
Abstract
Background:
The Achilles tendon is prone to rupture, particularly in middle-aged men, and chronic injuries are often due to missed diagnoses or inadequate treatment. While acute ruptures can be managed with primary repair, chronic cases with tendon gaps >3 cm require reconstruction. A minimally invasive technique using autologous semitendinosus and gracilis tendon grafts has previously shown favorable short-term outcomes. This study evaluates longer-term outcomes with a minimum 5-year follow-up.
Methods
This study analyzed 21 patients undergoing minimally invasive Achilles tendon reconstruction with autologous hamstring grafts, compared with 21 healthy controls. magnetic resonance imaging confirmed diagnoses, and surgeries (2016–2019) used the EndoButton system for graft stabilization. Assessments included Achilles tendon Total Rupture Score (ATRS) for patient-reported outcomes, EuroQoL–5 Dimensions, 5 Levels (EQ-5D-5L) for overall health, and visual analog scale (VAS) for pain and satisfaction. Functional tests measured dorsiflexion (lunge test), calf endurance (heel rise test), and muscle strength (single-leg hop test), comparing operated vs unoperated legs.
Results
ATRS and EQ-5D-5L Index improved from 2 to 5 years (P = .0136, P = .0396), although significance was lost after Bonferroni correction. Functional test results remained stable. The operated limb achieved >90% of the nonoperated side across tests. Compared with controls, patients reported lower EQ-5D-5L scores and greater pain (P < .05), but satisfaction remained high (VAS score 9/10). One retear occurred due to infection.
Conclusion
Minimally invasive Achilles tendon reconstruction using hamstring autografts results in sustained functional and subjective improvements at a minimum of 5 years postoperatively. Despite modest residual deficits compared with uninjured controls, high satisfaction and strong limb symmetry support the long-term efficacy of this approach. This study demonstrates that the functional and subjective results of patients after Achilles tendon reconstruction with hamstring graft remain stable and satisfactory at a minimum of 5 years postoperatively.
Level of Evidence:
Level III, retrospective cohort study.
Introduction
Even though the Achilles tendon is the biggest and most robust tendon in the human body, it is also one of the tendons that is most frequently damaged. Ruptures of the Achilles tendon are particularly common in middle-aged men who play sports occasionally.34,37 Despite the high frequency of Achilles tendon ruptures, up to 25% of acute injuries are misdiagnosed and manifest as a chronic condition.33,43
Men in their middle years who are sporadically active are more likely to experience a spontaneous rupture caused by Achilles tendinopathy, and these ruptures frequently happen without any warning signs or symptoms.14,17,38 If an Achilles tendon lesion is not treated for longer than 4 weeks, it is considered chronic.12,38 Although neglected spontaneous ruptures and inadequate repairs are major contributors to chronic Achilles tendon lesions, chronic midsubstance tendinopathy without rupture also represents a common pathologic entity. 14
Primary direct repairs have shown to be successful in acute situations, yet it is not applicable in chronic conditions with either a gap or severe lengthening of the tendon manifested by an increase in passive ankle dorsiflexion.11,21,28 More robust techniques with graft augmentation are usually recommended for such chronic circumstances, as recurrent rupture, large tendon defects (exceeding 3 cm), and significant degeneration of the tendon tissue. 31 In principle, by restoration of tendon tissue continuity it is anticipated to also restore full function of the operated limb.3,5,13 The optimal treatment for Achilles tendon re-rupture and rehabilitation protocol remains controversial among specialists in orthopaedics, sports medicine, and physiotherapy. 42 Many robust reconstructive techniques have been described before.26,29,41,49 One of the major issues remains high risk of postoperative complications, mostly infection or problems with tissue healing. Therefore, a novel technique has been developed in our institution using a minimally invasive approach with an autologous semitendinosus and gracilis tendon graft. 39 Furthermore, we have described the specific rehabilitation protocol after this procedure. 24
In 2022, we published an article describing the results of a group of 30 patients after the aforementioned procedure, with 1-year and 2-year follow-up. We showed satisfactory functional outcomes as well as a good rate of return to normal physical activity in this cohort. However, we decided to follow these patients for a longer period because we included, on one hand, young participants <30 years of age, and on the other hand, those >50 years of age. 23 Thus, the functional requirements and biological status might be completely different among the members of the cohort.
