
Abstract
Background:
The clinical treatment of Weber B fibular fractures has primarily focused on the symmetry of the medial clear space. Numerous radiographic studies demonstrate no change in tibiotalar contact area until the deltoid ligament is disrupted. In contrast, more recent studies using weightbearing CT scan (WBCT) and 3D volume analysis suggest that medial clear space (MCS) volume can in fact increase in the setting of a Weber B fibular fracture even if initial radiographs are reassuring, possibly because of a loss of fibular buttress. This study aims to evaluate the ability of WBCT to quantify the impact of isolated Weber B fractures on MCS volume (3D), as well as understand the implication of increasing fibular displacement among patients with a symmetric MCS distance (1D) on initial radiographs.
Methods:
The study group included 18 patients with unilateral Weber B ankle fractures who underwent preoperative bilateral foot and ankle WBCT. The control group consisted of 60 patients with forefoot/midfoot conditions without ankle injury who underwent similar imaging. Measurements on WBCT images included (1) MCS distance; (2) syndesmotic area; (3) anterior, middle, and posterior distal tibiofibular distance; (4) fibular rotation; (5) distance from fibular tip to plafond; and (6) fibular fracture displacement. Additionally, volumetric measurements included (1) MCS volume, (2) syndesmotic joint volume from the tibial plafond extending to 3 cm and 5 cm proximally, and (3) lateral clear space volume were calculated. Area under the receiver operating characteristic (ROC) curve (AUC) analysis and Delong test were used, and optimal cutoff values to distinguish between stable and unstable Weber B fractures without syndesmotic instability and MCS widening were determined using Youden J statistic.
Results:
Among patients with unilateral Weber B ankle fractures, all WBCT measurements showed no side-to-side difference in any parameter, except MCS volume (P values < .001). When compared to the uninjured side, fibular displacement up to 2 mm and up to 4 mm was associated with MCS volume increases of 37.1% and 51.8%, respectively, compared with the contralateral uninjured side. Based on ROC analysis and Youden J statistic, a fibular fracture displacement of 2.3 mm was identified as the optimal threshold associated with a significant increase in MCS volume (AUC, 0.81; sensitivity, 77.8%; specificity, 80%). The control group showed no side-to-side difference in any of the measurements.
Conclusion:
In this preliminary study using WBCT, 3D MCS volume measurements showed statistical differences in Weber B fibular fractures compared with the contralateral side, even when 1D distance measurements appeared symmetric. A displacement threshold of 2.3 mm was identified through ROC analysis, although the clinical significance of these volumetric changes remains unclear and requires validation through clinical outcome studies.
Level of Evidence:
Level III, comparative diagnostic study.
Introduction
Ankle fractures are among the most common injuries encountered in foot and ankle orthopaedic practice, with supination external rotation (SER) injuries resulting in Weber B fractures accounting for approximately 50% of all cases. 12 Despite their prevalence, distinguishing between stable and unstable fracture patterns remains a significant clinical challenge especially in SER II ankle fractures. The gold standard for assessing ankle mortise stability in SER injuries has traditionally been measuring the medial clear space (MCS) on weightbearing or gravity stress radiographs.9,21,26,32 Some argue that weightbearing (WB) radiographs may offer a more accurate predictor of stability. 14 In patients with an anatomically reduced mortise on WB radiographs, emerging evidence suggests that nonoperative management with protected WB and functional rehabilitation generally yields successful outcomes.14-16,20,27
The ongoing debate surrounding the optimal management of SER II Weber B ankle fractures is largely fueled by discrepancies in the literature regarding which diagnostic parameters most accurately predict fracture stability. Radiographic studies on Weber B fibular fractures suggest that significant changes in tibiotalar contact area typically occur only after deltoid ligament disruption. Even 1 mm of talar displacement can significantly alter ankle biomechanics, leading to accelerated ankle arthrosis. 4 Traditionally, the deltoid ligament has been considered the primary medial stabilizer, with talar displacement occurring only if it is compromised. 13 However, Ramsey and Hamilton reported that lateral talar displacement in isolated fibular fractures, even with an intact deltoid ligament, can be sufficient to alter tibiotalar joint dynamics, thereby supporting the need for surgical intervention. 25 Similarly, Curtis et al 6 found that fibular shortening and external rotation, even in the presence of an intact deltoid ligament, led to a decrease in tibiotalar contact area.
