
Abstract
Background:
Distraction arthroplasty aims to treat ankle osteoarthritis while preserving the native ankle joint, often to prevent or delay ankle arthrodesis or total ankle replacement (TAR). No study to date has explored TAR outcomes in patients who have had prior distraction arthroplasty. Thus, this study described the clinical, radiographic, and patient-reported outcomes for TAR at minimum 2-year follow-up in patients who had undergone prior ankle distraction arthroplasty.
Methods:
This retrospective review included 19 ankles in 17 patients who underwent TAR at a single institution subsequent to ipsilateral distraction arthroplasty. The primary aims were to evaluate complication rate and patient satisfaction following TAR. PROMIS scores were obtained preoperatively and at minimum 2 years postoperatively. The proportion of patients who achieved the patient acceptable symptom state (PASS) threshold for each Patient-Reported Outcomes Measurement Information System (PROMIS) domain at final follow-up was used to assess patient satisfaction following TAR.
Results:
TAR was performed a mean of 5.3 ± 3.5 years following distraction arthroplasty. At mean 4.4-year follow-up after TAR, 18/19 (94.7%) ankles remained implanted. One ankle was revised because of failure of the talar component, and there were 4 additional reoperations. Radiographic complications were observed in 37% of patients at 2 years postoperatively. Patients experienced significant improvement at 2-year follow-up for PROMIS domains of Physical Function (P = .002), Pain Interference (P = .007), and Pain Intensity (P = .010). At final follow-up, PASS was achieved by 65% and 71% of patients in the Physical Function and Pain Interference domains, respectively, but only 35% in the Pain Intensity domain.
Conclusion:
TAR is a viable option to treat ankle osteoarthritis symptoms that persist after distraction arthroplasty. However, many of these patients present with a complex surgical history and, therefore, may be at a greater risk for reoperation. Thus, patients should be counseled appropriately before electing to proceed with distraction arthroplasty before more definitive surgical treatment options.
Level of Evidence:
Level IV, case series.
Introduction
Ankle osteoarthritis (OA) is a debilitating condition that affects approximately 1% of the world population 16 and is most commonly the result of high-energy tibial plafond fractures, bimalleolar ankle fractures, or recurrent ankle instability. 3 Post-traumatic ankle arthritis predominately affects a younger population with higher physical demands, which introduces challenges when devising treatment options. 10 Ankle arthrodesis (AA) has historically been the gold standard for treatment of ankle OA, but loss of ankle range of motion, changes in gait, 11 and increased stress at adjacent joints occurs. Although total ankle replacement (TAR) has emerged as a viable treatment option for ankle OA, literature investigating long-term outcomes are limited.
Ankle distraction arthroplasty is a surgical treatment option for ankle OA that has historically been used to prevent or postpone AA or TAR, particularly in young patients. 20 Unlike AA and TAR, distraction arthroplasty is a joint-preserving surgery that aims to optimize the regenerative capacity of the body by mechanically unloading the ankle joint with an external fixation frame. 3 Range of motion and intermittent synovial fluid pressure, 2 essential elements for nutrition and stimulation of chondrocytes, are maintained. Furthermore, because mechanical contact is eliminated, this process is theorized to initiate cartilage repair. 20 Cartilage repair mechanisms may also be further enhanced by significant periarticular bone turnover that occurs with ankle distraction. 20 Although ankle distraction arthroplasty has demonstrated clinical benefit,18,21,23 there is a considerable failure rate resulting in arthrodesis, TAR, or repeat distraction within the first 5 years following ankle distraction.13,20,23 Despite high rates of failure of ankle distraction and the emergence of TAR as a viable treatment option for ankle OA, no studies have investigated the outcomes of TAR in patients with prior distraction. The distraction that occurs during the procedure may lead to increased stiffness in the ankle, and adjuvant procedures performed at the time of surgery, such as ankle arthroscopy and microfracture, can negatively impact bone quality. Thus, distraction arthroplasty has the potential to negatively impact the outcomes of subsequent total ankle arthroplasty.
The purpose of this study was to report on the clinical and radiographic outcomes of primary TAR in patients with prior distraction arthroplasty at a minimum 2-year follow-up. We hypothesized that TAR patients with prior distraction arthroplasty would have high rates of radiographic complications, reoperations and revisions, and low rates of patient acceptable symptom state (PASS) achievement at 2-year follow-up.
