these findings suggest ORIF may be preferable for most patients, with TTCA reserved for carefully selected cases where conventional fixation is unlikely to succeed. Given the limitations of administrative data, prospective randomized trials with longer follow-up are needed to definitively establish optimal treatment algorithms for this challenging patient population.
Level of Evidence:
Level III, prognostic.
Introduction
Trimalleolar ankle fractures represent a significant clinical challenge, particularly in patient populations with compromised bone quality and soft tissue envelope such as the elderly, diabetes patients, and those with osteoporosis.9,10,13,19 Conventional open reduction and internal fixation (ORIF) has long been the standard treatment for these injuries; however, this approach is often associated with high complication rates in high-risk patients. 15 Factors such as poor bone quality, soft tissue compromise, and the presence of comorbidities including diabetes mellitus, peripheral neuropathy, and vascular disease can lead to wound complications, nonunion, and prolonged recovery periods when managed with traditional ORIF techniques.7,12,20
Recent advances in minimally invasive stabilization have introduced retrograde tibiotalocalcaneal (TTC) arthrodesis as a viable alternative. Several studies have demonstrated that TTC nailing can offer distinct advantages over ORIF, including decreased operative time, minimal soft tissue dissection, and the ability to allow early weightbearing. For example, Taylor et al 17 reported high union rates and low complication rates with the use of TTC nailing in fragility ankle fractures without formal joint preparation, emphasizing its potential to overcome the limitations posed by the traditional fixation methods in elderly, osteoporotic patients. Similarly, Tarkin and Fourman highlighted the utility of TTC nailing in a geriatric population with periarticular trauma, noting that its biomechanical stability and minimally invasive nature promote early mobilization and improved functional outcomes. 16 Furthermore, in the context of complicated diabetic ankle fractures—where the risks of wound complications, infection, and limb loss are markedly elevated—Ebaugh et al 5 demonstrated that primary TTC nailing can result in high limb salvage rates and acceptable complication profiles (18.5%) in the absence of formal joint preparation.
Recently, Dawar et al 4 reported the differential risk profiles of patients undergoing TTC arthrodesis (TTCA) for traumatic fractures compared with those for osteoarthritis, showing that those undergoing the procedure for traumatic indications have a significantly higher risk of 30-day readmission, 90-day readmission, revision surgery, and postoperative complication (odds ratio [OR] 3.002, P < .001). This analysis raises the question as to whether or not TTCA is suitable in the setting of traumatic fracture as compared to traditional ORIF. Furthermore, most of the work that suggest the superiority of TTCA has been underpowered, with the largest sample size comparing the 2 approaches being 296. 11 By critically comparing ORIF and TTCA, we hypothesize that TTCA will be associated with a greater rate of adverse outcomes compared with ORIF in the setting of trimalleolar ankle fractures.
Methods
Data Set
The study used deidentified, publicly available data from the NRD and was exempt from institutional review board approval. All analyses adhered to HCUP data use agreements and complied with relevant privacy regulations. A retrospective analysis of the 2016-2021 Nationwide Readmissions Database (NRD) was conducted to compare outcomes between TTC arthrodesis and ankle ORIF. The NRD, part of the Healthcare Cost and Utilization Project, represents roughly 60% of US hospitalizations. We selected 2016 as the start date to ensure consistent use of International Classification of Diseases, Tenth Revision (ICD-10) codes. Discharge weights provided by the NRD were used to generate nationally representative estimates.