Recent advancements in imaging, particularly with weightbearing CT (WBCT) and 3D volume analysis, have challenged this conventional understanding.2,3 These studies reveal that the medial clear space (MCS) volume, a 3-dimensional (3D) measurement distinct from traditional 1-dimensional (1D) measurements of the MCS distance, can increase in the presence of a Weber B fibular fracture even if initial radiographs suggest a symmetric MCS. Adding further complexity, the role of fibular displacement as a predictor of instability remains contentious.5,28,31 Although some studies support the use of fibular displacement severity as an indicator of instability, others find it to be an unreliable parameter.
Such inconsistencies in the literature have inevitably led to uncertainty regarding the most effective diagnostic criteria and treatment strategies for Weber B fractures. 18 This study aims to evaluate the ability of WBCT to quantify the impact of isolated Weber B fractures on MCS volume (3D), as well as elucidate the implication of increasing fibular displacement among patients who had a symmetric MCS on initial weightbearing radiographs.
Methods
Study Population and Design
After obtaining Institutional Review Board approval, a retrospective review was conducted on bilateral foot and ankle weightbearing computed tomography (WBCT) acquired with the PedCAT system (CurveBeam) at an academic medical institution. WBCT imaging captured complete views of the bilateral ankles and the entire foot. The study group included patients who had undergone surgical fixation for unilateral Weber B lateral malleolar fractures, with intraoperative confirmation of a stable syndesmosis. The control group included patients who underwent WBCT for Lisfranc joint injuries or distal forefoot conditions without any associated ankle injury and were able to fully bear weight. Patients were excluded if they had bilateral foot or ankle trauma, were younger than 18 years old, had evidence of ankle arthritis, and patients with ipsilateral distal tibial injuries extending to the incisura. All patients included in the study demonstrated medial clear space (MCS) <4 mm on initial weightbearing radiographic evaluation.
The patient group consisted of 18 patients (36 ankles) with unilateral Weber B lateral malleolar fracture who were found to have no syndesmotic or medial ankle instability on stress testing at the time of surgery. All patients underwent preoperative WBCT with unprotected ankles during scanning. All these patients exhibited symmetric MCS on both the initial radiographs and WBCT. Indications for surgical fixation included syndesmotic tenderness in 12 patients, the presence of intra-articular loose bodies in 2 patients, and displaced lateral malleolar fractures in 4 patients. On the other hand, the control group was composed of 60 patients (120 ankles) with no ankle injuries who underwent WBCT for unrelated forefoot or midfoot conditions. Demographic data collected for both groups included age, gender, body mass index, and the time interval between the initial injury and the acquisition of WBCT imaging.