Methods
Patients
Following institutional review board approval, a retrospective review of prospectively collected data within an institutional TAR patient registry was performed. All patients with a history of ankle distraction arthroplasty who underwent primary TAR between January 2011 and March 2022 at a single institution were identified. The TAR patient registry collects patient-reported outcomes (PROs), demographic information, surgical procedures performed, associated complications, reoperations, revision procedures, and radiographic data. A chart review was performed in order to verify the information found within the registry. Inclusion criteria included (1) individuals with a diagnosis of ankle arthritis, (2) individuals who had prior distraction arthroplasty performed, (3) individuals who underwent primary TAR between January 2011 and March 2022 at a single institution, and (4) minimum 2-year postoperative follow-up. Exclusion criteria included (1) patients undergoing revision TAR surgery and (2) patients with less than 2-year postoperative follow-up. Patients included in the study underwent surgery with one of 4 fellowship-trained foot and ankle orthopaedic surgeons with extensive prior experience in TAR.
Complications, Reoperations, and Revisions
Chart review was performed to identify complications, reoperations, and revision procedures. Reoperations were defined as any surgical procedure following primary TAR with retention of both metal components. Revision was defined as removal of the tibial and/or talar implant, conversion to arthrodesis, or amputation.1,27
Radiographic Analysis
Radiographic analysis was conducted using the digital Picture Archiving and Communication System (PACS) (General Electric Healthcare, UK). Weight-bearing anteroposterior (AP) and lateral radiographs were obtained preoperatively and at 1 year and 2 years postoperatively. Radiographic analysis was performed by a fellowship-trained foot and ankle surgeon masked to the surgeon who performed the TAR and the clinical outcomes.
Preoperative weightbearing radiographs were used to assess tibiotalar coronal alignment. Tibiotalar coronal alignment was measured on AP weightbearing radiographs using the midline tibiotalar ankle (TTA), defined by the angle between the anatomical axis of the tibia and a line tangent to the talar dome or talar component, respectively.7,14,25 The absolute difference between tibiotalar coronal alignment and 90 degrees was defined as tibiotalar coronal deformity; neutral tibiotalar coronal deformity was defined to be less than 5 degrees.7,14,25
Postoperative weightbearing radiographs were used to assess tibiotalar coronal alignment and tibiotalar offset, defined as the absolute difference between tibiotalar coronal alignment and 90 degrees. For patients who underwent revision and/or reoperation procedures, the last radiograph before the revision procedure was used for alignment measurements. Postoperative tibial implant alignment was measured on AP weightbearing radiographs using the angle between the anatomical tibial axis and the inferior border of the tibial component. The absolute difference between the tibial implant alignment and 90 degrees was defined as tibial component deviation. 25
Postoperative radiographs were also assessed for subsidence, radiolucency, and/or periprosthetic cyst formation. All available postoperative radiographs were used to assess progression, resolution, or presence of radiographic abnormalities. Subsidence was defined as a change of greater than 5 degrees in tibial implant alignment or a change of ≥5 mm in the vertical position of the talar component.5,8 Radiolucencies of greater than ≥2 mm around the implant were identified. Periprosthetic cysts were defined as hypodense zones measuring greater than 5 mm in diameter with peripheral sclerosis but no inner bone trabeculae. 4
Patient-Reported Outcomes
Patient-Reported Outcomes Measurement Information System (PROMIS) scores, including the Physical Function, Pain Interference, Pain Intensity, Global Physical Health, Global Mental Health, and Depression t scores, were collected preoperatively and at 1 and 2 years postoperatively. PROMIS is a validated tool that assesses patients’ perceptions of their physical, emotional, cognitive, and social health. 12 PROMIS scores are reported using a t score between 0 and 100. The national average within the Unites States is a t score of 50 with an SD of 10 points. 9 For PROMIS functional scores (Physical Function, Global Physical Health, and Global Mental), higher scores indicate greater physical function, physical health, and mental health, respectively (better outcomes). For PROMIS symptom scores (Pain Interference, Pain Intensity, and Depression), higher scores indicate greater pain interference, pain intensity, and depression (worse outcomes). 17 PROMIS scores were evaluated to determine if the PASS was achieved, as previously described for TAR patients by Shaffrey et al. 28 Score thresholds for each of the PROMIS domains were determined to assess patient satisfaction with surgical outcomes.
