
Abstract
Background:
Previous studies of conversion of failed ankle arthrodesis to total ankle arthroplasty showed failure in patients with an absent distal fibula, and more recently that has been considered a contraindication. However, these conclusions were based on limited case series with older prosthetic designs, and the potential for successful conversion in this challenging patient population remains unclear. This retrospective study examines the midterm follow-up of 21 patients treated for a conversion of failed ankle arthrodesis by a single surgeon using a standard technique with a single prosthesis, with a focus on the treatment of 5 patients with a deficient distal fibula.
Methods:
Between May 2010 and August 2019, 27 patients underwent conversion using a prosthesis with an intramedullary tibial component, 21 of which were available for the study. Six patients had a deficient distal fibula, and 5 were available for follow-up. Our primary outcome measure was having a total ankle arthroplasty in place. Secondary outcomes were evaluated postoperatively with a visual analog scale, the American Orthopaedic Foot & Ankle Society (AOFAS) ankle and hindfoot score, a satisfaction survey, and radiographic assessment of the arthroplasty and any concomitant hindfoot fusions.
Results:
Mean follow-up for all patients was 7.6 (2.6-11.8) years, with follow-up of the deficient fibula group of 8.2 (4.9-11.8) years. Complications included malleolar fracture with or without subsequent surgery (n = 5), varus deformity (n = 1), and wound dehiscence or infection (n = 2). At final follow-up, all patients, including the 5 with a deficient distal fibula, had an intact ankle arthroplasty, although 3 with intact fibulas had undergone prosthetic revision. Postoperative dorsiflexion was 4.5 ± 5.1 degrees and plantarflexion 20.9 ± 13.37 degrees. There were no pseudarthroses in the 11 patients with concomitant hindfoot arthrodesis. Mean (±SD) VAS score was 4.4 ± 3.0 and AOFAS score was 71.2 ± 21.7. Sixty-seven percent reported that they were satisfied or very satisfied, with 16% dissatisfied or very dissatisfied. One of the deficient fibula patients was very dissatisfied. Seventy-six percent had no limitations with activities of daily living and two-thirds of those had no limitations at all.
Conclusion:
Consistent with previous studies, we find that total ankle arthroplasty can be a satisfactory salvage procedure for patients with a failed ankle arthrodesis. Unlike previous reports, we observed high prosthetic retention in patients with a deficient fibula, although pain relief and range of motion outcomes were mixed, and some patients required revision surgery. These findings should be interpreted in light of the intrinsic limitations of a small sample size, lack of preoperative comparison data, and incomplete follow-up in the deficient fibula group.
Level of Evidence:
Level IV, clinical research.
This is a visual representation of the abstract.
Introduction
Although total ankle arthroplasty has been gaining acceptance, arthrodesis was long the traditional surgical treatment for painful ankle arthritis. Unfortunately, a number of significant problems can occur in patients who undergo the fusion procedure, including gait abnormalities, pseudarthrosis, malposition of the fusion, arthritis in the surrounding joints, and even pain in a well-positioned and healed fusion.4,5,13,16 Transtibial amputation is sometimes the result, but the limb-salvage treatments include repeat arthrodesis with or without osteotomies, tibiotalocalcaneal fusion, or pantalar fusion.2,3,5,11,13,14
In 2004, Greisberg and colleagues 6 reported on another option: conversion of failed ankle arthrodesis to a total ankle replacement. They found this to be a viable treatment but cautioned that it should not be used in patients with a deficient distal fibula. In their series of 18 patients, all 5 who had extensive thinning or resection of the lateral malleolus at the time of fusion had failure of the arthroplasty, including 3 who went on to below-knee amputation. Their patients were all treated with a second-generation prosthesis, the Agility Ankle (DePuy), no longer available in the United States.
Several subsequent studies using a variety of prostheses have further explored conversion procedures with short- to medium-term follow-up, confirming its utility as a salvage procedure, notwithstanding the incidence of intraoperative complications that can occur and recognizing that few patients end up with complete pain relief. Extending this procedure to patients with a deficient distal fibula has remained problematic, and the established teaching recognizes this as a contraindication for conversion.9,15,17 -20
The purpose of this report is to add our experience with deficient-fibula patients to the existing literature on conversion procedures.