Weightbearing CT Measurement Methods
Measurements were obtained bilaterally on both the injured and uninjured ankle. WBCT-based measurement techniques—ranging from 1D linear assessments to 2D area and 3D volumetric analyses—have been previously described to evaluate medial and lateral clear space, the syndesmotic joint, and fracture morphology.4,7,11,19,22 Axial images of the distal syndesmosis taken 1 cm proximal to the tibial plafond were used to measure anterior, middle, and posterior tibiofibular distances, fibular rotation, and syndesmotic area (Figure 1).7,11,19,22 Sagittal plane images were used to assess lateral malleolar fracture displacement, whereas coronal images were used to evaluate fibular shortening by comparing the vertical distance from the fibular tip to the tibial plafond against the contralateral side.4,24,29 Medial clear space measurements were performed on the midcoronal slice of the CT scan. 1
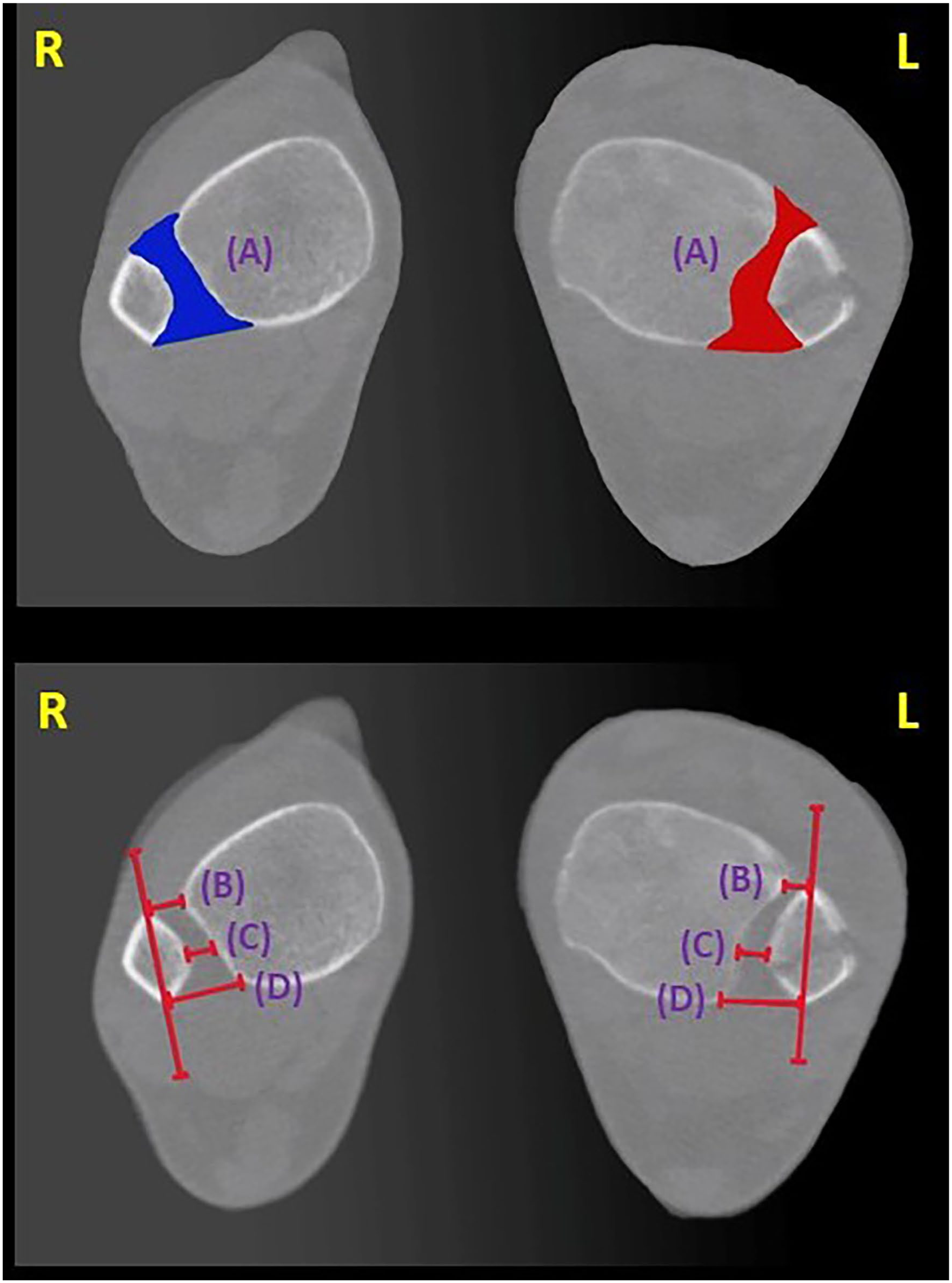
Weightbearing computed tomography syndesmotic joint measurements in a patient having left-side Weber B fracture. Axial view images. (A) Syndesmotic joint area (shaded area). (B) Distance between the anterior quadrant of the syndesmotic joint. (C) Distance between the middle quadrant of the syndesmotic joint. (D) Distance between the posterior quadrant of the syndesmotic joint. L, left; R, right.
