
Abstract
Background:
Progressive collapsing flatfoot deformity (PCFD) is a complex condition characterized by hindfoot valgus, midfoot varus, and forefoot abduction, leading to functional impairment and pain. Surgical correction often includes lateral column lengthening (LCL), which addresses structural deformity and restores alignment. Autografts remain the gold standard as an osteotomy gap filler for LCL despite donor site morbidity. Allografts augmented with patient’s own bone marrow aspirate concentrate (BMAC) offer a potential alternative because of their osteogenic properties. This study compares the clinical and radiologic outcomes of autografts vs allografts with BMAC in LCL for PCFD.
Methods:
This retrospective study reviewed 38 patients who underwent LCL for PCFD at a tertiary institution from 2012 to 2022. Patients were divided into 2 groups: the 25 who received autografts (group A), and the 13 who received allografts (group B) mixed with BMAC. Clinical outcomes were assessed using visual analog scale (VAS), American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot scores, and 36-Item Short Form Health Survey (SF-36) scores at 6 and 24 months postoperatively. Radiologic union was evaluated through serial weightbearing radiographs at regular interval post-surgery.
Results:
Both groups A and B achieved radiologic union at an average of 5.64 ± 1.80 and 5.15 ± 2.58 months, respectively. There were no cases of delayed union or nonunion. Both groups demonstrated significant improvements in VAS, AOFAS, and SF-36 scores at 6 and 24 months, with no statistically significant differences in outcomes. Group A had 2 cases of peroneal tendinopathy, 1 case of peroneal tendon adhesion to the plate, 1 case of screw prominence, and 1 case of chronic pain attributed to plantar nerve irritation. Group B had no reported complications.
Conclusion:
This study suggests that allografts augmented with BMAC may be a viable alternative to autografts for LCL in PCFD, offering comparable union rates and functional outcomes. However, as a retrospective cohort study with a small sample size, further prospective research is needed to confirm these findings.
Level of Evidence:
Level III, retrospective cohort studies.
This is a visual representation of the abstract.
Keywords
Introduction
Lateral column lengthening (LCL) osteotomy is a well-established surgical intervention for addressing the structural deformity and restoring the mechanical alignment of the foot in progressive collapsing flatfoot deformity (PCFD).7,8,14,21,23 A cadaveric study, conducted by Baxter et al, involved performing LCL on 12 cadaveric flatfoot models. Findings revealed that LCL corrected 60% of hindfoot valgus deformity and completely resolved midfoot abduction. 3
However, the choice of graft material for filling the osteotomy gap remains a subject of debate. Autografts, harvested from the iliac crest or calcaneus, are considered the gold standard because of their osteogenic potential but come with donor site morbidity.2,5 Allografts provide a structural alternative without the need for a secondary surgical site, although their integration can be slower. Synthetic bone substitutes, such as hydroxyapatite or tricalcium phosphate, offer osteoconductive properties but lack osteoinductivity. Bioactive glass and composite grafts are also being explored for their biocompatibility. Precut metallic wedges too have been advocated in LCL for PFCD. 24 These glass and composite grafts and precut metallic wedges are not available at our institution.
Taking a closer look, the choice of autografts presents with donor-site morbidity, limited availability, and extended operative time are notable drawbacks.1,2,12 There have even been suggestions, in recent studies, of using bone graft obtained locally in the calcaneus to avoid donor-site morbidity.15,18,19 Allografts, on the other hand, offer practical advantages such as abundant availability and elimination of donor-site complications, but their use may be limited by theoretic poorer union rates because of reduced osteogenic potential, risk of disease transmission, and the risk of immune response.5,25,16 Nonunion rates as high as 15% when using tricortical iliac crest allografts have been reported. 9
To address these limitations, the incorporation of bone marrow aspirate concentrate (BMAC), derived from each patient’s own bone marrow, has been explored as a strategy to enhance osteogenesis and promote graft integration. BMAC is rich in mesenchymal stem cells, growth factors, and osteoprogenitor cells, offering a biologically active adjunct that may improve the outcomes of bone grafts. 11 Although BMAC has been increasingly used in orthopaedic surgery, its efficacy as an adjunct in the specific context of LCL remains unexplored.
This study aims to compare the clinical and radiologic outcomes of autografts vs allografts augmented with BMAC as osteotomy gap fillers in LCL procedure to provide evidence-based guidance for the selection of graft materials.
