
Abstract
Background:
An accessory navicular is a supernumerary ossicle located medial to the navicular bone, typically within the substance or insertion of the posterior tibial tendon, and can be a source of pain and dysfunction in active individuals.
Methods:
This was a retrospective comparative study evaluating the outcomes of the modified Kidner procedure in athletes (ballet, basketball, volleyball, running, football, soccer, etc) and nonathletes. Our study included 42 consecutive feet that were operatively managed with the modified Kidner procedure for a symptomatic accessory navicular between the years 2014 and 2023. Patients who underwent any other procedure in addition to the modified Kidner procedure were excluded from the study. The objective of this study is to determine the outcomes of the modified Kidner procedure for an accessory navicular in the athletic population compared to the nonathletic or general population.
Results:
Athletes had no difference in postoperative Foot and Ankle Ability Measure (FAAM) activities of daily living (ADL) and visual analog scale (VAS) scores compared with nonathletes. Interestingly, comparison of single-sport to multisport athletes revealed that single-sport athletes presented with worse preoperative VAS and FAAM scores. However, there was no significant difference in postoperative patient-reported outcomes between single-sport and multisport athletes.
Conclusion:
Our results suggest that although single-sport athletes may present with more severe preoperative symptoms, they experience comparable improvement following operative management relative to nonathletes or multisport athletes
Level of Evidence:
Level III, retrospective comparative study.
Introduction
An accessory navicular is an extra bony growth that may be seen near the navicular bone on the medial aspect of the foot. The presence of an accessory navicular (AN) may be the source of debilitating pain and diminished physical activity in young active patients. Pain may arise due to contact of the shoeware on the accessory navicular, exacerbating symptoms during moments of high physical demand (physical activity, trauma, etc). 1 This hinders the physical function of athletes in their daily lives and sports-related activities. Similarly, Pretell-Mazzini et al 2 reported that 85% of patients with AN had pain during physical activity, and almost half of the cohort was unable to participate in physical activities. Excision of the accessory navicular and advancement of the posterior tibial tendon has been shown to provide significant relief of pain and improved function for individuals who have failed to improve with conservative management.1,3 -5
Prior data have shown that athletes with AN are less likely to improve from conservative management; however, there is limited data on whether athletes are more likely to benefit from operative management compared with nonathletes. 1 Additionally, there is a scarcity of data evaluating patients with AN within the US population. The objective of this study is to determine the outcomes of the modified Kidner procedure for an accessory navicular in the athletic population compared with the nonathletic or general population. We hypothesized that athletes would have worse patient-reported outcomes compared to nonathletes.
Methods
This was a retrospective comparative study evaluating the outcomes of the modified Kidner procedure in athletes and nonathletes. Athletes were determined based on patient self-identification (documentation in the electronic medical record) and participation in at least 1 sport (ballet, basketball, football, soccer, hockey, volleyball, etc). Of these, the level of athletic activity was reported for a total of 20 patients and designated as follows: 8 recreational, 1 collegiate, 7 high school, 3 competitive, and 1 elementary school. The other 22 patients had no documentation of the level of athletic activity in the electronic medical record. The diagnosis of accessory navicular was confirmed radiographically by the senior surgeon. Patients between the ages of 10 and 37 years presenting with symptomatic accessory navicular and managed with the modified Kidner procedure were included in this study. Forty-two feet with a symptomatic accessory navicular that met the inclusion criteria were included for analysis in this study. Patients were matched in a 1:1 ratio for age. Exclusion criteria were as follows: (1) patient with asymptomatic accessory navicular, (2) history of additional procedure on the same foot or ankle, (3) <6 months follow-up, or (4) undergoing any other procedure besides the modified Kidner procedure (eg, flexor digitorum longus transfer, Evan osteotomy, Cotton osteotomy, calcaneal osteotomy, gastrocnemius resection, tarsometatarsal arthrodesis, subtalar arthrodesis, talonavicular arthrodesis, etc) (Figure 1).