Statistical Analysis
A department-designated statistician performed the analysis of the collected data. Demographic data and complications were reported using descriptive statistics. Descriptive statistics were reported as mean, SD, and range for continuous variables, and frequency and percentage for discrete variables. To evaluate longitudinal changes in PROMIS outcomes over time, linear mixed-effects models (LMMs) were used. Each model included a random intercept for subject to account for within-patient correlation across repeated measures. Time point (baseline, 1-year, and 2-year) was modeled as a fixed effect to assess changes in outcome trajectories over time. Pairwise comparisons between all time points were conducted using estimated marginal means derived from the model, and the Bonferroni technique was applied to adjust for multiple comparisons and reduce the risk of type I error. Statistical significance was established at an alpha of .05. Analysis was conducted on R: A Language and Environment for Statistical Computing (R Core Team, Vienna Austria 2023) and the pROC. 24
Results
There were 19 ankles from 17 patients that met inclusion criteria and were included in the study analysis (Figure 1). The average time between distraction and subsequent TAR was 5.28 ± 3.52 (range, 0.96-13) years. There was a mean follow-up of 4.36 ± 2.79 years after TAR. There were 9 men and 10 women with an average age of 58.7 ± 10.9 years and an average BMI of 27.8 ± 4.9 (Table 1). Prior to TAR, patients had 2.6 ± 1.2 surgeries on average, inclusive of distraction arthroplasty. In addition to distraction, the majority of patients had prior ipsilateral foot or ankle surgery (15/19, 79%). Table 1 demonstrates the most common other procedures patients underwent, including arthroscopic debridement, open debridement, and ORIF. Concomitant procedures performed at the time of distraction can also be found in Table 1. Concomitant procedures performed at the time of TAR can be found in Table 2. There were 8 patients (42%) who had a tendon-Achilles lengthening, 2 (11%) who underwent a gastrocnemius recession, 7 (37%) who had medial malleolar prophylactic fixation, and 1 patient (5%) who had a medializing calcaneal osteotomy. No patients required subtalar fusion at the time of their primary TAR.

