
Abstract
Background:
The use of fourth-generation minimally invasive hallux valgus surgery with metaphyseal extra-articular transverse and Akin osteotomy, recently dubbed “META,” is a new generation of minimally invasive surgical (MIS) technique and a recent focus of foot and ankle orthopaedic literature associated with good functional outcomes and low complication rates. Literature in orthopaedic trauma has indicated that 2 or 3 neocortices on postoperative radiographs are associated with high likelihood of union. In this study, we conducted a retrospective analysis to investigate the time to bony union for patients undergoing fourth-generation MIS hallux valgus repair as well as the relationship between intraoperative degree of first-metatarsal displacement and time to bony union.
Methods:
We retrospectively analyzed 217 consecutive patients with moderate to severe hallux valgus who underwent fourth-generation MIS first distal metatarsal and Akin osteotomy between 2020 and 2023 and were followed for up to 1 year. Radiographic measurements included the scale of displacement between the proximal and distal portions of the first metatarsal as a percentage and the number of neocortical bridge formations at the osteotomy site. Postoperative weightbearing radiographs were recorded at 6 weeks, 3 months, 6 months, and 1 year to assess time to union and patient clinical outcomes. Two orthopaedic surgeons independently reviewed the radiographs to assess progression to bony union. Any discrepancy in analysis was resolved by a third-party clinician. Complete union was defined as the presence of at least 2 new cortical bridge formations on postoperative X-ray films. Patients were divided into 3 groups based on the percentage of shift on the first metatarsal head (≤50%, 51%-75%, ≥76%) for the purpose of our analysis.
Results:
Union (≥2 cortices) was observed in 17%, 70%, and 90% of patients at 6 weeks, 3 months, and 6 months, respectively. At final follow-up (mean 13 ± 6.9 weeks), 92% achieved union. No significant differences in time to union were observed across metatarsal shift groups.
Complications include 3 nonunions, 3 revisions, 16 cases that necessitated removal of hardware, 1 case of superficial wound infection, 1 case of deep wound infection, and 6 deformity recurrences.
Conclusion:
Time to union after META procedure typically occurred by 13 weeks, independent of shift magnitude. Surgeons may consider ≥2 cortices and absence of symptoms as sufficient indicators for advancing weightbearing. These findings may assist in patient counseling and postoperative planning.
This is a visual representation of the abstract.
Introduction
Surgical techniques for addressing symptomatic hallux valgus have advanced considerably over the past 2 decades, with minimally invasive surgery (MIS) emerging as a key focus in foot and ankle orthopaedic research. Traditionally, much of the research has centered on third-generation MIS procedures, characterized by the chevron wedge osteotomy combined with the Akin osteotomy.2 -5,10 However, fourth-generation MIS technique has recently been developed, incorporating a metaphyseal extra-articular transverse and Akin osteotomy, recently dubbed “META.” 3 This updated approach allows for a dual correction: a lateral shift of the metatarsal bone and a rotational adjustment, enhancing the alignment of the sesamoid bones and addressing complex deformities more comprehensively. Although investigations into this innovative surgical method are still in their early stages, preliminary outcomes have shown promising improvements in both function and alignment, highlighting its potential to redefine hallux valgus management while maintaining low malunion and nonunion rates.
Clinical evaluation of bony union and bony nonunion are a frequent focus of orthopaedic studies. Investigation of bony nonunion is commonplace in the literature due to dire clinical implications including infection, poor patient outcomes, decreased recovery, high health care costs, and potential mortality. The rate of increased nonunion may be associated with certain risk factors, which can be categorized as host, biological, or mechanical factors. Some examples of these factors include smoking, age, diabetes, steroid use, vascular supply, complications of the fracture, and gender. Some factors such as diabetes and age are very well understood why nonunion may occur. On the contrary, more studies are needed to fully understand nonunion rates on gender, method of fixation, and level of immobilization. One thing that is clear is that the rate of nonunion increases with the number of risk factors a patient has. 8
A plethora of orthopaedic studies have been performed to evaluate union rates in various population sets, bone groups, and injury types. Although there appears to be a consensus regarding the time for bones to heal, to date there has been no definition provided for what constitutes bony union. In most cases, union is simply suggested by the radiographic reviewer. 7 This problem of having an ambiguous definition of bony union is consistent across orthopaedic literature.1,13 In the current literature, authors vary in studies on defining “union” as either tricortical or quadricortical callus formation at the site of the fracture (Figures 1 and 2). Authors use cortical formations measured by multiple radiographic images to determine whether union or nonunion will occur. 6 In addition, the timeline of union is also variable depending on the type of bone fractured, with one study reporting time to union for distal femur fractures to be approximately 28 weeks. 9 A systematic review of bony union found the mean time to fracture union in 49 studies comprising 2441 cases to be 18 weeks (range 12-36 weeks). 12 In a previous study, there was clear variation in the time to union depending on the bone fractured. Van Kollenburg et al 11 found that the average time to union was the highest in diaphyseal tibia fractures, which was 32.1 ± 7.4 weeks. Of the other fractures analyzed, humeral fractures treated with nailing or plating had the shortest time to union, with an average of 10.9 ± 2.7 weeks.