Methods
Patient Selection
This retrospective study of prospectively collected registry data was approved by the Centralised Institutional Review Board (approval number: CRIB 2019/2776) and carried out per the ethical standards laid down in the 1964 Declaration of Helsinki. Informed consent was also obtained from all participants. All consecutive patients with symptomatic PCFD who underwent surgical intervention at our tertiary institution by multiple, senior fellowship-trained orthopaedic surgeons between July 2012 and October 2022 were considered. Inclusion criteria encompassed all patients aged 21 years or older who underwent LCL in the management of PCFD. Exclusion criteria included previous surgeries on the ipsilateral foot, any neurologic causes of PCFD (eg, Charcot neuroarthropathy, cerebral palsy), use of autografts supplemented with platelet-rich plasma, and patients lost to follow-up within 2 years. A total of 38 patients met the study criteria (Figure 1).
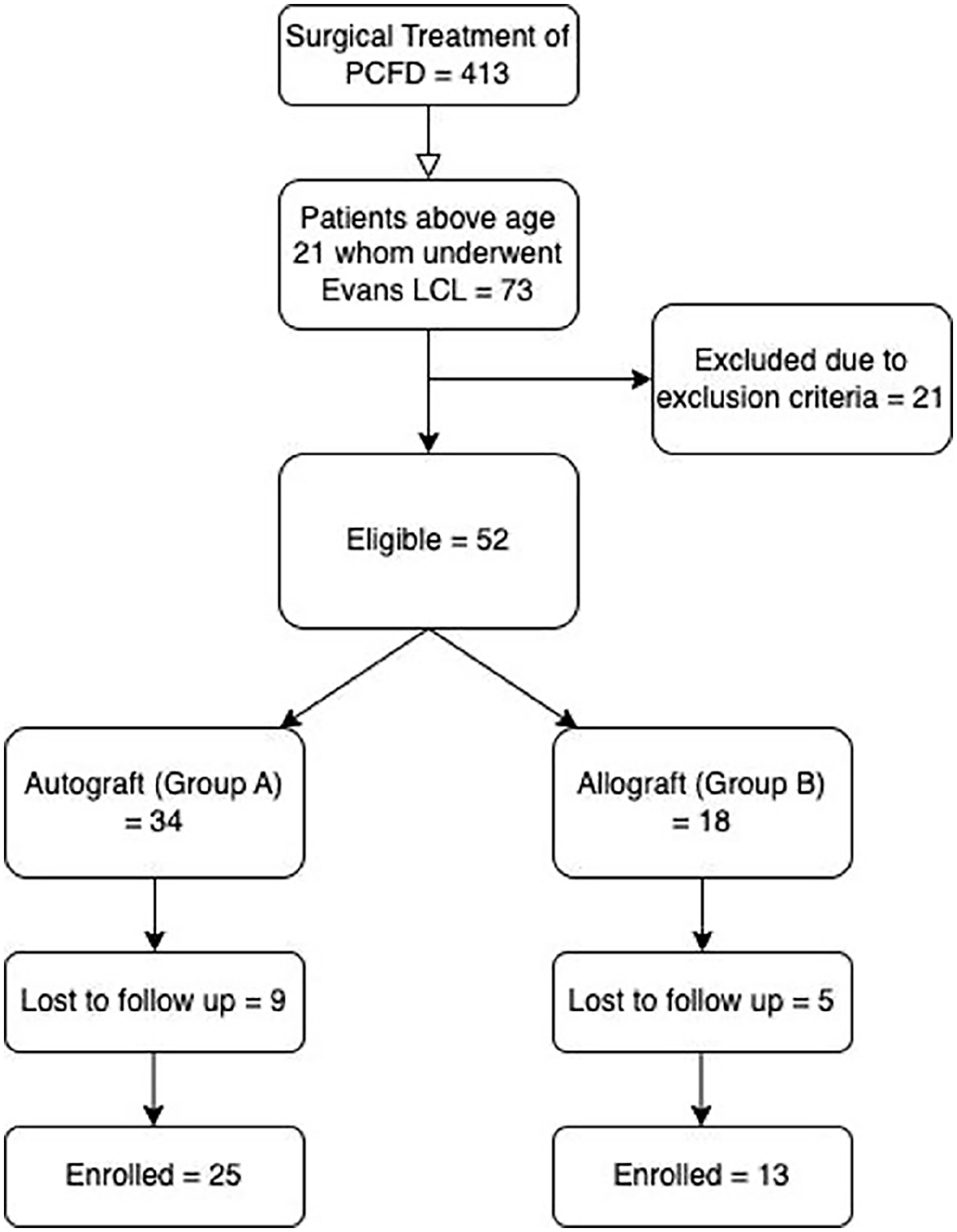
Patient selection.