Case Identification
Adult patients (≥18 years) treated for trimalleolar ankle fractures between 2016 and 2021 were identified using a combination of and International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM), diagnosis codes for trimalleolar fracture and International Classification of Diseases, Tenth Revision, Procedure Coding System (ICD-10-PCS), procedure codes for either TTCA or ORIF. Patients were divided into 2 cohorts based on the primary surgical procedure. Patients undergoing TTCA were identified by requiring both ankle (0SGF/G codes) and tarsal (0SGJ/H codes) fusion procedure codes in the same index encounter, a strategy adapted from prior NRD analyses of TTCA.3,4 Although the codes are not specific to TTCA, manufacturers of TTCA devices instruct surgeons to apply these codes when billing for the procedure. Patients receiving open reduction and internal fixation of the ankle joint were identified using a code for insertion of an internal fixation device by open approach. Specific ICD-10 codes are outlined in Supplementary Table 1. Exclusion criteria included cases with concomitant procedures that might confound outcomes (eg external fixation). To improve diagnostic specificity, nonunion and malunion complications were only analyzed in patients with at least 90 days of follow-up within the same calendar year. Patients with index surgeries occurring in Q4 were excluded from this analysis. Furthermore, we excluded readmissions that involved procedures or diagnoses pertaining to non–lower-extremity regions (eg, spine, upper limb, femur) to minimize misattribution.
Data Collection
Demographic variables (age, sex), comorbidities, and hospital characteristics were extracted from the NRD. Comorbidities were quantified using ICD codes outlined in Supplementary Table 2. Primary outcomes included overall complication rate (“Any Complication”) within 90 days, stratified complication rates outlined by ICD-10-CM codes in Supplementary Table 3, and 30-day and 90-day readmission rates. Overall complication rate was defined as the occurrence of any of the following: wound dehiscence, cellulitis, thromboembolism, nonunion, malunion, infection, or hardware failure, and the composite endpoint was used to assess the total burden of perioperative complications and to examine how high-risk status impacts complication rates across TTC and ORIF cohorts. High-risk status was defined as age ≥60 years and at least 1 of the following comorbidities: diabetes mellitus, hypertension, chronic kidney disease, osteoporosis, obesity, morbid obesity, or heart failure. Low-risk status applied to patients aged less than 60 years with none of the mentioned comorbid conditions.
Propensity Score Matching
To reduce selection bias and account for baseline differences between the TTCA and ORIF groups, propensity score matching (PSM) was employed. Matching variables included age, sex, and several comorbidities (eg, diabetes, hypertension, obesity, chronic kidney disease). The ICD-10-CM codes used to identify comorbidities is outlined in Supplementary Table 4. A 1:1 nearest neighbor matching algorithm with a caliper width of 0.1 SDs of the logit of the propensity score was used. Postmatching balance was assessed using χ2 analysis, with P values greater than .05 indicating adequate balance between groups.
Statistical Analysis
Descriptive statistics were used to summarize baseline characteristics and outcomes. Statistical significance was set at a P value <.05. Continuous variables are reported as means with SDs and were compared using Student t test. Categorical variables are expressed as frequencies with percentages and compared using χ2 or Fisher exact tests. For the primary outcomes of postoperative complications and readmissions, 95% CIs were calculated using the Wilson score method. Following PSM, we conducted multivariable logistic regression to further account for potential residual confounding. The model included age, sex, and baseline comorbidities—hypertension, diabetes mellitus, heart failure, osteoporosis, chronic kidney disease, obesity, and morbid obesity—as covariates. Adjusted odds ratios (aORs) were calculated for the composite complication outcome, as well as for 30-day and 31-to-90-day readmission rates. All analyses were performed using IBM SPSS version 29.0.
Results
Patient Factors
A total of 602 patients were included in the study, with 307 in the ORIF group and 295 in the TTCA group. The mean age was 66.99 years (SD = 12.88), with no significant difference between groups (ORIF: 66.53 vs TTCA: 67.47, P = .222). Gender distribution was nearly identical between groups (66% female in both groups, P > .99) (Table 1).
Demographics Between 2 Surgical Cohorts After Propensity Score Matching.

Abbreviations: ORIF, open reduction internal fixation; TTCA, tibiotalocalcaneal arthrodesis.