Postoperative weight bearing anteroposterior and lateral radiographs showing 4 neocortical bridge callus formations following fourth-generation minimally invasive hallux valgus correction surgery.
Materials and Methods
Study Design
A retrospective cohort study was designed to compare the radiographic and clinical outcomes of patients who underwent fourth-generation MIS hallux valgus correction. The study aimed to investigate the time for MIS hallux valgus patients to achieve bony union, defined as at least 2 neocortical bridge callus formations on radiographs. Additionally, we explored the relationship between the intraoperative degree of first-metatarsal displacement and time to bony union. Radiographic measurements, including time to radiographic union, degree of first-metatarsal shift, and the overall rate of union were assessed as primary outcomes. The secondary outcomes included a comparison of traditional radiographic measurements including the hallux valgus angle (HVA) and intermetatarsal angle (IMA). Adverse outcomes included but are not limited to revisions, infection, hallux valgus recurrence (defined as a change in HVA of 2.5 between any 2 postoperative radiographs or a HVA >15 degrees), nonunion, or hardware malfunction.
Patient Selection
The study included patients who underwent primary hallux valgus deformity correction using fourth-generation META surgery. The surgeries were performed by 3 fellowship-trained foot and ankle orthopaedic surgeons at a single center in Miami, Florida, between September 2020 and December 2023. The inclusion criteria encompassed patients who had postoperative weightbearing radiographs available for evaluation and those who maintained consistent follow-up. Patients who underwent MIS hallux valgus surgery as a revision, an open surgery for hallux valgus correction, or were lost to follow-up were excluded from the analysis. All patients followed similar postoperative weightbearing protocols, which included full weightbearing as tolerated in a postoperative sandal up to 2 weeks followed by progression of activities as tolerated.
Radiographic Evaluation
All patients underwent follow-up radiograph evaluations at 2 weeks, 6 weeks, 3 months, 6 months, and up to 1 year. Two orthopaedic surgeons, masked to the patient’s group assignment, independently reviewed the radiographs to assess and quantify time to radiographic union (measured in weeks). This assessment involved examining the presence of certain indicators at the fusion site, including lucency, bridging trabeculae, or evidence of hardware failure. Specifically, if a patient was both asymptomatic and their plain radiographs showed clear union through the presence of a bridging callus with neocortical bone formation in at least 2 planes, it was categorized as a bony union. Intraoperative first metatarsal shift, given as a percentage, was measured by taking the distance from the medial aspect of the distal metatarsal to the lateral aspect of the proximal metatarsal divided by the width of the first metatarsal at the level of the osteotomy (Figure 3). The presence of lucency or signs of hardware failure was considered indicative of nonunion and thus treated as an independent outcome measure. The occurrence of complications, such as malunion or any instances requiring revision surgery, were also documented and reported.