Patients were divided into 2 groups based on the type of graft used. Twenty-five of the 38 feet used a tricortical autograft harvested from the patient’s ipsilateral iliac crest, whereas 13 feet had used allograft mixed with BMAC (Zimmer, Warsaw, IN) (Figure 1). The donor site was grafted with chronOS (Synthes, Solothurn, CH). All allografts (AlloSource, Centennial, CO) were tricortical blocks that were cut to fit the recipient site, which was noted to be trapezoidal in shape. BMAC was harvested from the ipsilateral upper tibial diaphysis before inflation of the tourniquet. The tricortical allografts were then soaked in BMAC, till the BMAC was visually seen to completely infiltrate the cancellous portion of the allograft.
Surgical technique
The patient was positioned in a floppy lateral decubitus position with the operative foot superior. Through an extended lateral approach, a subperiosteal flap was elevated to expose the lateral calcaneus for medializing calcaneal osteotomy. LCL was performed via an Evans osteotomy at the lateral calcaneal process, 10 to 15 mm proximal to the calcaneocuboid joint. Distraction was achieved with a Weinraub distractor, and the gap was filled with a trapezoidal tricortical graft, shaped to restore the medial arch. The graft was tamped flush without fixation (Figure 2). Patients were repositioned supine as needed for additional medial foot procedures, which were performed in 92.1% of cases (Table 1).

Preoperative (A) and postoperative (B) lateral weightbearing views of operated foot using allograft mixed with bone marrow aspirate concentrate.
Type of Concomitant Procedures.

Abbreviation: BMAC, bone marrow aspirate concentrate.
Postoperative Management
Patients from both groups were placed under similar postoperative management. Initially, patients are placed in a nonweightbearing back slab postoperatively, which is soon converted to a cast for 6-8 weeks to protect the osteotomy site. Elevation was encouraged during the early postoperative period to reduce swelling and pain. Regular radiographic follow-up, as elaborated below, was crucial to assess bone consolidation. Once healing is confirmed, patients are transitioned to partial and then full weightbearing in a walking boot, accompanied by physical therapy to restore range of motion, strength, and gait.
Evaluation of Radiologic and Clinical Outcomes
Patient-reported outcome measures (PROMs) evaluated include preoperative and postoperative assessments using the visual analog scale (VAS) for pain for midfoot and hindfoot, the American Orthopaedic Foot & Ankle Society (AOFAS) scores for the midfoot and hindfoot, and the physical component summary (PCS) and mental component summary (MCS) of the 36-Item Short Form Health Survey. PROM scores were measured by independent, trained physiotherapists involved in the pre- and postoperative evaluation of all orthopaedic patients at our institution. Therapists differentiated symptoms from midfoot and hindfoot accordingly. These findings were recorded preoperatively and at 6 and 24 months postoperatively.
Bony union was evaluated using preoperative and postoperative weightbearing radiographs of the operated foot in 2 planes. Postoperative radiographs were typically obtained at intervals of 2 weeks, 8 weeks, 4 months, 6 months, and 1 year.
Radiographic union was defined as the presence of osseous bridging across both sides of the graft in the absence of graft collapse or broken hardware.6,10,22,26 The radiographic assessments were performed by the radiologist reporting on the film and the operating surgeon. If there was no radiographic union noted at 6-month follow-up, the patient would be followed up at closer intervals of 1-2 months until radiographic union was achieved.
Statistical Analysis
Statistical analysis was performed using SPSS statistical software (version 25; SPSS Inc, Armonk, NY). Continuous data with normal distribution were reported as mean and SD and compared using the paired samples t test and independent samples t test. To identify the univariate outliers, demographic variables and self-report measures were converted into standardized z scores. None of the cases had a z score greater than 3.29. The significance level was set at P < .05. t tests were used for analysis of relationships between groups with independent samples, while repeated measures ANOVA was applied for analyzing within-group changes over time.
Results
Statistical analysis shows no significant differences in demographics between the 2 groups in terms of gender, operative side, age, and body mass index (Table 2). There was no difference in number or types of concomitant procedures performed between both groups either (Table 1).
Comparison between Autograft and Allograft in terms of Baseline Characteristics.

Abbreviation: BMI, body mass index.
The time to union was comparable between both groups with group A and group B achieving radiologic union at 5.64 ± 1.80 and 5.15 ± 2.58 months, respectively (P = .501)
At the 6-month follow-up, both group A and group B demonstrated significant improvements in VAS, AOFAS scores for midfoot and hindfoot, as well as MCS scores (Table 3). Comparison between both groups were not statistically significant. By the 24-month assessment, both groups demonstrated further improvements in VAS, AOFAS scores, and PCS and MCS scores compared with preoperative scores, with no discernible statistical variances between them.