Analysis of comorbidities revealed several significant differences between groups before PSM. Prior to matching, the ORIF group demonstrated significantly higher rates of hypertension (47.1% vs 38.7%, P = .040), current nicotine dependence (15.7% vs 9.8%, P = .017), diabetes (13.9% vs 5.7%, P < .001), and fibromyalgia (3.9% vs 1.0%, P = .030) compared with the TTCA group. Conversely, the TTCA group had significantly higher rates of hypothyroidism (24.7% vs 17.9%, P = .002), heart disease (25.8% vs 12.9%, P < .001), and anticoagulant therapy use (12.9% vs 7.1%, P = .003). Although peripheral neuropathy is a well-recognized risk factor for complications following ankle fracture surgery, it was not included in our comorbidity analysis because of inconsistent or nonspecific coding in the NRD. After PSM, these differences were effectively balanced, with no statistically significant differences observed between the ORIF (n = 307) and TTCA (n = 295) groups for any comorbidity (Table 2).
Comorbidities Before and After Propensity Score Matching (PSM).
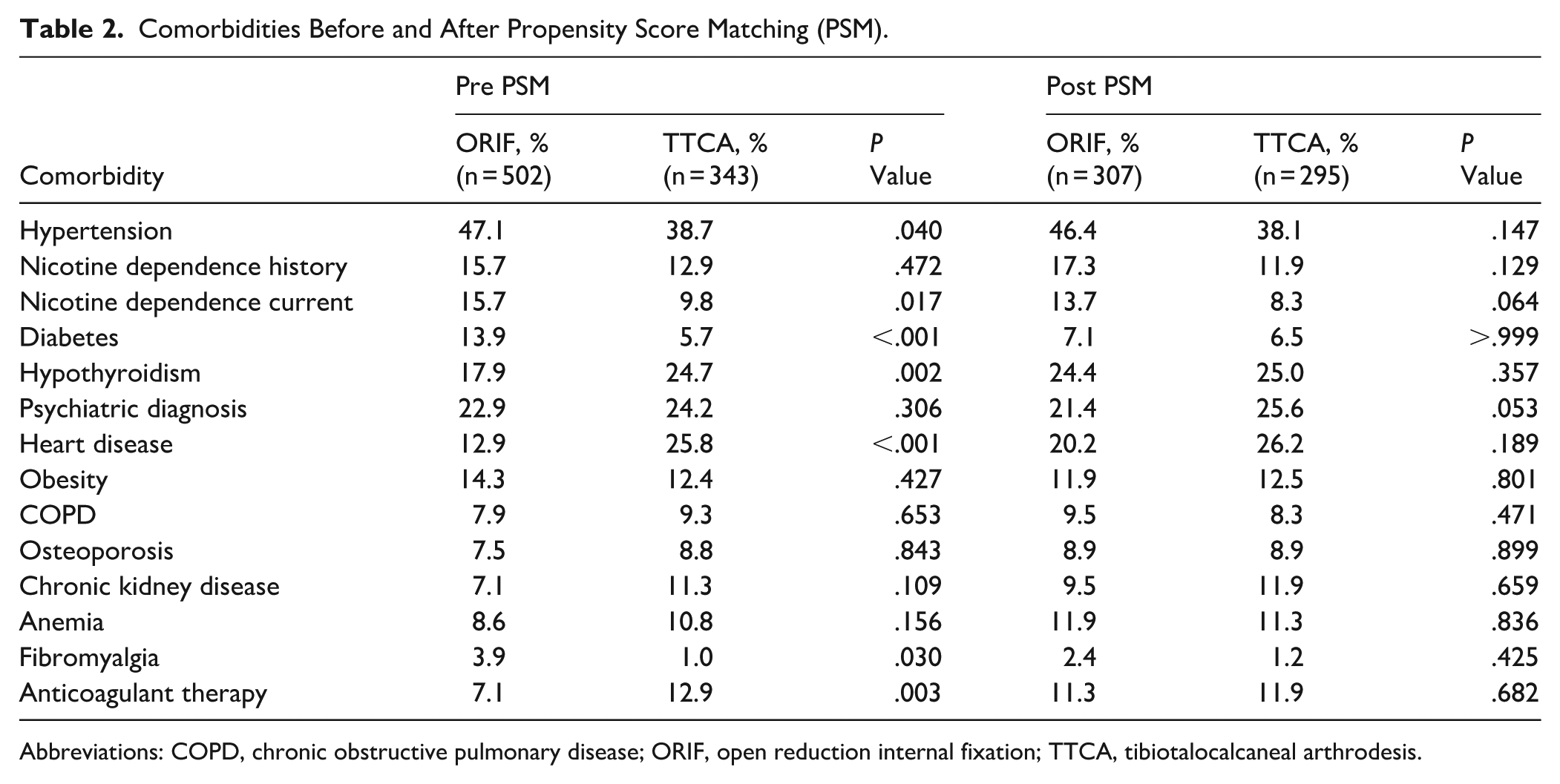
Abbreviations: COPD, chronic obstructive pulmonary disease; ORIF, open reduction internal fixation; TTCA, tibiotalocalcaneal arthrodesis.