Materials and Methods
Demographics
Between 2010 and 2019, a total of 27 patients with failed ankle arthrodesis were treated by conversion to an INBONE/INBONE II (Wright Medical, Stryker) total ankle arthroplasty by a single surgeon. Of those 27 patients, 3 had died, 2 were unable to be located, and 1 patient declined to participate in this study because of concerns about privacy. Twenty-one patients, 11 male and 10 female, with an average age 60 years (40-18) at the time of conversion comprised the general study group, seen at final follow-up an average of 90 months (31-141) after conversion. Two patients could only provide radiographs, 1 was unable to travel during the study period, and the other had just entered hospice. Six of the original 27 patients had a deficient fibula. Of these, 3 women and 2 men were able to participate. This group had a mean age of 58 years (40-69) at conversion and 66 years (45-79) at the final follow-up, which took place 98 months (48-141) after the conversion.
Three of the study group had their original arthrodesis procedure done for osteoarthritis; for one it was the index procedure, whereas a second had an arthroscopy prior to fusion and the third had an ankle arthroplasty that failed and required conversion to the arthrodesis. The remaining 18 patients had the arthrodesis done to treat posttraumatic arthritis that developed after ankle fractures.
The 5 patients in the deficient fibula group included 4 who had arthrodesis for posttraumatic arthritis, and 1 who had a failed ankle arthroplasty for treatment of osteoarthritis before undergoing the arthrodesis.
We recognized 3 modes of failure of the arthrodesis: Fourteen patients had a solid ankle arthrodesis but developed painful adjacent hindfoot arthritis, including 2 in the deficient fibula group (Figures 1 and 2). Four patients had a solid ankle arthrodesis in a painful malposition, including 1 deficient fibula patient (Figure 3). Three patients had a pseudarthrosis of the ankle, including 2 in the deficient fibula group (Figures 4 and 5).

Patient 1: (A, B) 50-year-old woman with failed ankle arthrodesis and subtalar arthritis with a varus fracture deformity in the tibia. (C, D) Initial postconversion views of original INBONE prosthesis with tibial stem placed in varus due to constraints of her fracture deformity. A talar body fracture was fixed with screws, and a subtalar fusion with fusion rods. After insertion of the prosthesis, there was demonstrable lateral instability, necessitating transfer of the peroneus brevis tendon into the distal end of the fibula stump at the same setting. Final follow-up 141 months after conversion (E, F) shows tibial-talar malalignment increased by 9.6 degrees. The tibial prosthesis alignment is unchanged. The ankle was stable and the patient declined further ankle surgery.

Patient 4: (A, B) 68-year-old woman with painful subtalar arthritis after an ankle arthrodesis for failed ankle ORIF. (C, D) Initial postconversion views show ankle prostheses in place. A talar body fracture was fixed with a single screw. A thin medial malleolus was fractured when the ankle was manipulated before the medial bone cut was completed. This was temporarily fixed at the time, and 10 days later definitive fixation was applied with the long plate and screws fixing the medial malleolus. A deltoid reconstruction was also done with an allograft tendon, and the button in proximal tibia adjacent to plate is fixation for that. The subtalar arthrodesis was fixed with a cannulated screw. The symptomatic plate and screws were removed 3 years after conversion. (E, F) At 121 months after conversion, the prosthetic alignment is maintained, and the subtalar fusion and the talus and malleolar fractures have healed with a hypertrophic medial malleolus.

Patient 5: (A, B) 69-year-old woman who underwent ankle arthrodesis for posttraumatic arthritis had previously also had a triple arthrodesis done. (C, D) She had painful malposition of her pantalar fusion. Initial postconversion views show large components, with fractures of the medial and lateral distal tibia. The lateral fracture was fixed with a single wire, with no fixation medially. (E, F) The final radiographs at 121 months after conversion show the prosthetic alignment has been maintained. The wire fixing the lateral distal tibia fracture was previously removed, and the fractures have healed with exuberant bone formation, leading to ankylosis of the joint. This patient was dissatisfied.

Patient 15: (A, B) 64-year-old man had previously been treated for osteoarthritis with a tri-component ankle replacement and calcaneal osteotomy. After developing an infection and undergoing prosthetic removal and several debridement procedures, he had arthrodesis attempted, but unfortunately developed a pseudarthrosis. He was advised to have an amputation. (C, D) Initial postconversion views show the ankle prosthesis in place. (E, F) The final radiographs at 49 months after conversion show a tibial-talar malalignment of 97.9 degrees. The tibial stem and talar component position are unchanged.

Patient 18: (A, B) 40-year-old man had multiple trauma from a fall off a bridge, including ipsilateral hip, femoral shaft, pilon, and calcaneus fractures. He had previously undergone multiple surgical procedures, including ankle and hindfoot arthrodesis that resulted in malposition with pseudarthroses. (C, D) Initial postconversion radiographs show the ankle prosthesis in place. (E, F) The final radiographs at 59 months after conversion demonstrated the prosthetic alignment has been maintained. A subtalar arthrodesis has been performed and has healed.