Comparison of PROM Scores Across Group A and B Preoperatively and at 6- and 24-Month Follow-up. a

Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; MCS, mental component summary; PCS, physical component summary; PROM, patient-reported outcome measure; VAS, visual analog scale.
Boldface indicates significance (P < .05).
Significant reductions in pain and improvements in patient-reported functional outcomes for both groups was seen at 6 and 24 months for both groups whereas intergroup comparisons at these time intervals revealed no statistical differences, showing comparable effectiveness of the interventions employed (Table 3).
Furthermore, the study compared the mean degree of change in various variables of PROMs between group A and group B between different time points (preoperative vs 6 months and preoperative vs 24 months). In terms of VAS scores for the Midfoot, both groups showed a significant increase in improvement of scores from preoperative to 6 months and 24 months, with group B having a higher degree of change at both time points (P < .001 for both comparisons). Similar trends were observed for VAS scores for the hindfoot, AOFAS-midfoot, AOFAS-hindfoot, PCS, MCS, Physical Functioning (SFPF), Role Limitations due to Physical Health (SFRF), Bodily Pain (SFBP), General Health Perceptions (SFGH), Vitality (SFVI), Social Functioning (SFSF), Role Limitations due to Emotional Problems (SFRE), and Mental Health (SFMH), where both groups demonstrated significant improvements over time, and group B consistently had a higher degree of improvement at 6 and 24 months. In summary, both groups experienced improvements in various clinical outcomes from preoperative to 6 and 24 months, with group B generally exhibiting higher degree of improvement in scores, although these differences did not consistently reach statistical significance across all measures (Table 4).
Comparison of the Degree of Change in PROM Scores.
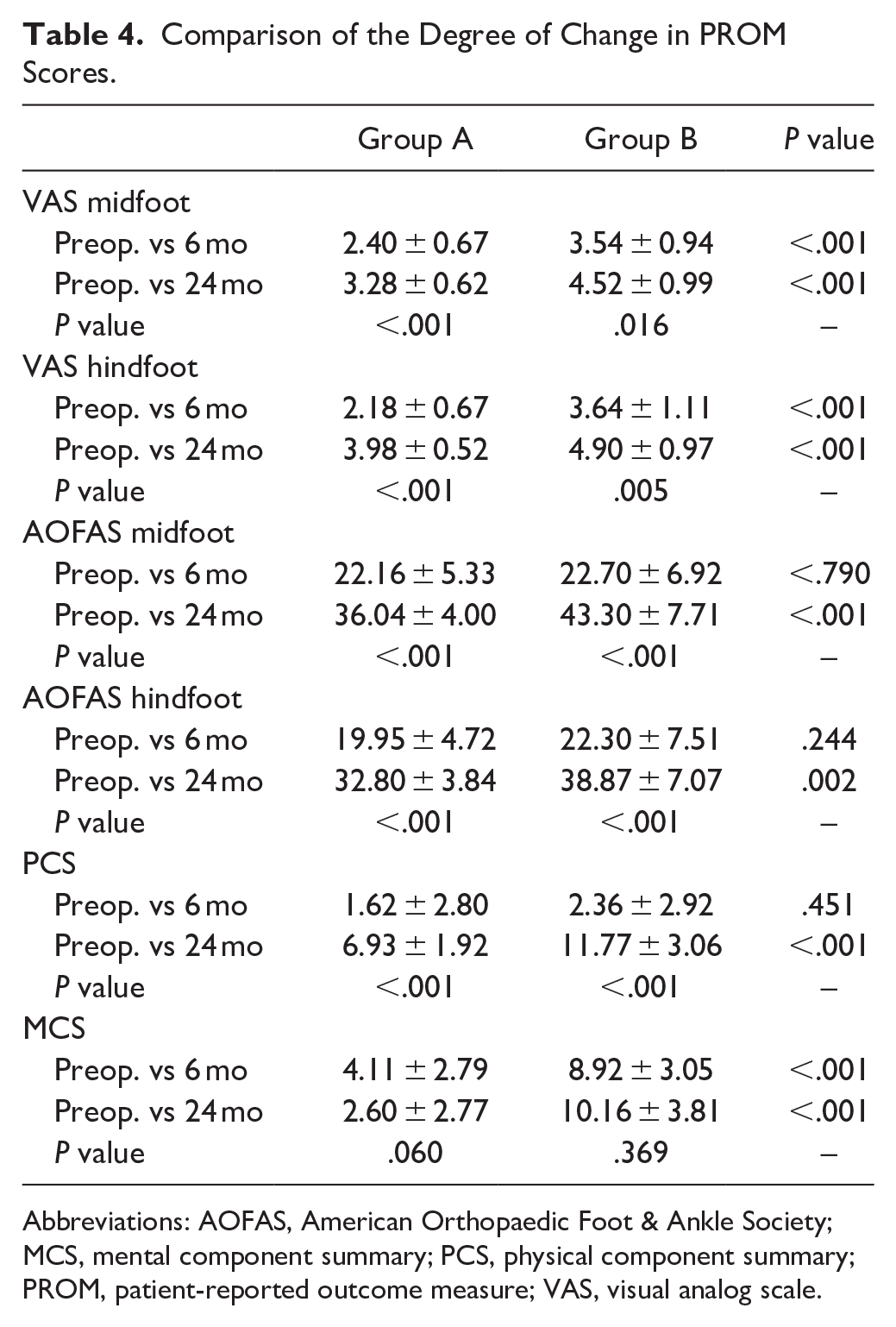
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; MCS, mental component summary; PCS, physical component summary; PROM, patient-reported outcome measure; VAS, visual analog scale.