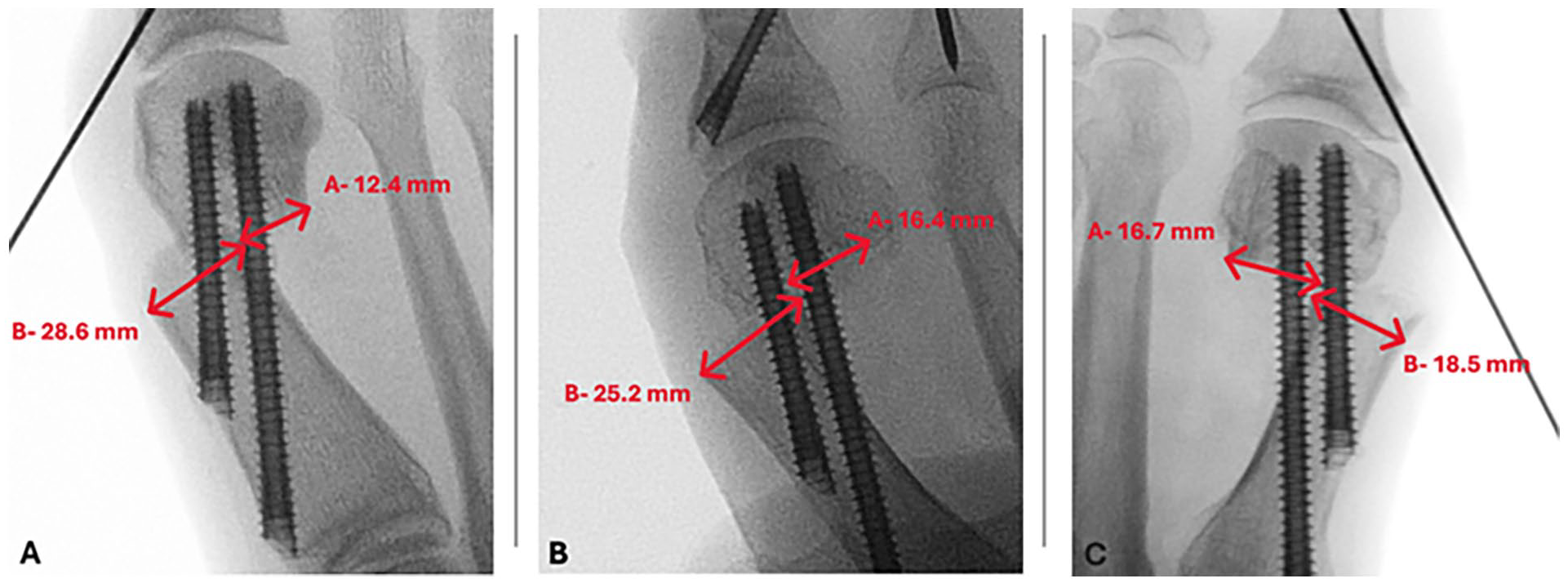
Anteroposterior radiographs showing first-metatarsal shift percentage, recorded as the distance from the medial aspect of the distal metatarsal to the lateral aspect of the proximal metatarsal divided by the width of the first metatarsal at the level of the osteotomy. (A) Less than or equal to 50%, (B) 50%-75%, and (C) greater than 75% first-metatarsal shift.
Statistical Analysis
Descriptive statistics were used to summarize the demographic characteristics of the patients. Continuous variables were reported as mean ± SD. Categorical variables were presented as frequencies and percentages. The mean time to radiographic union was compared using a 1-way analysis of variance and Games-Howell post hoc test. Additionally, radiographic angles preoperatively and at the time of final follow-up were compared using 2-tailed t tests. The significance level was set at P <.05. The statistical analysis was performed using statistical software (Excel, Analysis ToolPak, Python).
Ethical Considerations
The study protocol was reviewed and approved by the Institutional Review Board (protocol no. 1952671-1) of the research center. Patient confidentiality was strictly maintained throughout the study, with all data anonymized and stored securely.
Results
Patient Demographics
The cohort (N = 217) consisted of 195 women and 22 men, with an average age of 56 ± 14.9 years and a mean body mass index of 26 ± 4.5. There were 33, 101, and 83 patients with a metatarsal shift of less than or equal to 50%, 51%-75%, and greater than or equal to 75%, respectively. Patient demographics are summarized in Table 1.
Summary of Time to Union Patient Demographic Information and Degree of First-Metatarsal Shift. a

Abbreviations: BMI, body mass index; MT, metatarsal.
aContinuous data are represented as mean ± SD. Categorical data are expressed as a count and percentage (of total).
Analysis of Cortical Formation Across Shift Categories
A descriptive analysis was performed on each shift category of ≤50%, 51%-75%, and ≥76%, showing the percentage of patients in each category with bony union at each follow-up period (Figure 4), along with the mean time for bony union in each category. The mean time to union in the ≤50% group was 22.1 ± 9.2 weeks, 21.6 ± 11.1 weeks in the 51%-75% group, and 26.6 ± 16.4 weeks in the ≥76% group (Figure 5).