Flowchart of cohort identification, inclusion and exclusion criteria.
A trial of conservative management (orthotics, anti-inflammatory medications, and shoe modification) was attempted for all patients. Operative management was considered for those who endorsed persistent pain despite conservative management. In brief, operativemanagement was carried out through the following steps. (1) Using a No. 15 blade, an incision centered over the posterior tibial tendon insertion on the navicular was made. (2) After exposure of the posterior tibial tendon, the area of the accessory navicular was identified and excised en-bloc with sharp dissection or using a high-speed burr (mainly for for III variants). (3) A portion of the posterior tibial tendon insertion was released, tubularized, and advanced back to its insertion using a 3.0 Arthrex Bio-SutureTak anchor (Arthrex, Naples, FL). Postoperative protocol was directed as follows: nonweightbearing for 6 weeks, with the initial 2 weeks in a short leg splint. After 2 weeks, patients are transitioned to a short leg cast in slight inversion.
In our cohort, 19.4% were found to have type I accessory navicular, whereas 64.5% of individuals had type II, and 16.1% of individuals were found to have type III accessory navicular (Figures 2, 3, and 4). There were no associations between the type of accessory navicular and outcomes (P > .05). Average preoperative calcaneal inclination was 18.17 ± 0.98 degrees, 18.50 ± 6.70 degrees, and 15.25 ± 4.03 degrees for type I, II, and III AN, respectively (overall average of 17.88 ± 5.40 degrees). No association was found between preoperative calcaneal inclination angle and postoperative visual analog scale (VAS), Foot and Ankle Ability Measure (FAAM) activities of daily living (ADL), or FAAM sports subscale scores (P > .05). All patients were operatively managed with the modified Kidner procedure for symptomatic accessory navicular between 2014 and 2023 and were followed for an average of 4.10 ± 3.26 years. Demographic information, including age, sex, and body mass index (BMI), was collected using the electronic medical record. Outcome variables such as the VAS, FAAM ADL, and FAAM sports scores were also collected. Additional information, including rates of subsequent procedures after surgical management, was also included.

Type I accessory navicular marking by the accessory bone within the posterior tibial tendon insertion.

Type II accessory navicular representing an accessory bone attached to the navicular via cartilage.

Type III accessory navicular representing a fused accessory ossicle.
Statistical Analysis
IBM SPSS version 27.0 (IBM Corp, Armonk, NY) was used for the statistical analyses. Assessment of normality for continuous data was carried out using the Shapiro-Wilk test. All continuous values were found to be normally distributed except postoperative VAS score (P = .03). Independent samples t test, analysis of variance, χ2, and Fisher exact test were performed for data analysis. Multivariate analysis was carried out using analysis of covariance, comparing athletes and nonathletes with BMI as a covariate.
Results
Demographics and Preoperative Presentation
There were no differences in average age at the time of surgical management between athletes and nonathletes (Table 1). There were no significant differences in preoperative VAS or FAAM ADL scores. All other demographic comparisons found no difference (Table 1).
Demographics and Preoperative Presentation of Athletes Compared to Nonathletes. a