Complication Rates Between Cohorts
Significant differences in complication rates were observed between the 2 treatment groups. The TTCA group demonstrated a substantially higher overall complication rate compared with the ORIF group (35% [95% CI: 30.67%-41.56%] vs 13% [95% CI: 9.15%-16.53%], χ² = 43.613, P < .001). Specifically, nonunion and malunion rates were significantly higher in the TTCA group. Nonunion occurred in 10% of TTCA patients (95% CI: 8.37%-15.67%) compared with only 2% of ORIF patients (95% CI: 1.11%-4.63%) (χ² = 18.230, P < .001), whereas malunion was observed in 13% of TTCA patients (95% CI: 9.53%-17.19%) vs just 1% of ORIF patients (95% CI: 0.06%-1.82%) (χ² = 37.108, P < .001). Conversely, wound dehiscence was significantly more common in the ORIF group (4% [95% CI: 2.01%-6.3%] vs 1% [95% CI: 0.19%-2.44%], χ² = 4.550, P = .033). Readmission rates were also significantly higher in the TTCA group. The 30-day readmission rate for TTCA patients was nearly double that of ORIF patients (25% [95% CI: 21.42%-31.4%] vs 13% [95% CI: 10%-17.62%], χ² = 14.927, P < .001). Similarly, 31-90-day readmissions were significantly more frequent in the TTCA group (20% [95% CI: 15.83%-24.94%] vs 10% [95% CI: 7.21%-13.98%], χ² = 11.192, P < .001) (Table 3). The overall mean length of stay was 7.62 days (SD = 8.70), with a trend toward longer stays in the TTC group that did not reach statistical significance (ORIF: 7.19 vs TTCA: 8.08 days, P = .084).
Complications and Readmission Comparative Analysis After Propensity Score Matching (PSM). a
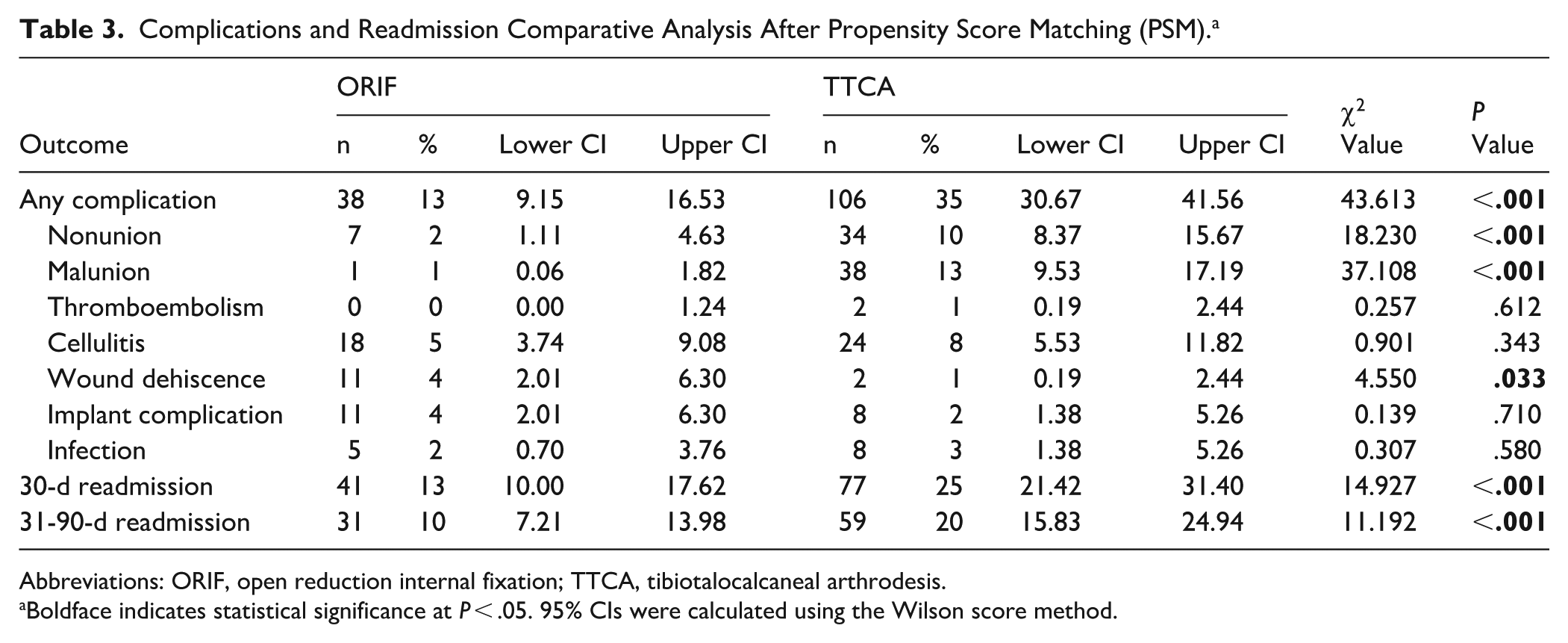
Abbreviations: ORIF, open reduction internal fixation; TTCA, tibiotalocalcaneal arthrodesis.
Boldface indicates statistical significance at P < .05. 95% CIs were calculated using the Wilson score method.
Multivariable Logistic Regression Analysis
In multivariable logistic regression performed on the matched cohort, TTCA remained significantly associated with higher odds of experiencing any complication compared to ORIF (aOR 4.10, 95% CI 2.29-7.33; P < .001). TTCA was also associated with increased odds of 30-day readmission (aOR 2.21, 95% CI 1.21-4.03; P = .010) and 31-to-90-day readmission (aOR 2.35, 95% CI 1.21-4.58; P = .012), suggesting the association persists even after controlling for demographic and comorbidity differences.