Flow diagram detailing the number of patients screened, excluded, and analyzed within the study.
Patient demographics for the cohort of primary TAR patients with prior distraction arthroplasty. Values are expressed as frequencies with percentages for categorical values and as means ± SD for continuous variables. *Other prior foot and ankle surgeries included peroneal tendon repair, supramalleolar ankle osteotomy, revision ORIF of tibia, gastrocnemius release, lateral ankle ligament reconstruction, and removal of hardware.
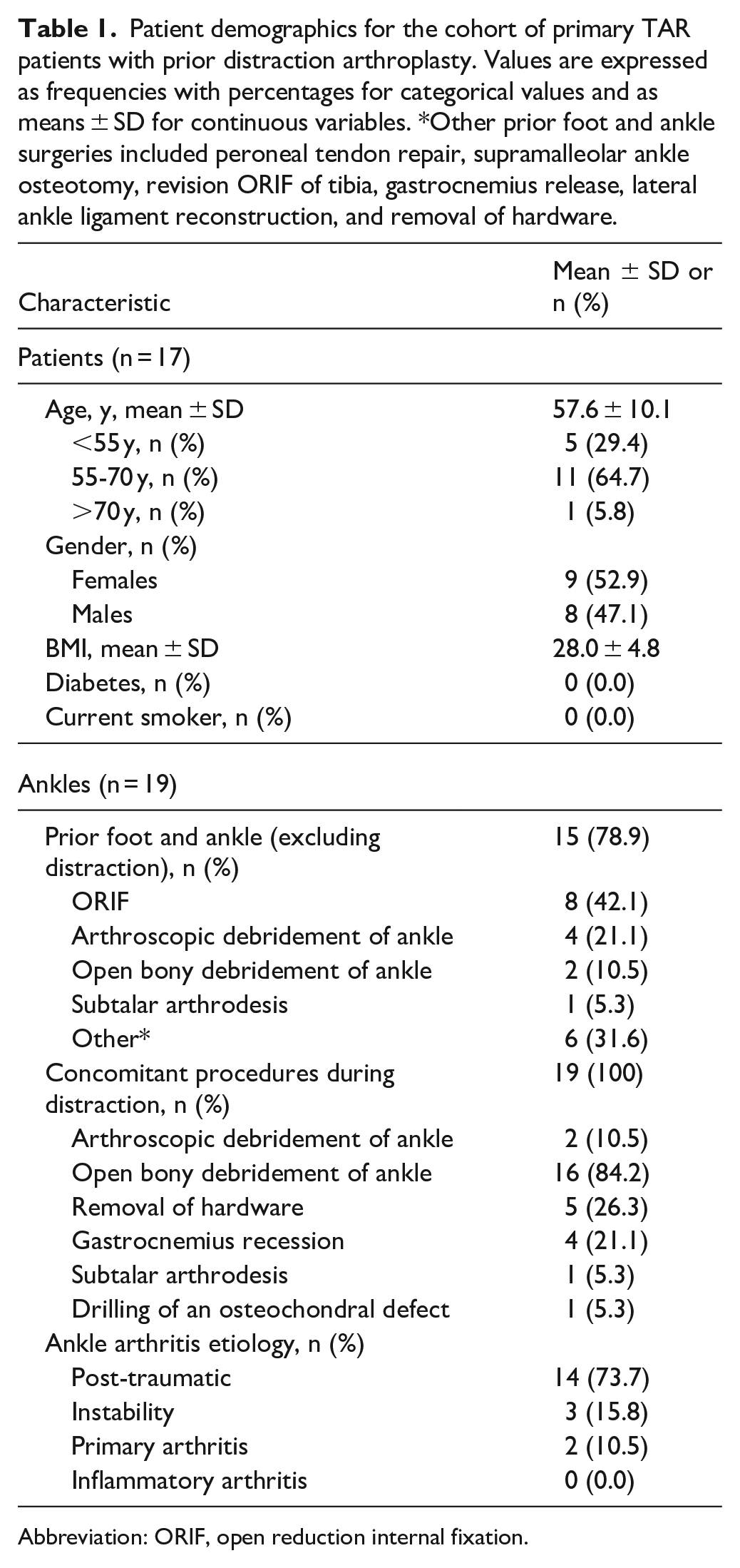
Abbreviation: ORIF, open reduction internal fixation.
Concomitant Procedures Performed at the Time of the Primary TAR for Patients in this Cohort (n = 19). a

Abbreviation: TAR, total ankle replacement.
The frequency of each procedure is stated, alongside the percentage of patients that underwent each procedure at the time of primary TAR.
Other concomitant procedures included cyst grafting (1), bone spur removal (1), talonavicular fusion (1), calcaneonavicular coalition excision (1), tarsal tunnel release (1), flexor digitorum longus tendon laceration repair (1), flexor digitorum longus tendon transfer (1), deltoid ligament release (1), subtalar joint release (1), and posterior tibial tendon lengthening (1).
Revisions, Reoperations, and Complications
One ankle (5%) required revision total ankle arthroplasty due to failure of the talus 1.72 years postoperatively. No other ankles required revision, for an overall success rate at 2 years of 95%. There were 4 (21%) additional ankles that required reoperation within the first year. One patient developed a flexor hallucis longus contracture and underwent flexor hallucis longus lengthening in the great toe and flexor digitorum longus tenotomy in the fourth toe, 1 patient developed arthrofibrosis and underwent posteromedial ankle arthrotomy and excision of scar tissue, 1 patient developed a suture abscess and underwent an irrigation and debridement, and one patient had a talonavicular nonunion after undergoing talonavicular fusion concomitant with TAR and underwent revision talonavicular fusion (Table 3). One other patient developed a superficial wound infection that was treated with antibiotics alone. There were no additional patients that required reoperation or revision at final follow up.