Operative Characteristics
All procedures were performed in the hospital except one that was done in an outpatient surgery center. The first 5 patients we converted were treated with the original INBONE prosthesis, with the INBONE II used in the remaining 22. 21 Our study group had 3 patients treated with the original INBONE and the remaining 18 treated with the INBONE II, with the same procedure for both.
Ten of the 21 study group patients had subtalar arthrodesis performed together with the conversion procedure. One of those patients also had a talonavicular arthrodesis. Two patients also had plates and screws removed, and 12 patients had screws alone removed. One patient had repair of a peroneus brevis tendon tear, and another had an excision of a calcaneal bone spur. All of these were scheduled to be done simultaneously with the conversion procedure.
Surgery and Postoperative Management
We developed a standard technique based on experience with some problems:
We began by removing any existing implants that would interfere with placement of the new prosthesis. Next, if a subtalar fusion was to be done, that joint was opened through an oblique incision over the sinus tarsi, and the joint surfaces prepared, leaving the fixation to be provided later. A standard anterior approach was used to expose the front of the ankle from medial to lateral malleoli.
The bone cuts for our prosthesis were made using a large leg-holding frame, but the importance of making proper bone cuts can be applied to any system. In some cases, it was easy to see where the original ankle joint line was—dorsally, medially, and laterally—and the monoblock cutting guide we used could be placed with reference to those on both anteroposterior (AP) and medial-lateral views (Figure 6). In other cases, cutting guide placement was approximated: on the AP view, the superior cut should be made to preserve as much malleolar bone as possible, acknowledging that with the proximal malleoli edges curving inward, a cut too proximal would narrow the bone that was left. Similarly, placement of the inferior cut should be conservative of the talus, with particular consideration of the upward slope of the subtalar joint posteriorly.

Location of bone cuts: (A) AP view of monoblock cutting guide placed with care to ensure the bone cuts will leave adequate malleolar bone to prevent fracture. (B) Lateral view of saw blades placed through the superior and inferior slits in the monoblock cutting guide to locate the site of the cuts. The inferior cut must not enter the subtalar joint posteriorly. (C) AP view after bone cuts have been made and the central bone segment has been removed. It is necessary at this point to complete the cuts between the talus and the malleoli both medial and lateral before any attempt is made to mobilize the ankle. AP, anteroposterior.
Finally, a smaller cutting guide is generally a better choice than a larger one. We learned by unfortunate experience that making cuts that leave very thin malleolar bone remnants would lead to fractures (Figures 2 and 3). The situation in Figure 3 shows medial and lateral distal tibia fractures associated with using large components, which had been our preference in the first few patients.
Another important point is that the gutters must be completely free, using the oscillating saw, small rongeurs, and curettes to ensure that the talus is separated from the medial and lateral malleoli before any attempt is made to move the ankle (Figure 6). Figure 2 demonstrates a medial malleolus fracture that occurred when the ankle was manipulated after an incomplete medial gutter debridement.
After prosthetic insertion, if a hindfoot arthrodesis was performed, bone graft was salvaged from the ankle bone cuts and placed into the joint, with fixation applied with screws or fusion rods.
Postoperative care included removing the skin staples after 7-10 days, and then a short-leg nonweightbearing cast was applied. Patients were kept in the cast for 3 weeks unless a fusion was done, in which case the cast was changed at 6 weeks postoperatively. When the cast was removed, a walking orthosis was used for 4 weeks with no fusion or 6 weeks with a fusion. We routinely obtained ankle radiographs at 3 months and 1 year postoperatively.
Follow-up Evaluation
Patients were contacted, provided informed consent, and were scheduled for a radiograph and office visit, where they were assessed by an orthopaedic surgical resident not involved in the surgery. They completed questionnaires for functional assessment of activities of daily living (ADL) using the American Orthopaedic Foot & Ankle Society (AOFAS) hindfoot score, which was chosen for comparison with the older existing studies that relied on it. 12 Ankle range of motion (ROM) was measured clinically with a goniometer as this had been previously described. 17 Total ROM was computed as the sum of the plantarflexion and dorsiflexion. Foot and ankle pain levels were assessed using the visual analog scale (VAS), where 0 indicated no pain and 10 indicated unbearable pain. 8 Patient satisfaction was categorized as not satisfied or neutral, versus satisfied, based on a self-described 5-point scale (1 = very dissatisfied, 3 = neutral, 5 = very satisfied).