The study aimed to evaluate the long-term effects of Achilles tendon reconstruction (ATR) using a minimally invasive technique using autologous semitendinosus and gracilis tendon grafts based on functional and subjective parameters, with a follow-up of at least 5 years. The specific aims were to assess the long-term persistence of outcomes observed at the 2-year follow-up (ie, at 5 years), to compare these outcomes with those of age-matched healthy controls, and to evaluate potential differences in functional parameters between the affected and contralateral, non-involved limb.
Materials and Methods
Study Design and Patient Characteristics
This is the prospective evaluation of the study group that were previously followed for 2 years after minimally invasive reconstruction of the Achilles tendon with autologous semitendinosus (ST) and gracilis (GR) tendon grafts. 23 From 30 patients included at baseline, 21 responded at 2 and 5 years. Of the 9 patients lost to follow-up, 1 relocated to another country, 5 declined to participate in the evaluation due to personal reasons, and 3 could not be contacted because of incorrect contact information. Therefore, 21 patients after the aforementioned procedure (ATR group) and 21 healthy individuals (control group) with no history of injury or surgery in the lower limb were included in the study. 23 Both groups were matched for sex, age, and physical activity level. None of the participants were competitive athletes. The maximum tolerated level of physical activity, as assessed by the Tegner Activity Scale, was 6. All patients in the ATR group were required to attend the follow-up clinical and functional evaluation in person.
The inclusion and exclusion criteria are described in detail in our previous study and presented in Table 1. The diagnosis of Achilles tendon injury was based on magnetic resonance imaging.
Inclusion and Exclusion Criteria of the Study Group.

Abbreviation: MRI, magnetic resonance imaging.
Surgical Procedure
Two trained orthopaedic surgeons (P.B. and T.P.) performed surgical procedures between 2016 and 2019 at Rehasport Clinic in Poznań. The entire intervention group underwent minimally invasive Achilles tendon reconstruction using hamstring autografts. Posterolateral and posteromedial portals were made 3 cm above the calcaneus to clean the tendon endoscopically. Hamstrings were harvested and prepared for the EndoButton system. A midline skin incision was made near the calcaneus, followed by Kirschner-wire drilling under fluoroscopy. The graft with an EndoButton loop was inserted into the drilled tunnel. Eight consecutive skin incisions were made, and the graft ends were brought through the native Achilles tendon and tied at the proximal incision. This technique enables Achilles tendon reconstruction with semitendinosus and gracilis tendons, offering a salvage option in resistant cases. A full description of the procedure has been published. 39
The protocol, according to which the rehabilitation of all patients was carried out, was created based on our team’s many years of experience and available scientific evidence. The protocol is divided into specific stages, of which only the first 3 are limited by time guidelines. Functional guidelines cover the subsequent stages. Rehabilitation with a therapist takes place once a week, and during the remaining time, the patient performs the assigned exercises in the home environment. The beginning of the dynamic work stage by the patient and the end of the entire rehabilitation process is covered by a functional assessment performed by a physiotherapist. The full description of the rehabilitation protocol was published in our previous study. 24
Subjective Assessment