Three-dimensional volumetric assessments of the distal tibiofibular articulation were conducted using WBCT data, with regions of interest extending from the level of the tibial plafond to 3 cm and 5 cm proximally (Figure 2).2,3 This method, previously validated, demonstrated excellent interrater reliability with intraclass correlation coefficients (ICCs) of 0.93 (95% CI, 0.89-0.95) and 0.94 (95% CI, 0.90-0.96), respectively.
2
Additional volumetric measurements included quantification of the medial and lateral clear spaces, defined respectively as the space between the medial malleolus and the talar dome, and between the lateral malleolus and the talar dome as previously described.
4
Axial CT images with a standard slice thickness of 0.3 mm were used to calculate the medial clear space (MCS) area on each slice, beginning at the most distal portion of the medial tibiotalar joint and extending superiorly to the top of the talar dome (Figure 3).
4
A similar method was applied to determine the lateral clear space (LCS) area, using the same 0.3-mm axial slices spanning from the inferior margin of the lateral talofibular joint to the dome of the talus (Figure 3).
4
Thereafter, the volume of the syndesmotic joint extending up to 3 cm and 5 cm proximally as well as MCS and LCS was created and measured in the axial orientation utilizing following the formula:

Weightbearing computed tomography syndesmotic joint measurements in a patient having left-sided Weber B fracture. Anterior view images. (A) Syndesmotic joint volume up to 3 cm above the joint line. (B) Syndesmotic joint volume up to 5 cm above the joint line. L, left; R, right.

Weightbearing computed tomography medial clear space (MCS) and lateral clear space (LCS) volumetric measurements in a patient having left-side Weber B fracture. (A) Axial view: (i) MCS area (shaded area); (ii) LCS area (shaded area). (B) Volumetric measurement of the MCS and LCS joints. L, left; R, right.
Statistical Analysis
The baseline characteristics were described using percentage and frequency for categorical variables and mean ± SD for continuous values. Statistical analyses were performed to assess demographic differences between the patient and the control groups using χ2 tests for categorical variables. To test the primary hypothesis that the degree of fibular translation correlates with tibiotalar instability with associated increase in MCS volume, a paired t test was used. Additionally, a receiver operating characteristic (ROC) curve analysis, along with the Delong test, was performed to determine the minimum fibular fracture displacement required to accurately identify an unstable Weber B ankle fracture was determined using Youden J statistic. An area under the curve (AUC) of 0.5 to 0.6 suggests no discrimination (ie, no differentiation between stable and unstable fractures), 0.6 to 0.7 is considered poor, 0.7 to 0.8 is considered acceptable, 0.8 to 0.9 is considered excellent, and more than 0.9 is considered outstanding. 8 In this study, a P value <.05 was considered as statistically significant. SPSS, version 26.0, was used to analyze the data (IBM SPSS Statistics, Armonk, NY).
Results
WBCT 1D, 2D, and 3D Measurements
There were no significant differences between the patient and control groups in terms of age, sex, body mass index, or the interval between injury and WBCT acquisition (Table 1). Among patients with a unilateral Weber B lateral malleolar fracture, all WBCT measurements showed no side-to-side difference in any parameter, except MCS volume, which showed a statistically significant increase (P values <.001; Table 2). The results are summarized in Table 2. In the control group, however, no significant differences in any measurements were observed between the 2 uninjured ankles, including MCS volume (Table 3). The results are summarized in Table 3.
Baseline Characteristics of Individuals in the Patient and Control Groups.

Abbreviations: BMI, body mass index; WBCT, weightbearing computed tomography.
Bilateral Differences in Weightbearing CT Measurements in the Patient Group.

Abbreviations: LCS, lateral clear space; MCS, medial clear space; TP, tibial plafond; WBCT, weightbearing computed tomography.
Boldface indicates significance (P < .05).
Bilateral Differences in Weightbearing CT Measurements in the Control Group.