High Risk vs Low Risk
Finally, subanalysis of complication rates based on patient risk stratification revealed significant differences both between treatment modalities and across risk groups. In the high-risk patient population, TTC treatment was associated with a substantially higher complication rate (approximately 42%) compared to ORIF treatment (approximately 18%), with this difference reaching statistical significance (P < .05). Similarly, in the low-risk cohort, TTC treatment resulted in significantly higher complication rates (approximately 32%) compared with ORIF treatment (approximately 8%), also reaching statistical significance (P < .05). When comparing within treatment groups, high-risk patients experienced higher complication rates than low-risk patients for both treatment modalities. The difference was more pronounced in the ORIF group, where high-risk patients had more than double the complication rate of low-risk patients (18% vs 8%, P < .05). In the TTC group, high-risk patients also demonstrated higher complication rates compared to low-risk patients (42% vs 32%), though this difference was not statistically significant (Figure 1).

Complications rates by risk category. Dashed lines signify statistical significance between groups at P < .05. ORIF, open reduction internal fixation; TTC, tibiotalocalcaneal arthrodesis.
Discussion
Our study analyzed a large nationwide cohort of trimalleolar ankle fractures, comparing ORIF to TTCA. The findings revealed that TTCA was associated with significantly higher overall complication rates than ORIF, particularly regarding nonunion and malunion. Furthermore, TTCA patients demonstrated higher 30- and 90-day readmission rates, suggesting a greater burden of postoperative morbidity. Contrary to prior assumptions that TTCA might reduce complications in high-risk patients, our data indicate that ORIF is associated with decreased risk of adverse outcomes in terms of fracture healing. We hypothesize that the higher complication rates observed in TTC nailing compared to ankle ORIF may result from greater disruption of local vascular supply during intramedullary reaming, increased soft tissue trauma, and biomechanical alterations due to loss of subtalar and ankle joint motion.