The results of the following questionnaires were compared between the ATR group and the healthy control group. ATRS is a patient-reported instrument that has shown high reliability, validity, and sensitivity for measuring outcomes after treatment in patients with a total Achilles tendon rupture. 22 This questionnaire focuses on the patient’s perception of his or her health status, which should be considered the most important indicator of treatment success. Moreover, it determines the patient’s level of satisfaction with the outcome of the applied treatment and his return to activities of daily living from before the injury. The ATRS score ranges from 0 to 100 points, with higher scores indicating better outcomes. The minimal clinically important difference (MCID) is 10 points, corresponding to 10% of the total score.35,42
The EuroQoL–5 Dimensions, 5 Levels (EQ-5D-5L) health questionnaire assesses overall health status, encompassing functional abilities, physical symptoms, and emotional aspects that are pertinent even for those who are healthy. The EQ-5D-5L is a more sensitive 5-level adaptation of the original 3-level version (EQ-5D-3L).16,19 Norms for the Polish population for the EQ-5D-5L have already been established. 15 The first part of the EQ-5D-5L questionnaire consists of 5 items assessing mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Based on these responses, an index score is calculated, ranging from −0.285 to 1.0, where 1.0 represents optimal health. The second component is the “Health Today” assessment, measured using a visual analog scale (VAS), with scores ranging from 0 to 100. The MCID for the EQ-5D-5L index varies across populations and has been reported to range from 0.017 to 0.098.4,48 For the VAS component, the MCID has been estimated between 7.5 and 8.0 points. 20
VAS was also used for evaluation of pain and satisfaction with the outcome of treatment. The MCID for the VAS has been reported to range from 1.8 to 5.2 points following foot and ankle surgery. 25
Functional Assessment
Functional test results were compared within the ATR group by assessing the operated limb against the nonoperated limb. The ratio between the operated and nonoperated sides was calculated using the Limb Symmetry Index (LSI). The functional evaluation was performed by a trained physiotherapist (B.K.) and was based on 3 objective tests: the weightbearing lunge test, the heel rise test, and single leg hop test. All tests were performed for each limb separately, following the existing protocols. 23 The weightbearing lunge test measures the extent of dorsiflexion of the ankle joint and foot complex. 27 The heel rise test gives information about the endurance of the calf muscle. 36 The single leg hop test is a performance-based measure used to assess the combination of muscle strength, neuromuscular control, confidence in the limb, and the ability to tolerate loads related to sports-specific activities.2,36,40
Statistical Analysis
All statistical analyses were performed using TIBCO Software Inc (2017) Statistica, version 13. The significance level for all tests was set at P < .05. Descriptive statistics, including median, SD, and range (minimum and maximum values), were used to summarize the analyzed variables.
The normality of data distribution was assessed using the Shapiro-Wilk test. As none of the examined variable pairs followed a normal distribution, nonparametric tests were applied for hypothesis testing.
To evaluate differences in mean values between 2 independent groups (study vs control), the Mann-Whitney U test was used. To assess differences between time points (2-year vs 5-year follow-up) and between limbs (operated vs nonoperated), the Wilcoxon signed-rank test was applied. In addition, Bonferroni correction was used for multiple comparisons between time points to control for Type I error (false rejection of the null hypothesis).
To analyze the relationships between variables, the Spearman rank correlation coefficient was used.
Results
Characteristics of the Study Groups
Demographic data of both groups included in the study are presented in Table 2. Average follow up time was 72.8 (minimum 60–maximum 96) months. Both groups consisted of 21 men.
Demographic Data. a
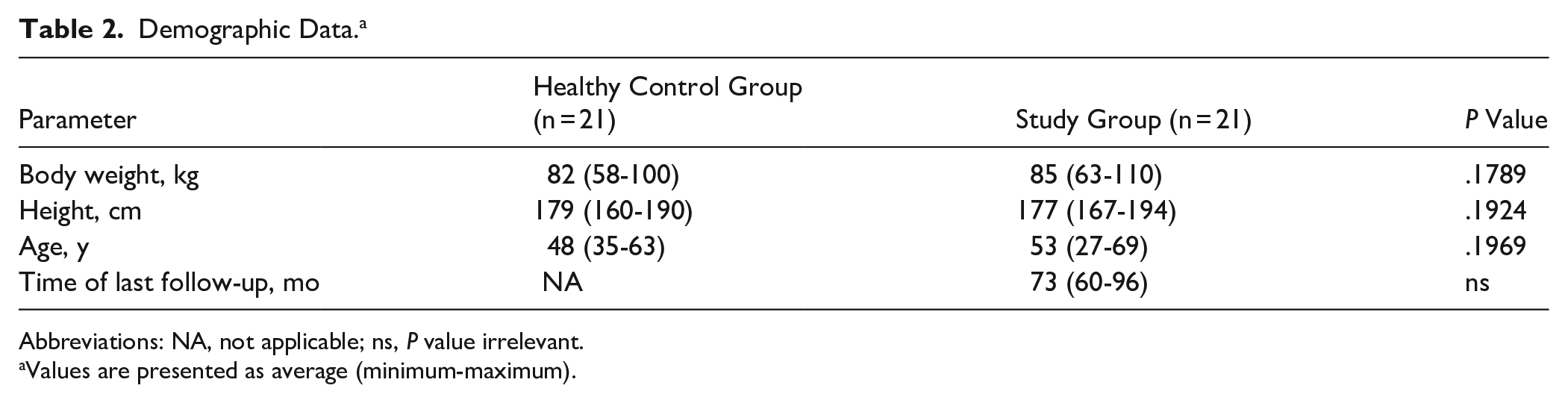
Abbreviations: NA, not applicable; ns, P value irrelevant.