Radiographic Evaluation
Preconversion radiographs were assessed to determine the nature of pathology for each patient, categorizing them as due to a pseudarthrosis of the ankle, arthritis in the surrounding joints, malposition of the ankle or hindfoot, or pain in conjunction with a radiographically satisfactory arthrodesis. A review of these radiographs found that they were not performed in a consistent fashion.
Assessment of radiographs taken in the first 3 months after the conversion procedure (early postoperative films) and final follow-up (final films) were generally weightbearing, although in 3 cases the early postoperative films were nonweightbearing.
Tibial alignment alpha angles (coronal implant angle) and beta angles (sagittal implant angle) were measured using parameters previously described, except that the calibrated templating feature (Visage 7 Enterprise Imaging Platform; ProMedicus Ltd, Australia) used does not make circular determinations, leaving the center of the tibial shaft proximally and the center at the metaphysis up to the observer’s judgement. 1 We did not include measurement of the talus prosthesis on the talus bone because our observer found it difficult to determine the axis of the talar neck on the radiographs.
Additionally, we performed a tibial-talar alignment measure on the early postoperative and final AP films. This describes the angle between the longitudinal axis of the tibial stem and a line along the base of the talar component, taken on the medial superior quadrant formed by the lines (Figure 7). We have considered this a measure of subluxation of the talar component under the tibial component.

Tibial-talar alignment: This is the angle measured between the longitudinal axis of the tibial prosthesis stem and the undersurface of the talar component on the AP radiograph. The measurement is made of the angle in the superior medial quadrant. An angle of 90 degrees defines perfect alignment. Measurements <90 degrees indicate a varus subluxation of the talus and measurements >90 degrees indicate valgus subluxation. Tibial-talar alignment for patient 1: (A) on the initial radiograph the angle is 92.6 degrees, and (B) on the final radiograph it is 102.2 degrees. Tibial-talar alignment for patient 15: (C) on the initial radiograph the angle is 93.5 degrees, and (D) on the final radiograph, it is 97.9 degrees.
The radiographic assessment was conducted by an orthopaedic surgeon uninvolved in the surgery or clinical evaluation of these patients.
Data Management and Statistical Analysis
Study data were collected and managed using REDCap electronic data capture tools hosted by our institution and imported into IBM SPSS 29.0 for analysis. 10
Descriptive statistics were computed for all follow-up measurements. The differences in the initial versus final alpha, beta, and tibial-talar malalignment were compared using a paired t test. Correlation coefficients were computed to assess the association of the VAS scores with patient satisfaction.
Results
Clinical Results
The mean AOFAS score for the study group was 71.2 ± 21.7. However, only 3 of the 5 patients in the deficient fibula group had clinical results recorded. The small sample sizes prevented comparisons of the fibula-intact and fibula-deficient groups.
The activity scores for the entire group found 56% (10 patients) having no limitations with any activity and an additional 22% having no limitations with ADLs but some limitations with recreational activities (14 patients total). ADLs were limited in 22% (4 patients total), and 3 of those also required the use of some assistive devices.
Total ROM was 28.5 ± 14.8 degrees for the patients with an intact distal fibula, and 13.8 ± 18.9 for the patients with a deficient distal fibula. The fibula-intact group mean dorsiflexion was 5.0 degrees (0-35 ± 5.5), with a plantarflexion of 23.9 degrees (5-40 ± 11.4). Mean dorsiflexion for the fibula-deficient group was 2.5 degrees (0-5 ± 2.9) and plantarflexion was 11.3 degrees (0-35 ± 16.5). One patient in the fibula-deficient group had 0 degrees dorsiflexion and 0 degrees plantarflexion, and with only 3 patients in this group having clinical results, this one negatively influenced the group results.
The mean VAS was 4.4 ± 2.25 for patients with an intact distal fibula, and 6.0 ± 3.61 for patients with a deficient distal fibula. Only 1 of the patients, in the intact fibula group, had a 0 VAS score (pain-free). One of the 3 fibula-deficient patients had VAS 9.
Patient satisfaction assessment found that 68% of patients were very satisfied or satisfied (13 patients), and 3 patients (16%) considered themselves to be neither satisfied nor dissatisfied. Three patients (16%) were dissatisfied or very dissatisfied (n = 1).