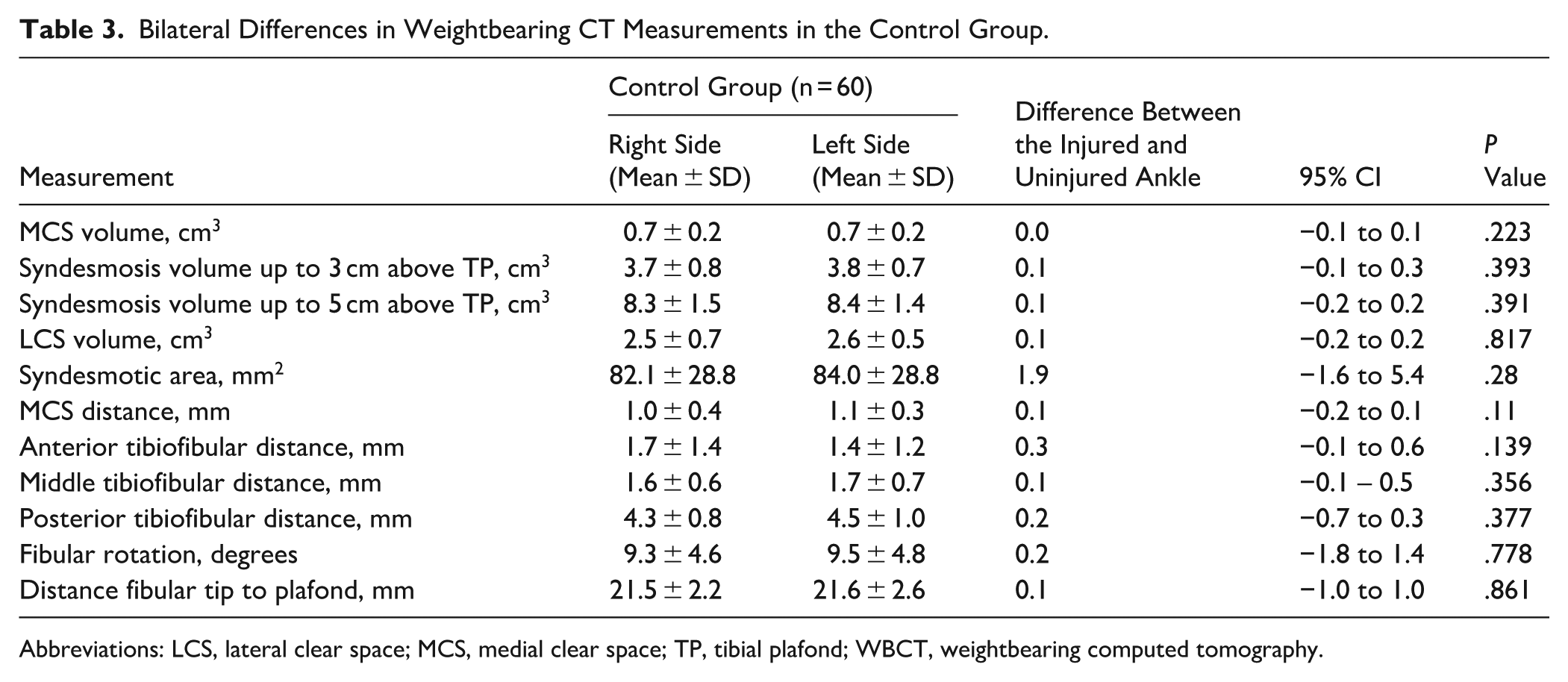
Abbreviations: LCS, lateral clear space; MCS, medial clear space; TP, tibial plafond; WBCT, weightbearing computed tomography.
In the patient group, when compared to the uninjured side, fibular displacement up to 2 mm and up to 4 mm increased MCS volume by 37.1% (0.23 cm3; P = .001) and 51.8% (0.3 cm3; P = .003), respectively (Table 4). Moreover, ROC curve analysis revealed that fibular displacement of 2.3 mm and above resulted in an increased MCS volume. This threshold yielded an area under the curve (AUC) of 0.81 (95% CI 0.75-0.90), with an accuracy of 78.9%, sensitivity of 77.8%, specificity of 80%, positive predictive value of 80%, and negative predictive value of 78.3%.