Values are presented as average (minimum-maximum).
Comparison of the Results of Patients 2 and Minimum 5 Years After the Procedure
The results of the ATRS and EQ-5D-5L Index significantly improved after 5 years in comparison to 2-year follow-up (P = .0136, P = .0396, respectively); however, the difference in ATRS was clinically insignificant. We observed an insignificant decrease in EQ-5D-5L Health Today category and a deterioration by 1 point in pain and satisfaction with the outcome of the applied treatment (Table 3). A post hoc power analysis was performed for parameters that initially demonstrated statistically significant differences between time points (Table 3). The analysis revealed adequate statistical power for the ATRS parameter (power = 0.84). In the case of the EQ-5D-5L Index, power could not be estimated because of the absence of SD and correlation data. Following the application of the Bonferroni correction (adjusted significance level α = 0.01), the differences in both parameters no longer reached statistical significance.
Comparison of the Results of Patients’ Subjective Evaluation 2 and 5 Years After the Procedure (n = 21). a
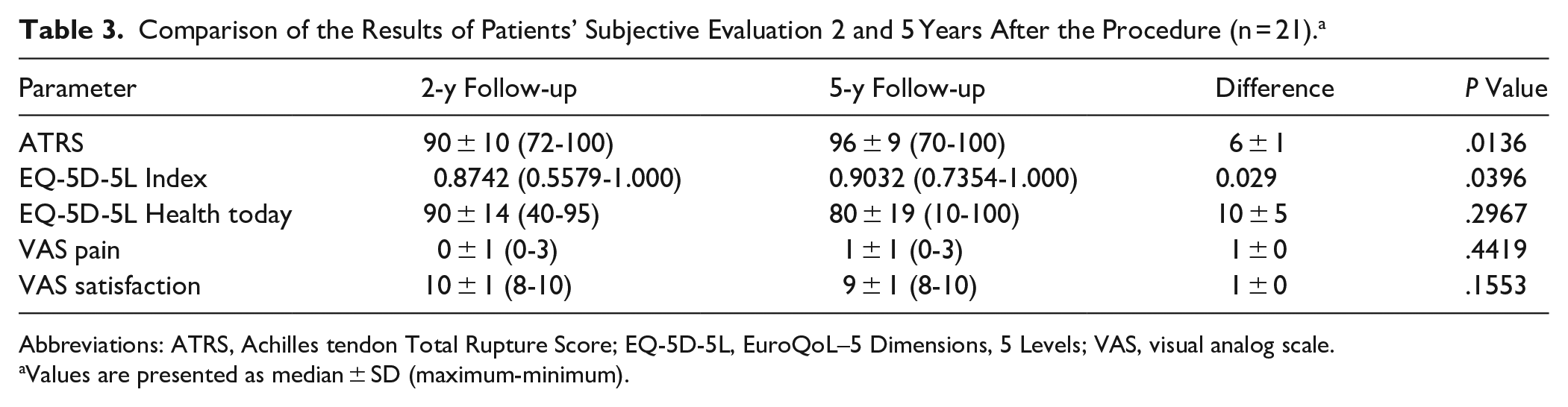
Abbreviations: ATRS, Achilles tendon Total Rupture Score; EQ-5D-5L, EuroQoL–5 Dimensions, 5 Levels; VAS, visual analog scale.