Our findings differ from several recent studies that have reported favorable outcomes with TTCA, particularly in elderly or medically complex populations. A recent retrospective cohort by Balziano et al 1 found a lower complication and revision rate with TTC nailing compared with ORIF in extremely elderly patients (mean age 88.6 years), although patient-reported outcomes were better in the ORIF group. Additionally, Georgiannos et al 6 conducted a randomized controlled trial (RCT) of 87 elderly patients with fragility fractures and reported a significantly lower overall complication rate with TTCA (8.1%) compared to ORIF (33.3%). Furthermore, their study found that only 2.7% of TTCA patients required reoperation within 1 year, whereas 13.8% of ORIF patients needed a secondary procedure. Similarly, Taylor et al 17 observed a 90% union rate with TTCA in a cohort of osteoporotic ankle fractures, with a relatively low infection rate of 5%. In the specific context of diabetic patients, where ankle fractures carry extreme risk, Ebaugh et al 5 reported that primary TTC nailing resulted in limb salvage in 96% of cases with an acceptable 18.5% complication rate and no symptomatic nonunions. These studies have been interpreted as support for primary arthrodesis in lieu of ORIF for select high-risk patients, under the premise that avoiding plates and screws in poor-quality bone or soft tissue will reduce failures. However, their small sample sizes limit their generalizability, and our findings from a much larger cohort suggest that these benefits may not extend to broader patient populations.
Recent large-scale retrospective analyses align more closely with our results. Jordan et al 8 conducted a systematic review and found that TTCA produce worse functional outcomes with a complication rate of approximately 18% to 23%. Interestingly, evidence from other fracture contexts suggests that the benefit of arthrodesis in preventing nonunion may depend on injury severity. In the setting of highly comminuted pilon fractures (AO/OTA type C3 distal tibia fractures), a recent comparative study found primary tibiotalar fusion lowered the nonunion rate relative to ORIF (nonunion in 1 of 16 fusion cases vs 5 of 19 ORIF cases). 2 In that severe intra-articular fracture scenario, primary arthrodesis achieved more reliable healing and comparable functional outcomes to ORIF. However, our results indicate that for typical malleolar ankle fractures, ORIF had a higher union success.
It is worth noting that the quality of evidence prior to our study was generally low: many were Level IV case series. Recognition of this gap exists, with calls for more robust data. Notably, a multicenter randomized trial (110 patients) is currently in progress to compare ORIF with TTC nailing in elderly ankle fractures, reflecting the growing interest in resolving this clinical dilemma. 18 Until such trials mature, our large database study provides the strongest evidence to date, and it suggests that TTCA is associated with greater occurrence of adverse outcomes compared with ORIF.
The primary strength of our study is its large sample size, making it the most extensive comparative analysis of ORIF vs TTCA in trimalleolar fractures to date. The use of a nationally representative database enhances the generalizability of our findings. Additionally, PSM mitigates selection bias and strengthens the validity of our comparisons. However, as a retrospective study relying on administrative coding, our findings are subject to potential coding inaccuracies and residual confounding. A key limitation of the NRD is its discharge-based, calendar-year structure, which prevents tracking patients across years and limits assessment of long-term outcomes like nonunion or malunion. To allow for at least 90 days of follow-up, we restricted outcome identification to discharges in the first 9 months, excluding late-year cases to reduce misclassification. However, this limited window may underestimate true complication rates, as diagnoses like nonunion are rarely confirmed within 30 days.