Bilateral Differences in Weightbearing CT Medial Clear Space Volume Measurements by Degree of Fibular Displacement in the Patient Group.

Discussion
Historically, the stability of a Weber B ankle fracture has been assessed based on evaluation of MCS widening as a surrogate for tibiotalar instability. A prior study by Bhimani et al 4 demonstrated the utility of WBCT in diagnosing syndesmotic instability, even in the presence of a lateral malleolus fracture. Irrespective of the presence or absence of syndesmotic instability, however, patients with a lateral malleolus fracture were noted to have a significantly increased MCS volume (3D) even if MCS area (2D) and distance (1D) measurements were symmetric. Whether an isolated SER II distal fibular fracture affects these measurements—and consequently, whether WBCT can reliably detect tibiotalar instability in such cases—remains unclear.
The present study found that MCS volume was greater in patients with isolated Weber B fibular fractures even if initial radiographs demonstrate a symmetric MCS and even if distance measurements on WBCT were similarly symmetric. These findings raise the possibility that tibiotalar displacement in Weber B fractures may occur in planes other than the coronal plane, although the clinical implications of such displacement patterns remain to be determined. Because this study did not correlate volumetric asymmetry with patient outcomes, these findings should be interpreted as radiographic observations rather than direct indicators of instability requiring surgery.
The 2.3-mm displacement threshold identified in this study was derived using MCS volume as the reference standard rather than clinical instability or outcomes. This threshold should therefore be considered a statistical finding rather than a clinically validated criterion for treatment decisions. Given the current lack of clarity provided to clinicians with current imaging modalities, these findings suggest that 3D WBCT may serve a role in the management of SER II Weber B ankle fractures with symmetric MCS on initial imaging. However, several important limitations must be acknowledged when interpreting these findings. First, our “control” group consisted of patients with forefoot/midfoot pathology rather than completely healthy individuals, which may limit the generalizability of our normal reference values. Second, the clinical significance of the statistical differences we observed in MCS volume remains uncertain without correlation to clinical outcomes or long-term follow-up data.
Despite the prevalence of Weber B fibula fractures, determining stability remains challenging when 1D MCS measurements appear symmetric. The historic focus has been on the deltoid ligament and its role as a tether to prevent tibiotalar translation. On the other hand, the distal fibula has cartilage on its medial aspect allowing it to engage the lateral talus as a lateral buttress. With increasing Weber B fracture displacement (both lateral translation and shortening), the loss of this bony buttress may result in subtle changes to the tibiotalar articulation whose long-term implications are unclear, especially in younger, more active patients. There are few instances elsewhere in orthopaedics in which we rely on a soft tissue restraint to overcome a loss of bony stability, and subtle rotational changes to the tibiotalar relationship may ensue.
Although MCS widening guides decision making, there is no consensus on the threshold of MCS asymmetry that implies instability. A 2017 survey of Dutch trauma and orthopaedic surgeons found many opted for surgery when MCS exceeded 4 mm on mortise radiographs, even without confirmed medial injury. Further diagnostics, like MRI or stress radiographs, were rarely used for MCS widths of 4-6 mm, leading to potential overtreatment. 30 Additionally, Karkkola et al 17 retrospectively evaluated long-term functional and radiologic outcomes in 160 ankle fractures treated according to stability classification and found that, at a mean follow-up of 12 years, 96% of patients with stable fractures treated nonoperatively had very good to excellent functional outcomes, compared with 82% in the surgically treated unstable group. Similarly, O’Keefe et al, 23 in the CROSSBAT multicenter randomized controlled trial, evaluated 160 patients with isolated Weber B fractures and minimal talar shift. Of these, 77 patients (40 surgical, 37 nonoperative) were available for a minimum 5-year follow-up. The authors found no clinically or statistically significant differences in outcomes between treatment groups, whereas surgery was associated with a higher rate of adverse events. Interestingly, when evaluated under a 3D lens, our study determined clear evidence of some degree of MCS asymmetry in Weber B fractures with the change in fibular buttress.