Values are presented as median ± SD (maximum-minimum).
The results obtained in functional tests are presented in Table 4.
Comparison of the Results of Functional Tests 2 and 5 Years After the Procedure (n = 21). a

Values are presented as median ± SD (maximum-minimum).
No change of 1 repetition in the heel rise test, maintenance of the dorsal flexion range of motion measured with the weightbearing lunge test, and a 4-cm decrease in the single-leg hop test of the operated leg can be observed in the 5-year follow-up. Those changes were statistically insignificant.
None of the tests in Table 6 are statistically significant when comparing 24 months to extended follow-up.
Comparison of the Results of Patients Treated Surgically and Healthy Control Group
The subjective outcomes reported by patients are gathered in Table 5 and Figure 1. There is a statistically significant difference in ATRS, EQ-5D-5L Index, EQ-5D-5L health today, and VAS pain between the control and study groups (P = .0144; P = .0014, P = .0006; P = .0242). The differences in EQ-5D-5L Index and EQ-5D-5L health today reached the level of MCID. In the control group, the mentioned parameters are statistically significantly better. In the satisfaction survey with the procedure, five years after the procedure, patients reported an average score of 9 on the VAS scale. Table 5 shows comparisons between groups, Bonferroni correction was not applied.
Subjective Evaluation of the Outcomes of the Applied Treatment.

Abbreviations: ATRS, Achilles tendon Total Rupture Score; EQ-5D-5L, EuroQoL–5 Dimensions, 5 Levels; VAS, visual analog scale.
Values are presented as median ± SD (maximum-minimum).

Box plot diagrams showing the distributions of the ATRS, EQ-5D-5L, Health Today, and VAS pain questionnaire parameters. Central lines represent the medians, boxes indicate the range from 25th to 75th percentile, whiskers indicate minimal and maximal values. *Statistically significant difference (P < .05). ATRS, Achilles tendon Total Rupture Score; EQ-5D-5L, EuroQoL–5 Dimensions, 5 Levels; VAS, visual analog scale.
Comparison of the Results Between Affected and Unaffected Side
The functional outcomes reported by patients after 5 years after the surgical treatment are gathered in Table 6 and Figure 2. There is a statistically significant difference in all functional tests (the weightbearing lunge test, the heel rise test, and the single leg hop test) between the operated and nonoperated limbs in favor of nonoperated side. Following the application of the Bonferroni correction (adjusted significance level α = 0.01), the differences in both parameters remained statistically significant. However, despite statistical significance, in all functional tests the operated leg achieved a result higher than 90% of the LSI of the healthy leg.
Results of the Functional Tests in the Study Group (n = 21).

Values are presented as median ± SD (maximum-minimum).

Box plot diagrams showing the distributions of the weightbearing lunge test, heel rise test, and single-leg hop parameters. Central lines represent the medians, boxes indicate the range from 25th to 75th percentile, whiskers indicate minimal and maximal values.
Correlations
No strong correlations were observed between tests, analyzed on a peer-to-peer basis, between groups, and within groups. All of the statistically significant correlations were weak: VAS pain vs VAS satisfaction, r = −0.41(indicating that lower pain levels are associated with higher patient satisfaction); ATRS vs VAS pain, r = −0.46 (indicating that lower ATRS scores are associated with higher reported pain); ATRS vs EQ-5D-5L index, r = −0.56.
Discussion
This study demonstrates that the functional and subjective outcomes remain stable and satisfactory at a minimum 5-year follow-up following Achilles tendon reconstruction with a hamstring graft. Furthermore, the cohort showed a low pain level and very high satisfaction with the outcome of the applied treatment despite existing differences in functional tests and self-evaluation questionnaires regarding the nonoperated side and control group, respectively.