Instances of Revision and Reoperation Following Primary TAR. a
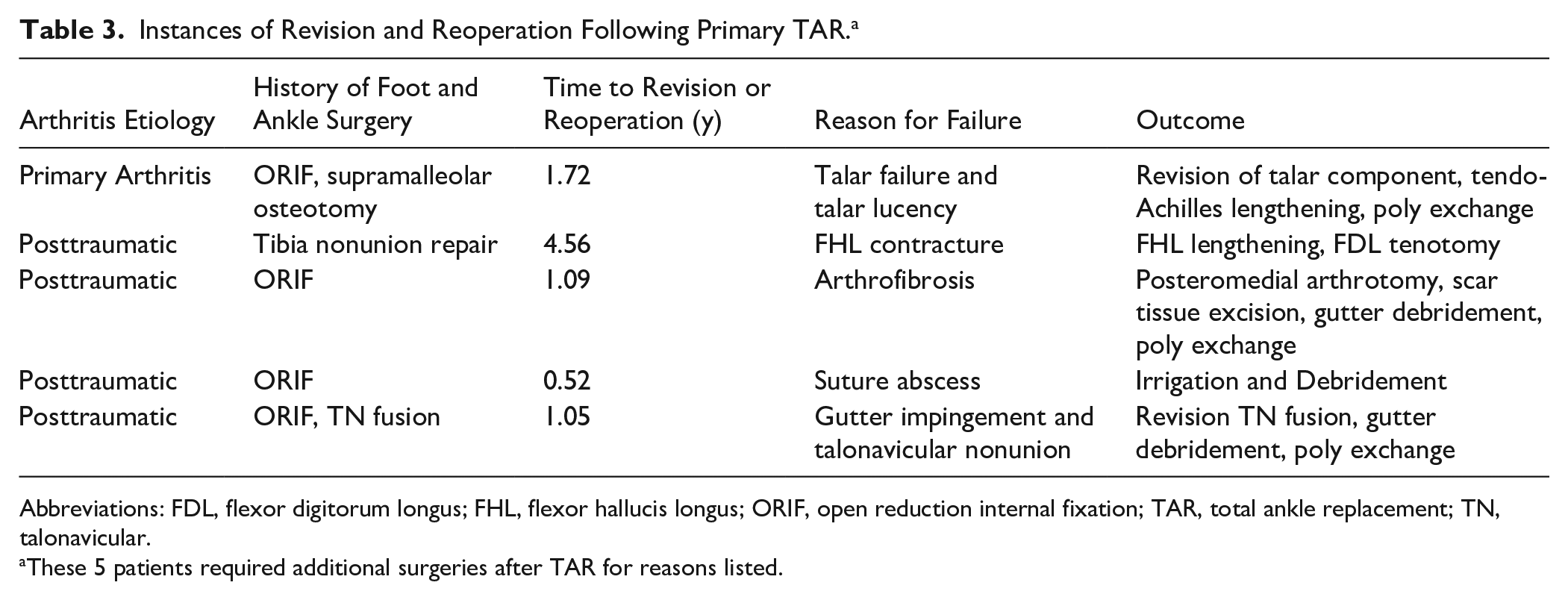
Abbreviations: FDL, flexor digitorum longus; FHL, flexor hallucis longus; ORIF, open reduction internal fixation; TAR, total ankle replacement; TN, talonavicular.
These 5 patients required additional surgeries after TAR for reasons listed.
Radiographic Outcomes
Preoperatively, the average absolute coronal tibiotalar deformity was 5.07 ± 5.19 degrees with a 95% CI ranging from 3.39 to 6.75 degrees, which demonstrated improvement to 1.05 ± 0.80 degrees postoperatively (P = .009). Radiographic complications were noted in 7 of 19 (37%) patients at final radiographic follow-up. Tibial subsidence was observed in 1 patient, tibial lucency was observed in 3 patients, and talar lucency was observed in 1 patient. One patient demonstrated both tibial and talar lucency. Additionally, 1 patient had periprosthetic talar cysts visible on radiographs (Figure 2).