Fibular displacement may help predict instability, although debate persists. In 2004, Harris and Fallat 13 recommended ORIF for SER injuries, such as Weber B fractures, with ≥2 mm of lateral, posterior, or superior fibular displacement. Earlier studies linked ≤2 mm displacement with normal MCS to a 97% positive predictive value of stability; however, Shahien and Tornetta 28 found no correlation, noting many unstable cases lacked fibular displacement. Similarly, van Leeuwen et al 31 found fibular displacement to have a poor correlation with MCS. In contrast, Cavanaugh et al 5 revealed significant ability to predict MCS widening for both lateral fibular displacement (P = .002) and anterior-to-posterior fibular gap (P = .001). In a biomechanical study, Gregersen et al 10 examined whether fibular plate fixation restores ankle stability in an SER4a cadaveric model. They evaluated lateral translation, valgus, and rotational stability across 3 ankle positions—10 degrees dorsiflexion, neutral, and 20 degrees plantarflexion—under 3 conditions: intact, injured without fixation, and injured with fibular plate fixation in 15 cadavers. Their findings showed that fibular fixation improved external rotation stability but did not fully restore native ankle mechanics. Talar tilt and shift remained unchanged between plated and nonplated models at neutral ankle position, and only minor improvements were noted in internal rotation. Our findings highlight that a more comprehensive 3D analysis may better assess stability. It is understood that an injured deltoid ligament contributes to MCS widening, but it is possible that losing integrity of the fibular buttress may alter the MCS volume. However, such findings may not be detected in 2D radiographic evaluation nor on 3D CT evaluation if relying on 1D distance or 2D area measurements. Rather than relying solely on 1D or 2D evaluations of MCS widening, integrating 3D imaging could more effectively capture both fibular displacement and MCS changes, enhancing predictive accuracy. It is critical to note that the long-term implications of more subtle increases in MCS volume are unclear. Statistical significance does not automatically equate to clinical significance. Although we detected measurable differences in MCS volume, the natural history and functional implications of these changes are unknown. Some degree of volume asymmetry may represent normal anatomical variation or adaptation that does not compromise clinical outcomes.
WBCT has provided a unique modality to optimize patient care by allowing 3D evaluation under physiological load. Prior research has assessed the utility of this technology in such as syndesmotic instability. 4 Limited by cost and the necessary improvements in AI software to quickly process images and provide clinicians with accurate evaluations, implementing 3D WBCT on a wide scale basis remains a challenge. Further studies are needed to assess the role of our findings in long term outcomes of SER II ankle fractures.
This study has limitations that should be considered when interpreting the results. First, our control group consisted of patients with forefoot/midfoot pathology rather than completely healthy individuals, which may affect the normative values and bilateral comparisons. Additionally, numerous studies have highlighted the need for bilateral comparison rather than absolute measurements in using WBCT, and our sample size may be insufficient to establish reliable absolute displacement thresholds. When honing in on an absolute fibular displacement measure, a larger sample size may improve the generalizability of the findings. Second, although 3D WBCT provides detailed spatial assessment, it may not fully replicate the complex forces acting on the ankle during functional activities, potentially limiting its ability to predict instability. Third, as this was a retrospective study without a power analysis, the generalizability of our findings may be limited. In addition, our analysis focused solely on radiographic parameters without correlation to clinical outcomes, which limits the ability to draw conclusions about treatment decisions or long-term function. However, we included all patients who met the inclusion criteria during the study period to reduce selection bias and enhance the clinical relevance of our results. Additionally, because all patients in the fracture group ultimately underwent surgery for varied indications, the findings may not be generalizable to nonoperatively managed Weber B fractures, which represent a large proportion of such injuries. Fourth, there was variability in the time from injury to WBCT acquisition (mean 25 ± 45 days), which may have introduced heterogeneity related to weightbearing status, ligamentous healing, and early bony remodeling. This variability could have affected the imaging findings and introduced uncontrolled variance in our analyses, which should be considered when interpreting the results. Fifth, the 2.3-mm threshold represents a statistical association between displacement and volume changes rather than a clinically validated cutoff for instability. This threshold was derived using our own volumetric measurements as the reference standard, creating a somewhat circular validation process that limits its clinical applicability. As such, this cutoff represents a value that needs to be validated through clinical outcomes, biomechanical testing, or direct assessment of deltoid integrity. While it provides insight into displacement patterns associated with increased MCS volume, further studies are needed to confirm its clinical relevance. Finally, measurement techniques such as area and volume may not be available in most CT imaging viewing systems, and software enhancements are necessary before the widespread use of volumetric measurements can be integrated into the existing clinical practice. Thus, using automated measurement software may help reduce this bias. Future studies should aim to evaluate larger cohorts, standardize imaging protocols, and follow up patients over long-term to validate these findings and further explore the clinical implications of WBCT in assessing ankle stability.