Treatment of neglected or chronic Achilles tendon ruptures is very challenging for the patient, physician, and physiotherapist. Our results showed that, in this case, all 3 parties might be satisfied with the long-term outcomes of the surgery. The subjective evaluation of Achilles tendon function in the ATRS significantly improved after 5 years compared with the results collected after 2 years. Moreover, patient satisfaction remained in the same range on the VAS scale (from 8 to 10). From the surgeon’s point of view, a very important factor is the retear rate after tendon reconstruction. There was no retear of the reconstructed or augmented Achilles tendon in our cohort. Physiotherapists’ main concern during the rehabilitation process, as well as in the long term, is the function of patients as measured objectively with specific and tailored performance-based tests. We showed that participants did not deteriorate in any test between the 2 analyzed follow-ups.
Limb symmetry regarding ankle range of motion, calf muscle strength, and neuromuscular control is a common goal of the rehabilitation process. It is required for a safe return to physical activity after injury but also for reducing the risk of reinjury.30,47 The LSI is the ratio of both sides—operated and nonoperated. It is widely used in the decision-making process in physiotherapy and returning to sport after various musculoskeletal injuries.30,47 An LSI of 90% is a minimal level that allows the physician to give “the green light” for full participation in professional and recreational sports.30,46,47 Therefore, we can conclude that differences observed in functional tests in our study give an opportunity to return to sporting activities, as they did not exceed 10%. The use of LSI seems appropriate in examining patients after Achilles tendon reconstruction to assess the functions of the operated area and the level of restored fitness. However, this requires further research using it in the specific cases of Achilles tendon injury.
We encountered difficulties comparing heel raise test results with population norms because of inconsistent testing methods in the literature. Studies use different surfaces, angles, and leg positions, making comparisons impossible. The group studied in our article during the extended follow-up achieved results at the level of 12 ± 5 (2-22) on a 30-degree elevation. We chose to perform this test in this manner to make it even more complex. Thanks to the slope, we assessed the strength of the calf muscle throughout its full range of motion, which constitutes the biggest advantage. Analyzing the results from the work presenting a large meta-analysis of the heel raise tests in healthy people, we found 3 studies that conducted this test on a 10-degree slope.7,14,32 In all of them, the age groups did not fit our study group’s average age. The mean age of participants was 28, 36, and 72 years. In 2 studies, the results were better than ours (32 SD and 33 SD heel raises), but the included patients were much younger. The worst results were reported in the oldest cohort (10 SD heel raises).9,18,44 The study by Chitre and Prabhu 10 from 2017, which included healthy participants similar in age to ours and with no previous ankle joint injuries, showed relatively inferior results on the heel raise test on a flat surface (14.5 ± 5.31 [6-23]). In our opinion, this test, performed in this manner, is much less demanding for the participant. Nevertheless, it indicates that the strength level of the calf muscles in patients who underwent Achilles tendon reconstruction with a hamstring graft after 5 years is at a high, satisfactory level.7,10
Comparing the results of the study group in the EQ-5D-5L Index (mean 0.9032) with the normative data of the Polish population in the most similar age group (45-54) (mean 0.947), we noticed a very small difference of 0.0438. 15 It is important to note that each of the questions in the survey has a different value that contributes to the final result. Therefore, comparing the result itself is a rather simplified conclusion. This small difference could still have significant implications for patient outcomes and treatment effectiveness.1,8,45
Furthermore, we observed insignificant difference in the EQ-5D-5L index between treated patients and controls. On the other hand, the control group had substantially better result in EQ-5D-5L Health Today than our cohort after a 5-year follow-up.
The results in the EQ-5D-5L index remained at the same high level after 5 years from the Achilles tendon reconstruction using a hamstring graft. However, EQ-5D-5L Health Today deteriorated significantly over time. In our opinion, this may be attributed to the aging of the included patients. The last evaluation was performed between 3 and 5 years after the previous examination, which took place 24 months after the procedure.