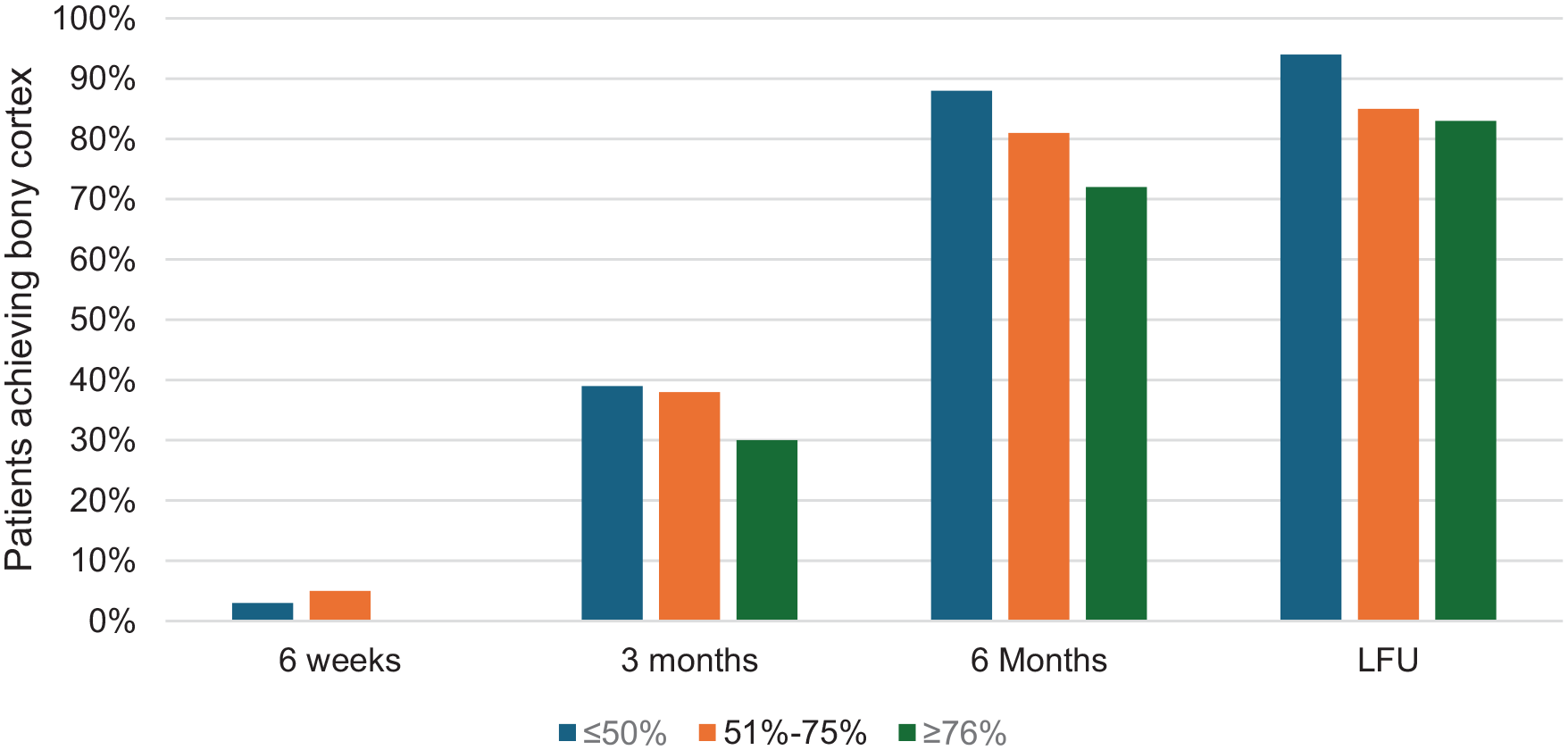
Percentage of patients achieving bony cortex formation across the metatarsal shift category.

Mean time to union by metatarsal shift category.
An additional analysis was performed to determine if there was a significant difference in the time it took to achieve bony union across each shift category. A 1-way analysis of variance alongside a Games-Howell post hoc test were performed to determine the significance across each shift. When looking at the results of the Games-Howell post hoc test, there was no significant difference in the time to achieve bone to union (Table 2).
Games-Howell Post Hoc Test Results of Mean Time to Bony Union Across All Shift Categories.

Significant at P < .05.
Analysis of Cortical Formation Regardless of Shift Category
A secondary descriptive analysis was performed to evaluate the percentage of patients that had achieved 1, 2, or 3 cortical bridge formations, across 6 weeks, 3 months, 6 months, and at the time of final follow-up, regardless of metatarsal shift group (Table 3; Figure 6). At final follow-up (mean 13 ± 6.9 weeks), 92% of patients were healed with radiographic evidence of 2 neocortices. When analyzed categorically, 17% of patients were healed at 6 weeks, 70% of patients were healed at 3 months, and 90% of patients were healed at 6 months.