Abbreviations: ADL, activities of daily living subscale; BMI, body mass index; FAAM, Foot and Ankle Ability Measure; VAS, visual analog scale.
Unless otherwise noted, values are presented as mean ± SD
Athletes and nonathletes had no difference in postoperative outcomes (P > .05). We also found that athletes and nonathletes had no difference in postoperative FAAM ADL scores (Table 2). Other comparisons evaluating the postoperative outcomes and rates of subsequent surgery found no significant difference between these 2 groups (Table 2). Covariate adjustment for continuous outcomes was conducted with BMI as a covariate. Similar to prior analyses, we found no differences in preoperative and postoperative VAS and FAAM ADL among athletes and nonathletes. Coefficient β represents the respective change in outcomes for nonathletes and athletes. Interestingly, after adjusting for BMI, we found that on average, athletes had slightly lower postoperative FAAM ADL scores compared with nonathletes (Table 3). However, this difference was not statistically significant (P = .8).
Outcomes of the Modified Kidner Procedure in Athletes and Nonathletes.
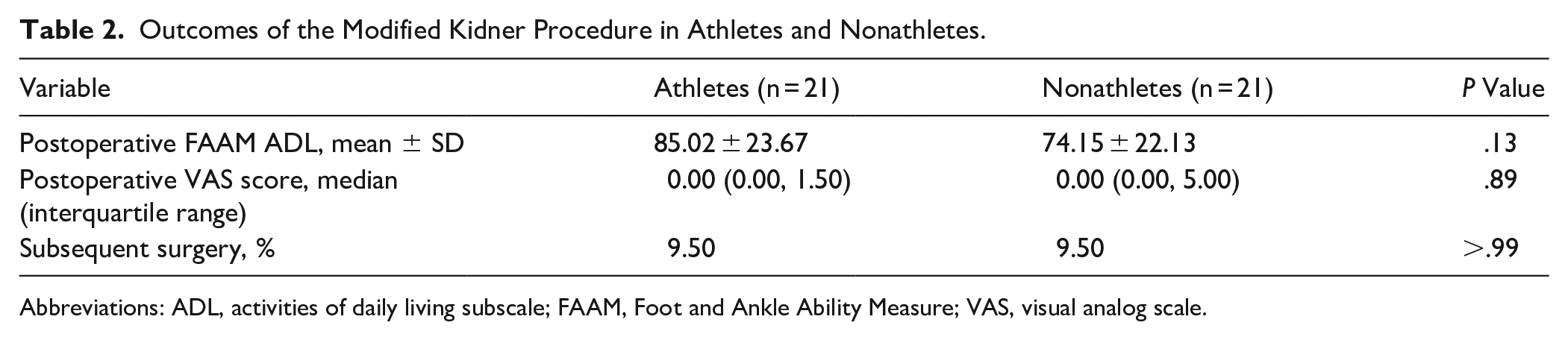
Abbreviations: ADL, activities of daily living subscale; FAAM, Foot and Ankle Ability Measure; VAS, visual analog scale.
Multivariate Analysis of Outcomes Between Athletes and Nonathletes. a

Abbreviations: ADL, activities of daily living subscale; FAAM, Foot and Ankle Ability Measure; VAS, visual analog scale.
Values reported are estimated marginal means, which have been adjusted for BMI as a covariate. Coefficient (β) represents the relationship between predictor/grouping variables and outcomes
A total of 4 feet had subsequent surgery for persistent pain or regrowth of AN: 2 recreational dancers and 2 nonathletes (95% CI −0.04, 0.23). One recreational dancer underwent subsequent surgery for flatfoot correction with flexor digitorum longus transfer, and calcaneal osteotomy. The others underwent subsequent surgery for regrowth or persistent pain.
Paired Analysis Evaluating Pre- and Postoperative Outcomes of the Modified Kidner Procedure
Paired analysis of the pre- and postoperative outcomes of our entire cohort showed that the modified Kidner procedure significantly reduced VAS scores in patients with AN (5.47 ± 2.20 vs 1.73 ± 2.73, P < .001) (Table 4). The modified Kidner procedure was also found to significantly improve the postoperative FAAM ADL score (57.41 ± 20.40 vs 83.36 ± 20.54) (Table 4). FAAM Sports score among athletes similarly improved post-operatively (Table 4).
Outcomes of the Modified Kidner Procedure Using a Paired Analysis.

Abbreviations: ADL, activities of daily living subscale; FAAM, Foot and Ankle Ability Measure; VAS, visual analog scale.
Boldface indicates statistical significance, P < .05.
FAAM sports scale only describes the athletes within our study population.
Subgroup Analysis of Outcomes in Single vs Multisport Athletes
Subgroup analysis of outcomes comparing single-sport to multisport athletes shows that self-described single-sport athletes, on average, presented with worse VAS and FAAM ADL scores than multisport athletes. However, both self-described single-sport and multisport athletes showed no difference in pain and FAAM ADL scores, with an average follow-up of 3.47 ± 2.56 years for single-sport athletes and 4.72 ± 3.53 years for multisport athletes (Table 5).
Outcomes of the Modified Kidner Procedure in Self-Reported Single vs Multisport Athletes. a