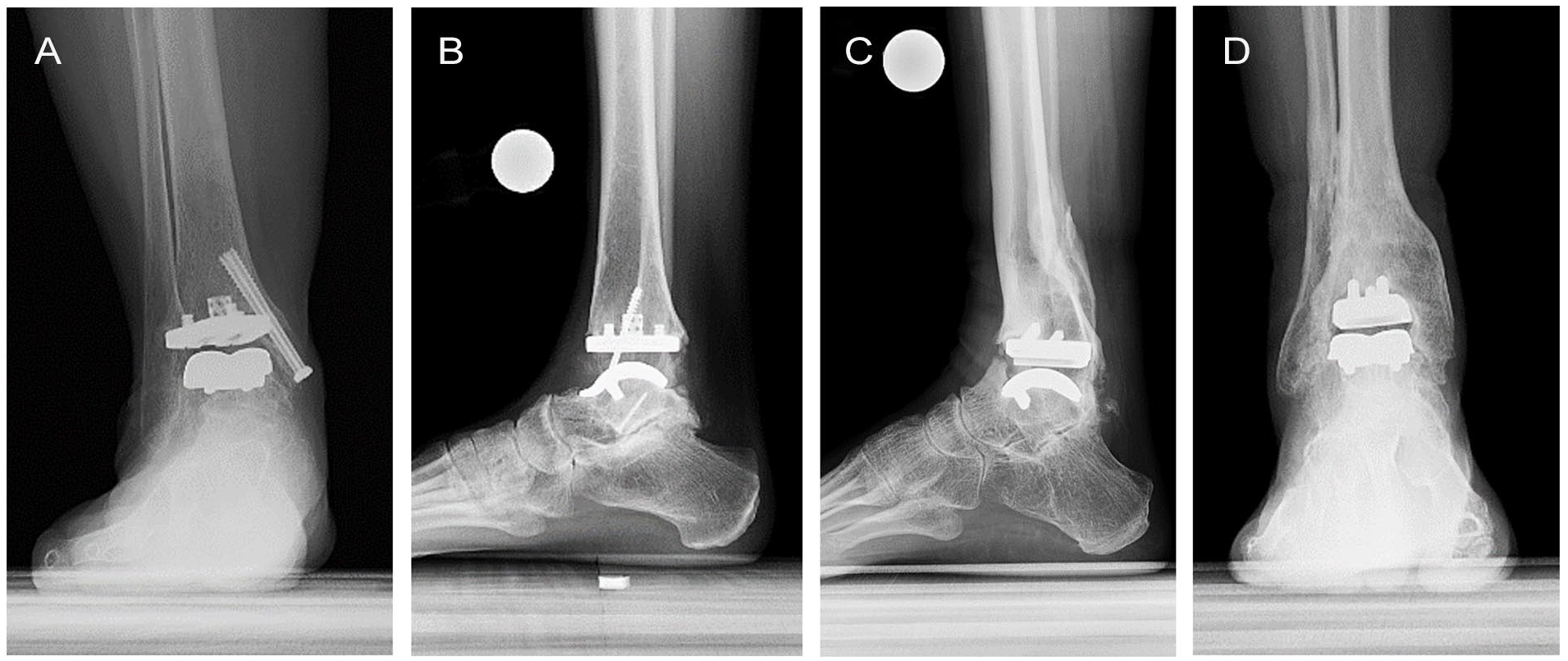
Representative images of radiographic complications including (A) tibial lucency, (B) periprosthetic cysts, and global tibial lucency in (C) lateral and (D) anterior-posterior views.
Patient-Reported Outcomes
PROMIS scores are reported in Table 4. Patients demonstrated clinically and statistically significant improvements in the domains of Physical Function (P = .002), Pain Interference (P = .007), and Pain Intensity (P = .010). At final follow-up, 65% of patients met PASS for the Physical Function domain, 71% met PASS for Pain Interference, 35% met PASS for Pain Intensity, 65% met PASS for Global Physical Health, 71% met PASS for Global Mental Health, and 50% met PASS for Depression.
PROMIS Outcomes and PASS Thresholds. a

Abbreviations: PASS, patient acceptable symptom state; PROMIS, Patient-Reported Outcomes Measurement Information System.
Parameters are reported as means ± SD (95% CI). Boldface indicates significance (P < .05).