Percentage of Patients Achieving Bony Cortical Formations at 6 Weeks, 3 Months, 6 Months, and Last Follow-up Regardless of Shift Category a
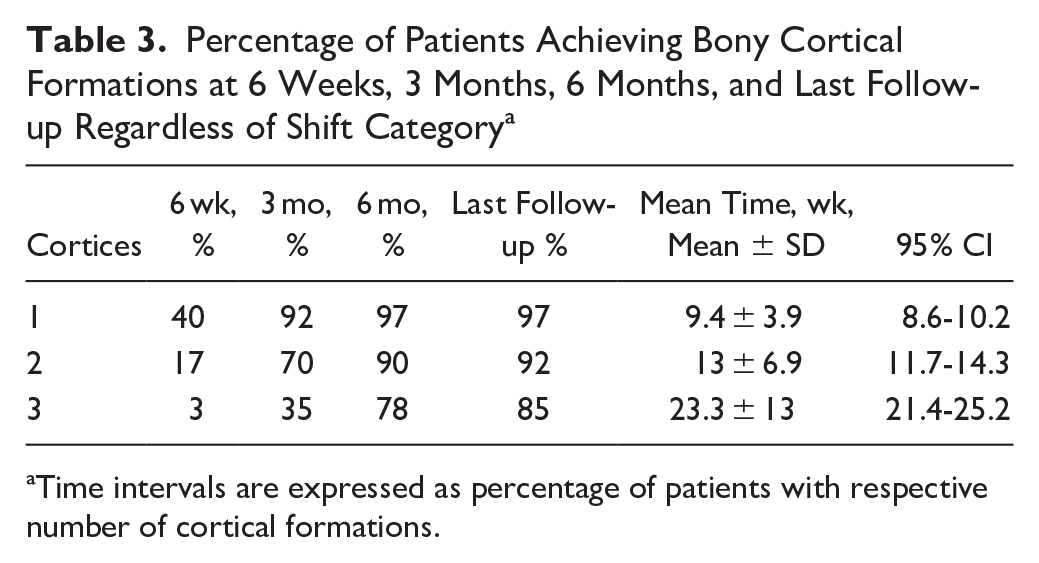
Time intervals are expressed as percentage of patients with respective number of cortical formations.

Mean time to 1, 2, or 3 cortical formations regardless of metatarsal shift.
Radiographic Outcomes of HVA and IMA
The mean preoperative HVA and IMA were 28.7 ± 7.7 and 12.8 ± 3.1 degrees, respectively. The mean HVA and IMA at final follow-up were 8.6 ± 6.4 and 4.4 ± 2.8 degrees, respectively. The mean preoperative to postoperative differences for both HVA and IMA were statistically significant with the HVA decreasing −20.1 degrees (P < .01) and the IMA decreasing −8.4 degrees (P < .01) (Table 4).
Radiographic Measurements Including Hallux Valgus and Intermetatarsal Angles.

Postoperative Complications
There were 32 patients (14.74%) with at least 1 or more postoperative complications. One patient had a superficial skin infection resolved with antibiotics and 1 patient had a deep wound infection, resolved with a course of antibiotics and wound debridement. Sixteen patients required surgical removal of hardware because of discomfort from a prominent screw. Two patients had exostosis formation, resolved surgically. Six patients experienced deformity recurrence; however, only 2 reported dissatisfaction and opted for revision surgery. One patient required revision because of excessive metatarsal screw length. There were 3 nonunions: 1 case at the proximal phalanx osteotomy site, resolved with screw removal and a revision osteotomy; 1 case of a nonunion at the metatarsal osteotomy site, for which the patient was asymptomatic; and 1 case of nonunion at the second metatarsal osteotomy, which was also approached conservatively because of a lack of symptoms.
Discussion
In this retrospective cohort study, we evaluated time to radiographic union in patients undergoing fourth-generation minimally invasive (META) surgery for hallux valgus correction. Our findings demonstrate that the vast majority (92%) achieved union—defined as formation of at least 2 neocortical bridges—by an average of 13 weeks. When using a more stringent definition of union (3 cortices), the average time extended to 23.3 weeks, which is consistent with most publications across various orthopaedic subspecialties, suggesting bony union to be expected around 6 months (26 weeks). 9 Importantly, the extent of intraoperative metatarsal shift did not influence time to union, suggesting that aggressive deformity correction did not delay healing with this surgery.