Furthermore, the NRD lacks clinical details such as imaging, so complication coding depends on billing accuracy. Comorbidities were identified solely through diagnosis codes and could not be confirmed through chart review or lab data. Although we used standardized and previously validated ICD-10 coding strategies, the accuracy of these codes in representing active, clinically relevant comorbidities may vary. Because of the limitations of the data set, the severity of comorbidities were not able to be assessed, which could impact postoperative outcomes. Variables such as fracture displacement or comminution, soft tissue envelope integrity, timing of surgery, surgical technique including joint preparation (or lack thereof), surgeon experience, surgeon fellowship training (Trauma vs Foot & Ankle), and intraoperative findings are not captured in administrative coding. Specific details regarding fixation of the posterior malleolus in the ORIF group could not be determined because of limitations in the coding granularity of the database. As a result, we are unable to report the rate of posterior malleolar fixation, which may influence outcomes and represents a limitation of our study. Furthermore, the NRD does not provide data on intraoperative details such as use of bone grafts, structural grafting, or biologic adjuncts (eg, BMP, DBM), which are known to influence fusion success in TTCA. 14
These factors likely influenced the decision to pursue TTCA vs ORIF and may also impact complication risk, introducing the potential for confounding by indication. Although we employed PSM and multivariable regression to mitigate observable differences between groups, unmeasured confounding remains a source of bias. Another possible limitation of this study is that the codes used to isolate TTCA by tarsal fusion is not specific to the subtalar joint, and although we believe that most cases included represent TTCA, this possible misclassification could introduce minor variability in the cohort. This study is also limited by our use of a composite “any complication” outcome, which groups adverse events of varying clinical severity. Although we recognize that individual complications carry different implications, the low frequency of many individual events within the respective “risk” cohorts restricted our ability to perform meaningful stratified analyses.
Our use of a composite endpoint was therefore a pragmatic decision to assess overall complication burden in relation to patient risk status and treatment modality. Additionally, length of stay may have been influenced by factors unrelated to the surgical procedure itself, such as medical clearance, social support, or concurrent medical management. The NRD does not capture these nonsurgical contributors to hospitalization duration. Although prior studies offer valuable insights into well-described patient cohorts and surgical techniques, their small sample sizes limit statistical power and generalizability. Our analysis of a larger cohort complements these studies by capturing population-level trends and complication rates across diverse hospitals, albeit with reduced clinical granularity. Thus, our findings should be considered alongside, rather than as replacements for, high-quality prospective data.
Our findings suggest that TTCA is associated with a greater risk of complication compared with ORIF. The significantly higher nonunion and readmission rates in the TTCA group suggest that primary arthrodesis should be reserved for select cases where ORIF is unlikely to be successful. Although TTCA may facilitate early weightbearing, its higher complication rates warrant careful patient selection and close postoperative monitoring. Surgeons considering TTCA should employ meticulous technique, including joint preparation and bone grafting, to optimize fusion rates and minimize complications.
Conclusion
In this large national database analysis, TTCA was associated with significantly higher complication and readmission rates compared with ORIF in patients with trimalleolar ankle fractures. Although these findings challenge recent smaller studies favoring TTCA in high-risk populations, important limitations including limited follow-up duration and lack of clinical detail warrant cautious interpretation. These results suggest that ORIF may remain preferable for most patients with trimalleolar fractures, with TTCA reserved for carefully selected cases where conventional fixation is unlikely to succeed. Well-designed prospective studies with longer follow-up are critically needed to definitively guide treatment decisions in this challenging patient population.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251375027 – Supplemental material for Tibiotalocalcaneal Arthrodesis vs Open Reduction Internal Fixation for Trimalleolar Ankle Fractures in High-Risk Patients: A National Database Analysis
Supplemental material, sj-pdf-1-fao-10.1177_24730114251375027 for Tibiotalocalcaneal Arthrodesis vs Open Reduction Internal Fixation for Trimalleolar Ankle Fractures in High-Risk Patients: A National Database Analysis by Abhiram Dawar, Gnaneswar Chundi, Zachary Fuller, David B. Ahn, Avani A. Chopra, Sheldon S. Lin and Tuckerman Jones in Foot & Ankle Orthopaedics
Footnotes
Appendix
International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) Codes for Comorbidities.