Patient satisfaction was highly negatively correlated with the VAS scores. Lower pain yielded higher satisfaction as measured by the VAS (ρ = −0.767, p < .001)
Radiographic Findings
The prosthetic alignment measurements are summarized in Table 1 for the patients who had not undergone revisions. There was no statistically significant change in either the alpha or beta angles for either fibula-intact or fibula-deficient groups from the initial postoperative evaluation to the final follow-up examination.
Initial Postoperative and Final Follow-up Tibial Prosthesis Angles.
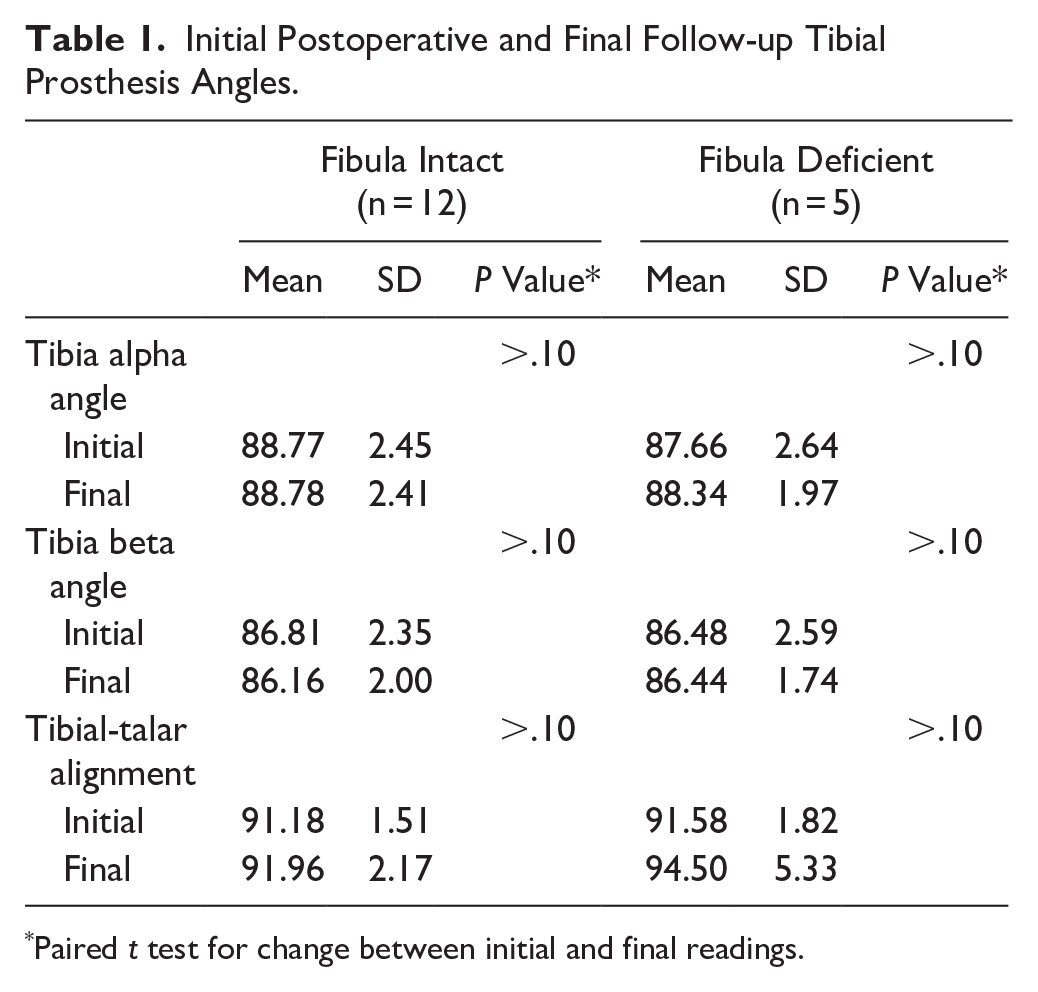
Paired t test for change between initial and final readings.
Tibial-talar alignment was similarly statistically unchanged within the fibula-deficient and fibula-intact groups. However, the standard deviation for the fibula-deficient group was larger on the final follow-up examinations (Table 1). This is due to changes in 2 patients, one progressing by 9.6 degrees and the other by 4.4 degrees (Table 2; Figure 7). The patients who had concurrent hindfoot fusions (10 subtalar and 1 talonavicular) all demonstrated solid arthrodesis. There were no evident problems with the implants fixing the arthrodesis.