Conclusion
This preliminary study demonstrates that WBCT can detect 3D volumetric changes in the medial clear space of Weber B fractures that are not apparent on traditional imaging, with a statistical association observed at 2.3 mm of fibular displacement. However, the clinical significance of these volumetric changes remains unknown. Before these findings can influence clinical practice, prospective studies with clinical outcome correlation are essential to determine whether these volumetric measurements provide clinically meaningful information beyond current assessment methods. The 2.3-mm threshold identified represents a statistical finding that requires validation through clinical studies rather than a treatment guideline.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251373078 – Supplemental material for Weightbearing CT Assessment of Medial Clear Space Volume Changes in Weber B Fractures: A Preliminary Analysis
Supplemental material, sj-pdf-1-fao-10.1177_24730114251373078 for Weightbearing CT Assessment of Medial Clear Space Volume Changes in Weber B Fractures: A Preliminary Analysis by Rohan Bhimani, Marguerite A. Mullen, Soheil Ashkani-Esfahani, Colin O’Neill, Gergory R. Waryasz, Gino M.M.J. Kerkhoffs, Christopher W. DiGiovanni and Daniel Guss in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
This study was approved by the Institutional Review Board of the hospital.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Soheil Ashkani-Esfahani, MD, reports general disclosures from Arthrex, Inc: research support; Bioretec Ltd: research support; Formlabs Inc: research support; Ipsen Pharma: paid presenter or speaker; Neatsy AI: research support; Orthofix, Inc: research support; Ossio Fiber Inc: research support; Stryker: research support; The Spine Journal: editorial or governing board. Gergory R. Waryasz, MD, reports general disclosures from American Orthopaedic Foot & Ankle Society: board or committee member; Arthrex, Inc: research support; Extremity Medical: paid presenter or speaker; OSSIO: paid presenter or speaker; Reign medical: IP royalties; Turner Imaging: research support; VKTRY: research support. Gino M.M.J. Kerkhoffs, MD, PhD, reports general disclosures from ESSKA: board or committee member; fa. Heel: unpaid consultant. Christopher W. DiGiovanni, MD, reports general disclosures from Arthrex, Inc: research support; Bristol-Myers Squibb: stock or stock options; Butterfly Network: research support; CreOsso: stock or stock options; Extremity Medical, Inc: paid consultant; stock or stock options; Extremity Medical, Inc: IP royalties; Foot & Ankle International: editorial or governing board; GE Healthcare: stock or stock options; Johnson & Johnson: stock or stock options; JOMI: IP royalties; Mediflix: stock or stock options; Medtronic: stock or stock options; Merck: stock or stock options; Neatsy: paid consultant; Orthofix, Inc: paid consultant; stock or stock options; OrthoScan, Inc: research support; Ossio: paid consultant; stock or stock options; Osso VR: stock or stock options; Paragon 28: stock or stock options; Pfizer: stock or stock options; Procter & Gamble: stock or stock options. Daniel Guss, MD, MBA, reports general disclosures from American Orthopaedic Foot & Ankle Society: board or committee member; Butterfly Network: research support; Ossio: paid consultant; stock or stock options; Paragon 28–fellowship funding: other financial or material support; Stryker fellowship grant via AOFAS: other financial or material support. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.