As novel methodologies of MIS hallux valgus surgery emerge, it is important to study and produce literature on outcomes, techniques, and effectiveness to contribute to optimal orthopaedic care. With more orthopaedic physicians employing the use of the newest generation of MIS techniques, it is important to justify exciting trends with verifiable and comparable outcomes. 3 Definitions of bony union have been inconclusive and controversial in orthopaedic literature, with the only consensus appearing to be the average time for bones to heal across the general population.1,6,7,13 To our knowledge, no study exists to investigate bony union in MIS hallux valgus surgery nor has there been a study to evaluate the effect of different intraoperative corrective techniques and their effects on patient outcomes.
Various limitations exist in our study. The retrospective study comes with inherent biases in analysis and may lessen the strength of our establishment of causality. Our sample size, although appropriate for both the specific procedure and patient subset, may inhibit this study’s statistical power. Our findings were provided through radiographic and clinical assessments. Despite any discrepancies being settled by a separate, masked orthopaedic physician, observer bias is a variable that affects interpretation of outcomes. Although our patient population is similar to the known populations in prior publications regarding hallux valgus, the patient demographics and risk factors were not controlled for. Lastly, our study relied on single-day radiographic analysis of patients going through a progressive healing process—the exact time of union cannot be extrapolated because our follow-ups were set across discrete time points (categorical) whereas the actual healing process is continuous in nature. Patients often present before or after the discrete and categorical time points that we schedule them for, reflective of their individual and unique schedules. We included in our analysis the expressed mean time to union in weeks as a limited estimation of healing time in consideration that development of 2 cortices can occur at any time point between the 3-month and 6-month follow-up visit.
Regarding categorical delineation of metatarsal shift, we intentionally avoided using a fourth quartile of 0%-25%. The majority of our patients belonged to either the 50%-75% shift group or the ≥76% group, with zero patients in the ≤50% group having an intraoperative shift of less than 40%. As a collective experience, this category of shifts was done primarily in the beginning of the study between 2020 and 2021. Furthermore, performing an intraoperative metatarsal shift of 0%-25% would pose a major risk of inadequate correction of the hallux valgus deformity. As such, we lumped together the lower 2 quartiles into an ≤50% category.
Although outside the purview of this study, the notable and most prevalent complication was the need for removal of hardware. We hypothesize that this is most likely due to the type of screws used to fixate the metatarsal, as we have observed fewer patients receiving the beveled-style screws with reports of pain in contrast to more patients who received the flathead screws with higher rates of pain.
Despite such limitations, this study can guide expectations on patient recovery time after MIS surgery. We offer the perspective that, in light of an asymptomatic patient and radiographic evidence of neocortical bridge formations, the surgeon can use their clinical judgment and patient feedback to determine when to advance postoperative activities. More so, our analysis on metatarsal shift may provide technical recommendations for surgeons as the fourth-generation MIS hallux valgus procedure becomes increasingly adopted. It is the belief of our surgeons that a shift of greater than 75% of the distal metatarsal head during the procedure provides the greatest corrections and poses no additional risk to patient recovery time.
Conclusion
Given ongoing ambiguity in defining radiographic bony union, we propose a clinically practical definition: the presence of at least 2 neocortical bridges in an asymptomatic patient. This threshold was met by 92% of patients by an average of 13 weeks following fourth-generation MIS hallux valgus surgery. When more conservative criteria are preferred (3 cortices), union was typically achieved by 23 weeks. The degree of metatarsal shift during surgery was not associated with delayed healing, suggesting that more substantial deformity correction is safe in terms of union timing. These findings provide useful benchmarks for postoperative expectations and rehabilitation protocols.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251343549 – Supplemental material for Time to Radiographic Union Following Minimally Invasive META Procedure for Hallux Valgus
Supplemental material, sj-pdf-1-fao-10.1177_24730114251343549 for Time to Radiographic Union Following Minimally Invasive META Procedure for Hallux Valgus by Taylor Schnepp, Kyle Lorenzo, Chase Burzynski, Jason Mirharooni, Wade Massey, Thomas San Giovanni, Christopher W. Hodgkins and Cary B. Chapman in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
This study has been approved under Baptist Health Institutional Review Board, IRB # [1952671-5]
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Cary B. Chapman, MD, reports general disclosures as Enovis: consultant; Conventus: consultant. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.