Discussion
To our knowledge, this is the first study to report on the clinical, radiographic, and patient-reported outcomes of primary total ankle replacement in patients with prior distraction arthroplasty at minimum 2-years follow-up. Patients underwent TAR a mean 5.28 ± 3.52 years after distraction. This study included 19 ankles in 17 patients at an average follow-up of 4.4 years after TAR. There was good implant retention (95%) with significant improvements in PROMIS scores. Nevertheless, the cohort experienced a 21% reoperation rate and 37% radiographic complications, underscoring that prior distraction may predispose to a more complex postoperative course. The reoperation rate was in concordance with some other TAR studies.19,25
The overall revision rate of 5% found within this study was lower than hypothesized and may be in part due to the small sample size; however, this revision rate is comparable to previously published studies investigating short- to midterm outcomes of TAR. In a sample size of 731 primary TAR patients using any implant type, Henry et al 15 reported 33 revisions, a revision rate of 4.5%, at a mean 2.7 years of follow-up. Similarly, Saito et al 25 reported a revision rate of 4.7% in a retrospective analysis of 64 patients with a mean follow-up of 2 years. Over a longer follow-up period of 7 years, Cody et al 6 reported a comparable revision rate of 6.4%. Given the concordance of revision rates, there does not appear to be an increased risk of need for revision in the first 5 years in patients who undergo TAR following distraction arthroplasty.
The overall reoperation rate in this study was 21%; although no direct comparison group was used in this study, this reoperation rate was similar to other TAR studies with similar follow-up periods. In the aforementioned study, Saito et al 25 reported a reoperation rate of 17.1%; another midterm follow-up study of TAR using the Salto Talaris implant (N = 76) reported 16 reoperations for a reoperation rate of 21.1%. 19 Interestingly, 2 of 4 (50%) of the reoperations in our cohort were stiffness-related (flexor hallucis longus contracture and arthrofibrosis). 29 This relatively less common reason for reoperation supports anecdotal observations of increased stiffness in patients with prior distraction.
Radiographically, patients demonstrated clinically and statistically meaningful improvement in deformity correction following TAR, with average absolute coronal tibiotalar deformity decreasing from 5.07 ± 5.19 degrees to 1.14 ± 0.88 degrees at 2-year follow-up (P = .042). Radiographic complications such as lucencies, subsidence, and cysts were noted in 7 of 19 patients (37%), comparable to an assessment of TAR Infinity implants that reported a radiographic complication rate of 26.2%. 29
Although there were statistically significant improvements in PROMIS scores in multiple domains, patients demonstrated lower than expected rates of meeting PASS thresholds postoperatively in the PROMIS Pain Intensity domain. Although 69% of patients in our cohort achieved PASS for both Physical Function and Pain Intensity at 2-year follow-up, only 35% of patients achieved PASS for Pain Intensity at 2-year follow-up. The Pain Interference domain measures to what extent the patient’s ankle symptoms interfere with their physical activity and quality of life, while the Pain Intensity domain aims to measure severity of a patient’s ankle pain. In other words, 69% of patients found their level of physical function acceptable and that the interference their pain imposed on their desired activities was acceptable. However, only 35% of patients felt that the severity of their pain was acceptable. This discrepancy warrants further investigation and may indicate that patients may have higher expectations for physical function and are willing to tolerate more painful symptoms to return to a certain level of activity. More generally, the substantial difference in PASS achievement for the Pain Intensity domain compared to the other domains provides evidence that patients who undergo TAR following distraction arthroplasty are likely not fully satisfied with their symptoms following TAR surgery. Attention to patient education may be necessary to manage expectations. Nevertheless, meaningful improvements in PROs still support the utility of TAR to relieve ankle OA symptoms in patients with a history of distraction arthroplasty.