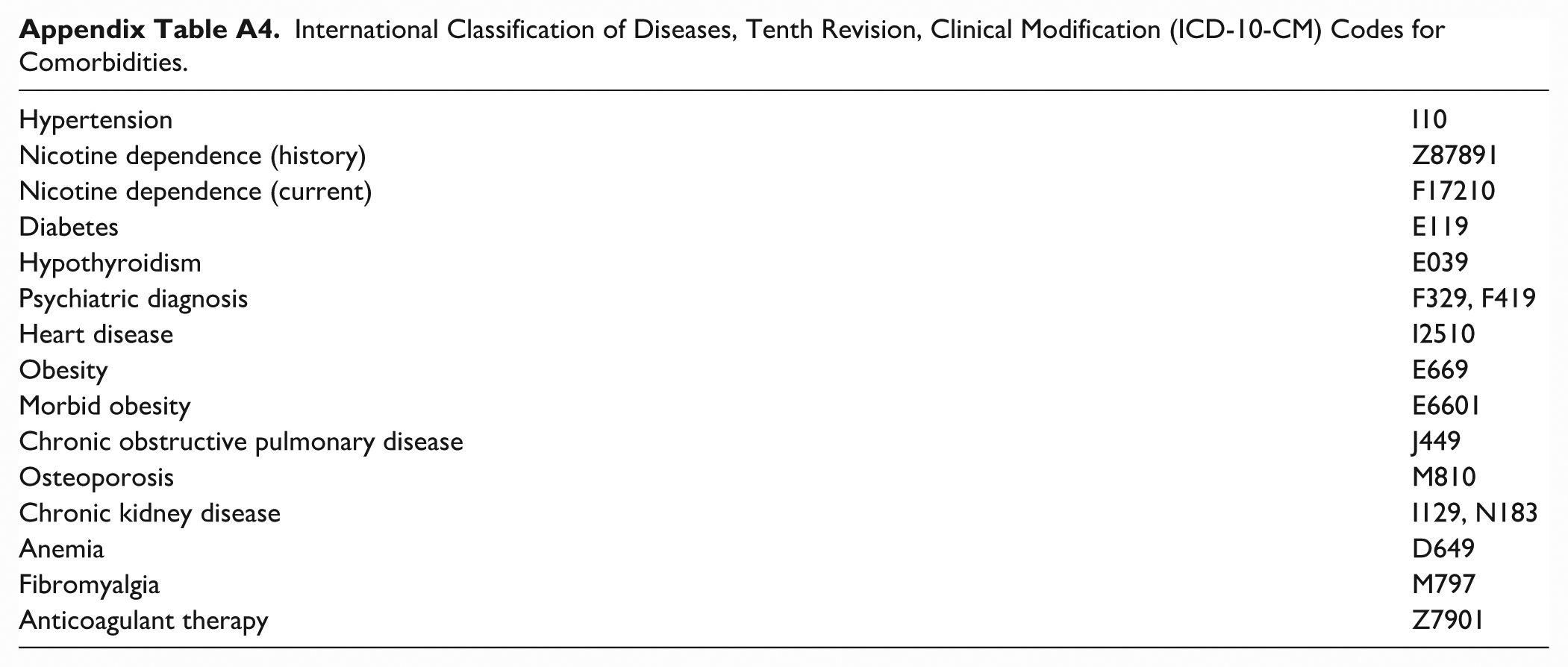
| Hypertension | I10 |
| Nicotine dependence (history) | Z87891 |
| Nicotine dependence (current) | F17210 |
| Diabetes | E119 |
| Hypothyroidism | E039 |
| Psychiatric diagnosis | F329, F419 |
| Heart disease | I2510 |
| Obesity | E669 |
| Morbid obesity | E6601 |
| Chronic obstructive pulmonary disease | J449 |
| Osteoporosis | M810 |
| Chronic kidney disease | I129, N183 |
| Anemia | D649 |
| Fibromyalgia | M797 |
| Anticoagulant therapy | Z7901 |
Ethical Approval
Ethical approval was not sought for the present study because this study used publicly available, deidentified data from the Healthcare Cost and Utilization Project, Nationwide Readmissions Database.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data Availability Statement
Data used in this study is publicly available through the Healthcare Cost and Utilization Project, Nationwide Readmissions Database (HCUP NRD).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.