Individual Tibial-Talar Alignment for the 5 Patients With a Deficient Fibula. a
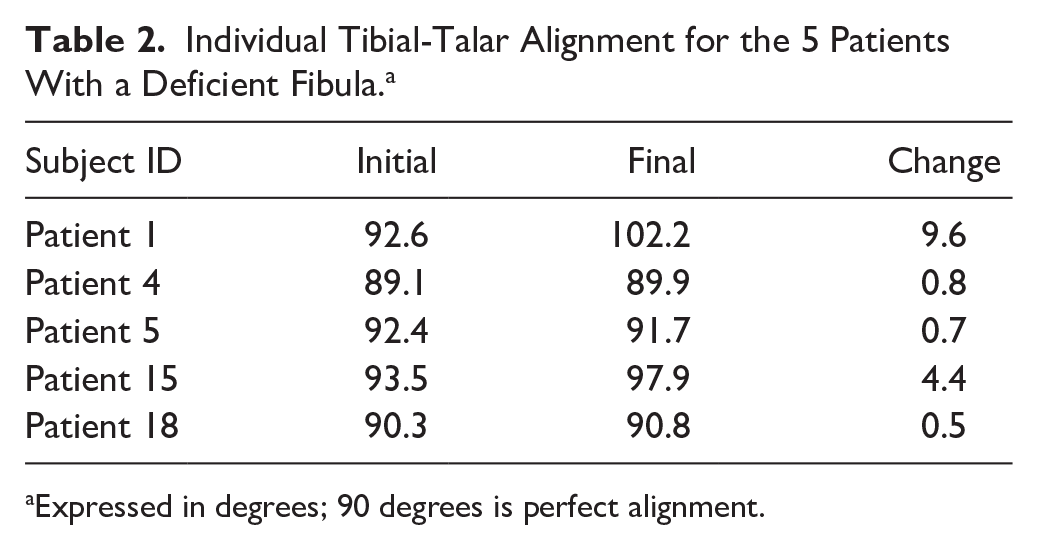
Expressed in degrees; 90 degrees is perfect alignment.
Complications
Five patients had fixation of intraoperative fractures. One lateral malleolar and 1 medial malleolar fracture were treated with plates and screws, a lateral distal tibia fracture was treated with a single K-wire, and 2 talus fractures were treated with screws. Two of these 3 patients had a deficient fibula. One fibula-deficient patient had lateral ankle instability after the leg was removed from the frame, and this was treated at the time with a peroneus brevis transfer into the fibula stump (Figure 1). One of those treated with plate fixation of a medial malleolus fracture had it redone 10 days later, combined with a deltoid ligament reconstruction (Figure 2). That was followed 3 years later with the removal of the plate and screws fixing the fracture.
The remaining complications and subsequent surgical procedures occurred in patients with an intact fibula (Table 3). Two of them developed wound-healing problems. One was superficial and was adequately treated with a wound vacuum-assisted closure. The second one, who had also had plate and screw fixation of an intraoperative lateral malleolus fracture, developed a deep infection requiring 3 debridements and finally INBONE prosthetic implant removal 3 months postconversion with the placement of an antibiotic spacer and then intravenous antibiotic treatments. That patient had revision surgery to reimplant a prosthesis 9 months after the original conversion (Figure 8, patient 12).
Complications Reported in Previous Studies and in the Present Investigation.


Longevity of conversion in intact and deficient fibula patients. Three intact fibula patients—3, 12, and 19—underwent prosthetic revision, with the time after conversion noted (X). Other minor procedures were conducted in patients 4, 8, 14, and 18.
Other problems developed in patients in the years after the conversion. One patient with an original INBONE prosthesis developed a fracture in a thinned lateral malleolus with subluxation of the joint 39 months after the original procedure. He underwent revision to an INBONE II, as well as having ORIF of the lateral malleolus and a deltoid ligament reconstruction with allograft (Figure 8, patient 3).
Another patient had ankle stiffness with residual equinus and varus after the conversion, and 5 months later underwent revision combined with a calcaneal osteotomy and fusion of the talonavicular and calcaneocuboid joints (Figure 8, patient 19).
The patient with the superficial infection (Figure 8, patient 8) underwent 2 separate calcaneal osteotomy procedures, the first one 2 months after the conversion, and the second one 39 months after the surgery. Finally, 91 months after the conversion the calcaneal screws were removed.
All told, 4 patients with an intact distal fibula underwent subsequent surgeries, 2 of them having 1 procedure, and 2 of them having 4 procedures. Two patients with a deficient fibula had subsequent surgery, a single procedure in one, and 2 procedures in the other.