Abbreviations: ADL, activities of daily living subscale; FAAM, Foot and Ankle Ability Measure; VAS, visual analog scale.
Unless otherwise noted, values represented as mean ± SD.
Boldface indicates statistical significance, P < .05.
Discussion
Young active patients with an accessory navicular are more likely to experience pain during physical activity, which limits their ability to participate in sports activities.1,6 In the current study, athletes and nonathletes had similar rates of subsequent surgery, pain, and performance of activities of daily living relating to the foot and ankle compared with nonathletes (Table 2). Interestingly, we found that single-sport athletes had worse preoperative VAS and FAAM ADL scores but no difference in outcomes after surgical management. (Table 5). In a retrospective comparative study, Jegal et al 1 evaluated a cohort of 31 athletes and 33 nonathletes. At 1-year follow-up, the authors found that athletes had greater patient-reported outcomes compared with nonathletes (AOFAS, 93.3 ± 5.3 vs 89.0 ± 7.0, P = .009). Similar to our current study, the authors found no difference in preoperative pain between athletes and nonathletes. However, the authors reported a greater incidence of bone marrow edema on the navicular bone among athletes compared to nonathletes (27/30 vs 16/27, P = .012). The presence of bone marrow edema may not be associated with pain; however, we could indicate that athletes had worse mechanical irritation or injury to the accessory navicular bone.
A subgroup analysis between our athletic populations (Table 5) found that at clinical presentation, self-described single-sport athletes had worse VAS and FAAM scores than multisport athletes. This result is likely due to the excessive load/strain on a specific portion of the body.
Prior studies have shown that single-sport athletes are at an increased risk of overuse injuries, especially in the lower extremities.7 -9 Furthermore, it is worth noting that athletes such as soccer players may have similar or worse symptom severity because of repetitive trauma to the foot. 10 Despite single-sport athletes experiencing worse pain scores during the preoperative period, they had similar improvements in pain scores and activities of daily living after undergoing the modified Kidner procedure (Table 5).
In a retrospective case series, Lee et al 11 found that the modified Kidner procedure led to a significant improvement in AOFAS and VAS. Similarly, we found that all patients undergoing the modified Kidner procedure had a significant improvement in pain and physical function as reflected by their VAS and FAAM scores (Table 4). However, the authors did not evaluate their cohort for outcomes related to sports. In our current study, we found significant improvement when comparing the preoperative FAAM ADL scale among self-reported single-sport and multisport athletes (P = .02). However, no difference was found between the 2 groups in the postoperative period.
Limitations
This study was limited by its retrospective design and reliance on the accuracy of electronic medical record documentation. Because of inconsistencies in documentation, we were unable to document the mechanism of injury in this cohort. Furthermore, missing data was not imputed, and no statistical methods were used to account for incomplete documentation of athletic classification or radiographic follow-up. Additionally, the retrospective design indicates that we were unable to increase the statistical power to detect changes at small effect sizes. Instances of missing imaging, such as MRI and postoperative radiographs, hampered a complete, retrospective evaluation of every patient.
Conclusion
Previous data has demonstrated that the athletic population is more likely to require surgical management for an accessory navicular. Athletes are equally likely to return to physical activity compared with nonathletes. Despite presenting with worse preoperative symptoms, single-sport athletes in our study appeared to achieve postoperative outcomes similar to those of nonathletes and multisport athletes following operative management.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251359654 – Supplemental material for Midterm Outcomes of the Modified Kidner Procedure for Accessory Navicular Syndrome in Athletes vs Nonathletes
Supplemental material, sj-pdf-1-fao-10.1177_24730114251359654 for Midterm Outcomes of the Modified Kidner Procedure for Accessory Navicular Syndrome in Athletes vs Nonathletes by Confidence O. Njoku Austin, Lauren E. Simonian, Asher B. Mirvish, David N. Fogg, Goodness C. Njoku Austin, Rajiv P. Reddy, Victor C. Crentsil, Matthew Como, Elizabeth O. Clayton, Onaje Cunningham, Logan E. Finger, Richard M. Smith and MaCalus V. Hogan in Foot & Ankle Orthopaedics
Footnotes
Author Note
The investigation was performed at the University of Pittsburgh Medical Center, Pittsburgh, PA.
Ethical Approval
A waiver of consent was granted by the institutional review board at the University of Pittsburgh for study 20020136. Retrospective chart review—waiver of consent was granted. No formal informed consent was obtained for patient inclusion in this study as no patient identifiers were included in the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.