There are studies presenting the use of various methods of tendon reconstruction with a double-bundle flexor hallucis longus tendon, V-Y tendon plasty, peroneus brevis transfer, or gastrocnemius flaps, but nevertheless the goal remains the same—restoration of proper function.26,29,41,49 Studies published in 2019 by Lin et al 29 and 2021 by Zou et al 49 reported excellent outcomes at an average follow-up of 31 and 32 months, respectively, following treatment of chronic Achilles tendon ruptures using V-Y tendon plasty and double-bundle flexor hallucis longus (FHL) transfer. The cited authors based their works on the results of the ATRS, the American Orthopaedic Foot & Ankle Society score (AOFAS), the Victorian Institute of Sports Assessment-Achilles score. Patients were able to return to daily life activity levels without restrictions. At the latest follow-up, all patients were able to perform repetitive single heel rise on the involved limb, and to walk without a visible limping. All of the postoperative magnetic resonance images showed the continuity of the Achilles tendon with no signs of cysts or inflammation, indicating perfect healing at the final follow-up.29,49
Song et al 41 in their study from 2020 show a significant improvement in the ATRS and AOFAS scores after Achilles tendon reconstruction using a semitendinosus muscle graft with the 4-year follow-up. The median AOFAS score in their study increased from 50 (5-75) to 100 (86-100), and the median ATRS score increased from 22.5 (6-67) to 99 (84-100).
Two studies with long-term follow-ups (143.5 months and 164 months) present excellent results of functional assessment and PROMS completed by the patients. They included in their testing protocol isokinetic strength measurement, AOFAS questionnaire, ankle range of motion, calf circumference, heel raise test, and visual analog scale (VAS) score. This work also relies on various methods of Achilles tendon reconstruction.26,41
In a long-term observation (72.8 months), our study group obtained 96 SD points in the ATRS. In our view, this is an excellent result, comparable to those presented in the aforementioned studies.
Furthermore, the most recent systematic review to date 32 that analyzed the outcomes of treatment for chronic Achilles tendon ruptures with different free grafts shows that probably the most suitable option for this procedure is the ipsilateral semitendinosus tendon autograft. It is associated with a relatively low rate of complications, especially when performed endoscopically, and allows for a return to physical activity prior to the injury. These conclusions confirm our observations and highlight that the method used by our team was suitable for these patients.
Our team’s rehabilitation protocol allows for quick removal of elbow crutches and movement without a brace. This is an essential aspect for elderly and obese people who find it very difficult to move with crutches. This approach is supported by our previous biomechanical study, which showed that the strength of the reconstructed Achilles tendon suture alone is approximately 400 N. 8 Patients may safely load the area, knowing the forces acting on the Achilles tendon during everyday activities do not exceed the aforementioned threshold. 6
The most vital point of our study is the long period of patient observation and the use of a combination of subjective, validated questionnaires and functional tests that gave us a bigger picture of patient’s state at follow-up time.
Limitations
The primary limitation of this study is the small sample size, which reflects the fact that this procedure is not a first-line treatment in clinical practice, thereby limiting patient availability. Additionally, the study population consisted exclusively of male subjects, which restricts the generalizability of the findings. The absence of preoperative data limits interpretation of the magnitude of recovery. Future investigations should incorporate isokinetic assessments of triceps surae strength and endurance, as well as plyometric testing (eg, platform jump tests), particularly in the context of long-term follow-up. A key statistical limitation is the loss of statistical significance for ATRS and EQ-5D-5L Index after Bonferroni correction. Moreover, the inability to calculate power for EQ-5D-5L due to missing data limits result interpretation. These findings should therefore be interpreted with caution.
Conclusion
Surgical reconstruction of the Achilles tendon using autologous semitendinosus and gracilis grafts leads to sustained improvements in patient-reported outcomes a minimum follow-up of 5 years. Functional performance remained stable, with the operated limb reaching more than 90% symmetry versus the nonoperated side. Although patients reported more pain and lower general health scores than healthy controls, overall function and satisfaction remained high, supporting the long-term effectiveness of the procedure.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251363880 – Supplemental material for Minimum 5-Year Outcomes After Minimally Invasive Achilles Tendon Reconstruction Using Autologous Hamstring Grafts
Supplemental material, sj-pdf-1-fao-10.1177_24730114251363880 for Minimum 5-Year Outcomes After Minimally Invasive Achilles Tendon Reconstruction Using Autologous Hamstring Grafts by Bartosz Kiedrowski, Jakub Kaszyński and Tomasz Piontek in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Bioethics Committee of the Medical University of Poznan by resolution No. 743/20. Informed consent was obtained from all participants in the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.