Prosthetic Failure
As noted above, 3 patients had INBONE prosthetic failure (Figure 8, patients 3, 12, and 19). All were satisfactorily revised. There were no prosthetic failures in the 5 patients with a deficient fibula. All 21 patients had a total ankle replacement in place at the time of follow-up.
Discussion
This study was performed to evaluate our experience in conversion procedures for salvaging failed ankle arthrodesis. Our findings demonstrate that conversion can be a viable salvage option, with all 21 patients retaining their prostheses at midterm follow-up. Similar to previous studies with shorter follow-up, we found it to be a reasonable salvage procedure for patients with an intact distal fibula. Notably, our results in the fibula-deficient subgroup differ from previously published reports, though the small sample size limits definitive conclusions. Other reports have noted a high incidence of failures in patients with a deficient fibula and those reports have led to a uniform dismissal for this condition (Table 3).6,7,9 -12
The baseline for comparison for treatment of failed ankle fusion is a revision of the arthrodesis. Although studies show that most patients ultimately have a satisfactory fusion, they also describe problems with the procedures, including a high number of complications and repeat operations, and even amputations in some patients. None of them identify treating patients with a deficient fibula.
In 1991, Kirkpatrick et al 11 used a fibula onlay graft and screw fixation in 11 patients, with successful bone union in nine, and a painless pseudarthrosis in a tenth. Kitaoka et al 13 treated 26 patients with an external fixator, and bone grafting in 18 of them, obtaining bone union in 77%. They had 16 good or excellent results, and found 20 of their 26 patients either satisfied or somewhat satisfied. Twenty-three percent of their patients had complications. Anderson et al 2 reported using internal compression screws in 20 patients, thirteen with pseudarthrosis and 7 with malunions. They had bone healing in 15 of the 20, although complications occurred in 55% of the patients, with 12 patients needing 19 additional procedures. Ultimately 17 were satisfied, including 3 who had amputations. Levine et al 14 treated 23 arthrodesis failures with autologous bone grafting, using internal fixation in 18 and external fixation in the other 5. Nine of the patients had additional hindfoot fusions treated: 7 were tibiotalocalcaneal and 2 pantalar. Twenty-one were successful in bone fusion, with 19 satisfied with the surgery. Easley et al 5 treated 45 failures with internal fixation, ring external fixation or tibiotalocalcaneal fusion and had an overall 89% fusion rate. The 5 patients who did not fuse elected to have transtibial amputation. They found 19 major and 33 minor complications among their patients.
A review of the clinical outcomes for conversion patients in the literature show an average range of AOFAS scores from 68 to 75 (Table 4). This is lower than the 78.2 reported for primary total ankle arthroplasties in a systematic review from 2007. 7 Complete pain relief from the surgery has been elusive, found in less than 20% of the patients. The average ankle range of motion is about 25 degrees total.
Results of Prior Studies of Conversion to TAR Compared With Present Investigation.

Visual analog scale (VAS) score 0-100. Others are 0-10.
Not available.
The patients in the present investigation had an AOFAS score of 71.2, which compares favorably with the range of 68-75 reported in the literature. Our patients had a slightly lower satisfaction level of 68% compared with satisfaction rates in the 80%-90% range in other studies. However, if the 3 patients who stated “neither satisfaction or dissatisfaction” are discounted, our dissatisfaction rate was only 16 percent, consistent with previous reports (Table 4).
The persistence of increased pain in our patients with an average VAS of 4.6 is higher than the averages in the literature that range from 1.5 to 3.0 (corrected for the scale of 0 = no pain). Although not statistically significant, it appears that having several patients with VAS over 7 may have resulted in our higher overall VAS scores. We did find that a lack of persistent pain was correlated with higher patient satisfaction for our group of patients.
We were not collecting preoperative subjective data in a systematic fashion during the early years of this study, so it is not possible to interpret our subjective data without that baseline for comparison.
The total ROM of our patients averaged 27 degrees, consistent with that found in the previous studies (Table 4).
Most conversion studies report prosthetic implant failures in about 10% to 15%, and our 3 of 21 patients (14%) were in this range (Table 3). These 3 prosthetic failures were all revised, and all of our patients had an intact arthroplasty in place at the final examination.
All patients in this study had a stable radiographic appearance of the tibial prosthesis, with no significant changes in the tibial alpha (coronal) or beta (sagittal) angles or tibial-talar alignment between the initial and final follow-up examinations. All hindfoot arthrodesis performed at the time of conversion went on to fusion.