Lower rates of satisfaction among prior distraction TAR patients may be attributed to a variety of factors, including younger age, posttraumatic arthritis etiology, and a history of ipsilateral foot and ankle surgery in addition to distraction. In this distraction cohort, 5 of 19 patients (26%) were younger than 55 years, a demographic previously reported to have worse PROs and increased rates of complications. 2 Additionally, younger patients are known to have higher expectations following surgery, and it may be more difficult to meet those expectations. 30 Furthermore, the arthritis etiology for 14 of 19 (74%) in this cohort of patients was posttraumatic because of fracture. One possibility for decreased patient satisfaction is that arthritis caused by trauma in the young patient, particularly when it occurs shortly after the traumatic event, may demonstrate a more sudden onset of symptoms compared with gradual or chronic conditions of instability or primary arthritis; thus, patients may have a different mindset toward increased pain intensity because of the proximity of their active, pain-free lifestyles before their traumatic event. Additionally, the majority of patients in this cohort had undergone prior foot and ankle surgeries in addition to distraction arthroplasty, confounding where the stiffness may be attributed to and implying an increased level of complexity that required more surgeries to properly treat. Including distraction, patients in this cohort had an average of 2.4 ± 1.2 ipsilateral foot and ankle surgeries prior to TAR, and all patients had at least 1 concomitant procedure at the time of external fixator application. Furthermore, 4 of the 5 patients who underwent additional surgeries after TAR had a history of ORIF. A history of orthopaedic surgery has been associated with lower rates of PASS achievement. 28 Patients with surgical history may develop more scar tissue and sequelae, resulting in diminishing returns after additional surgeries, including distraction arthroplasty and TAR. Because of extensive prior surgical history, this patient cohort is likely to be more surgically complex, thus reducing the utility of additional surgeries of distraction arthroplasty and TAR.22,26
There are several limitations within this study. First, the cohort of 19 ankles from 4 surgeons at a single center is underpowered for precise estimates and prevents meaningful multivariable analysis of complications, reoperations, and PASS attainment. Studies with a larger sample size and comparative control group are needed to better evaluate whether outcomes are worse in this cohort of patients compared with TAR patients without prior distraction arthroplasty. Additionally, given that most patients had prior foot and ankle surgery in addition to distraction arthroplasty prior to TAR and only 4 ankles required reoperation, it is difficult to determine causality given the complexity of the patients. Additional research on TAR following distraction arthroplasty is warranted to evaluate the unique needs of these patients before, during, and after TAR.
Conclusions
Patients who underwent TAR following ankle distraction arthroplasty had a 5% revision rate, 21% reoperation rate, and 37% radiographic complication rate at an average of 4.36 years’ follow-up. Patients demonstrated significant improvement in PROMIS scores. However, patients reported lower than expected rates of satisfaction in the PROMIS Pain Intensity domain following surgery, suggesting that despite acceptable levels of physical function, patients may still experience unacceptable levels of pain. Despite reoperation and revision rates similar for a TAR cohort, patients who undergo TAR following distraction may be at a greater risk for residual painful symptoms. Thus, using distraction arthroplasty in the context of delaying TAR may add to the complexity of this patient cohort; time between distraction arthroplasty and eventual TAR was highly variable. Although some patients received more than a decade of relief from ankle arthritis symptoms before requiring TAR, others underwent TAR 1 year later, demonstrating that distraction arthroplasty may have been ineffective and even compounded to the negative effects of prior surgical history on TAR results. Because of these unique challenges, more research is necessary to guide TAR surgical planning and treatment for ankle osteoarthritis following distraction arthroplasty.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251363917 – Supplemental material for Total Ankle Replacement Outcomes in Patients With Prior Distraction Arthroplasty
Supplemental material, sj-pdf-1-fao-10.1177_24730114251363917 for Total Ankle Replacement Outcomes in Patients With Prior Distraction Arthroplasty by Allison L. Boden, Kira Lu, Jensen K. Henry, Emily Teehan and Constantine A. Demetracopoulos in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
Ethical approval for this study was obtained from the Institutional Review Board (IRB #2020-2132).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jensen K. Henry, MD, reports disclosures related to manuscript from Exactech, Inc: paid consultant; Stryker: research support. Constantine A. Demetracopoulos, MD, reports disclosures related to manuscript from Exactech, Inc: intellectual property (IP) royalties; In2Bones: IP royalties; Wolters Kluwer Health–Lippincott Williams & Wilkins: publishing royalties and general disclosures from American Orthopaedic Foot & Ankle Society: board or committee member; Artelon: paid consultant; Arthrex: paid consultant; Enovis: paid consultant; HS2, LLC: stock or stock options; In2Bones: paid consultant; Responsive Arthroscopy: paid consultant; Restor3D: paid consultant; RTI Surgical: paid consultant; Simulate Technologies: paid consultant, paid presenter or speaker; Treace Medical: paid consultant, paid presenter or speaker; Stryker: research support. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.