Previous conversion studies found intraoperative fractures to be a common complication (Table 3), and we also had that problem. Three of our first 5 patients had malleolar fractures, with 2 of them also having talus fractures. These should have been avoidable, and with experience we took better care to follow the recommendations we described previously in the techniques section. Specifically, the use of smaller prosthetic implants, careful positioning of the bone cuts to avoid leaving thin sections more susceptible to fracture, and care to completely free the gutters between the talar body and distal tibia and fibula before attempting any ankle motion decreased our fracture rate. Even so, we had 2 further cases with malleolar fractures in the ensuing years.
The radiographic evaluation of the fibula-deficient patients show that the tibial components remained stable through the final follow-up. There were no statistically significant changes in tibial-talar angles over time, and 3 of the 5 patients in the study showed no radiographic changes in the prosthesis alignment at the follow-up examination. However, 2 of them (patients 1 and 15) had a worrisome increase in valgus angulation of 9.6 and 4.4 degrees comparing their final radiographs with the initial ones. The patient with the greater valgus angulation had been treated with the original INBONE prosthesis with less coronal-plane stability than INBONE II used in the other patient, and in the subsequent 3 who showed no valgus instability. 21 It is interesting to speculate if that design change resulted in enough stability to overcome an absent lateral strut in these patients. There are no other obvious factors to account for the stability we found in these patients, but it must be emphasized that these are a small number of patients, and it is not possible to attribute the results to this particular prosthesis.
The strengths of this study include a follow-up time of up to 11 years of a cohort that had the same procedure by a single surgeon using a single prosthesis. However, we recognize that there are important limitations in the study. First is the small number of participants, which is primarily due to the unusual nature of the treatment. Our study group was further limited to 21 of the 27 patients who had conversion surgery, a 22% loss, although there does not appear to be selection bias because 3 were due to patient death and a fourth patient who declined to participate because of her political beliefs, and 2 could not be located. We had no preoperative clinical data, so we are unable to make comparisons with the final results. Further, we had incomplete follow-up clinical data on 2 fibula-deficient patients—one who went into hospice and the second who was unable to travel to our facility for the examination. There were no standardized initial postoperative radiographs, and although we ordered weightbearing radiographs for the final follow-up assessment, they were performed in different facilities by different radiology technicians. The angular measurements on the radiographs were measured by a knowledgeable orthopaedic surgeon but were not verified by a second observer, and the software for making the measurements of the tibial canal could only make straight lines, so the suggested format of drawing circles in the midshaft of the tibia and the tibial metaphysis to best determine the central axis of the bone could not be applied. This limitation may have introduced variability in measurements, particularly for small alignment changes. In addition, it was not possible to make satisfactory measurements of the talar prosthesis position on the lateral radiographs, limiting the ability to assess talar subsidence. Although we made use of a goniometer to measure ankle ROM as had been done in a previous study, we recognize that this technique is not as accurate as measuring on radiographic dorsiflexion and plantarflexion views.
Conclusions
Based on our case series, conversion of failed ankle arthrodesis to total ankle arthroplasty can provide acceptable midterm outcomes, with all patients retaining their prostheses at an average 7.6-year follow-up. We have shown that patients with a deficient fibula undergoing conversion may retain their total ankle prosthesis for more than 10 years, although the extremely small sample size (n = 5) precludes definitive conclusions about safety or efficacy in this population.
Our findings suggest that the absolute contraindication for conversion in patients with deficient fibula may warrant reconsideration, but this should only be attempted by experienced surgeons in carefully selected patients. They suggest a counterpoint to the accepted teaching, and we hope this may lead to its inclusion in the conversation regarding salvage options for these patients, with the ultimate goal of properly designed prospective studies to assess its utility.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251351636 – Supplemental material for Midterm Outcomes Following Conversion of Failed Ankle Arthrodesis to Total Ankle Arthroplasty, Including Patients With a Deficient Fibula
Supplemental material, sj-pdf-1-fao-10.1177_24730114251351636 for Midterm Outcomes Following Conversion of Failed Ankle Arthrodesis to Total Ankle Arthroplasty, Including Patients With a Deficient Fibula by George Lian, William Ip, Andrea Hankins, Michele Guillen and Carol Parise in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from the Sutter Health Institutional Review Board, Approval number SHIRB: 2022.005-2. Patients provided written informed consent for study participation.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: George Lian, MD, received travel expenses for educational conference from Stryker Corporation, the manufacturer of the prosthesis used in this study. Disclosure forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from Sutter Medical Center, Foundation (Grant 947110-1107721).
Data Availability
Data for the study are not publicly available. Patients provided informed consent for study participation, but exportation of data externally was not included.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.