Complications
No cases of non-union were observed in either group. In group A, there were no reported instances of donor site wound complications or persistent pain over the review period. However, complications related to LCL and associated implants included 2 cases of peroneal tendinopathy, 1 case of peroneal tendon adhesion to the plate (requiring subsequent tenolysis), implant removal in 1 patient due to screw prominence, and 1 case of chronic pain attributed to plantar nerve irritation. In contrast, no complications were reported in group B.
Discussion
The findings of this study indicate that both autografts and allografts augmented with BMAC are effective as osteotomy gap fillers in LCL for PCFD. However, interpretation should remain cautious given the study’s retrospective design, small group size, and lack of randomization. Radiologic union rates and PROMs demonstrated no statistically significant differences between the 2 groups. Dolan et al 6 similarly found that union rates of allograft and autograft (iliac crest bone graft) are equal in a study of 33 cases. Vosseller et al 26 found the rate of nonunion and loss of correction for LCL was not significantly different between allograft and autograft in a study of 126 operated feet. Grier and Walling 10 even documented better healing and complication rates with the use of allograft with platelet-rich plasma vs autograft for LCL, while allowing for similar correction of deformity. In a retrospective study of 50 patients, Müller et al 17 found the ratio of patients with loss of hindfoot alignment and graft incorporation was not significantly different between the allograft and autograft group.
Results of our study showing comparable time to union in both groups suggest that allografts augmented with BMAC can serve as a viable alternative to autografts, addressing some of the challenges associated with autograft use, such as donor-site morbidity and limited availability. Despite the theoretical advantages of autografts, including their inherent osteogenic, osteoconductive, and osteoinductive properties, the addition of BMAC to allografts may possibly bridge the gap in biological activity as an effective osteogenic adjunct. This observation aligns with prior research that has shown improved graft incorporation and union rates with BMAC augmentation. 25 The ability of BMAC to enhance the osteogenic potential of allografts may provide an effective strategy for mitigating concerns regarding reduced osteogenic capacity and immune response associated with allograft use.
Both groups demonstrated significant improvements in pain, functional scores, and quality of life as measured by VAS, AOFAS, and 36-Item Short Form Health Survey scores over a 24-month follow-up period. The absence of statistically significant differences between groups highlights the comparable efficacy of autografts and allografts with BMAC in achieving clinical improvements. Notably, both groups experienced substantial pain reduction and functional restoration within 6 months postoperatively, with further enhancements observed at 24 months. This progressive recovery trajectory highlights the effectiveness of LCL, together with other components of the surgery, in addressing the structural and symptomatic aspects of PCFD.
The significantly higher preoperative PCS scores observed in group A (autograft group) compared to group B (allograft group), with a mean of 41.18 ± 9.12 vs 34.45 ± 6.40 (P = .023), suggest better baseline physical well-being among patients in the autograft cohort. This disparity could stem from selection bias, as patients with better preoperative functional status may have been deemed more suitable candidates for autograft procedures, which typically involve longer operative times and the potential for donor site morbidity. Alternatively, the lower PCS scores in group B may reflect a greater severity of deformity or higher prevalence of comorbidities necessitating the use of allografts, which are often chosen for more complex cases or when autograft harvesting is contraindicated. These baseline differences could have influenced the postoperative recovery trajectory and functional outcomes. Although both groups demonstrated comparable improvements in VAS, AOFAS, and radiographic union rates, the lower preoperative physical health in group B highlights the importance of individualized patient selection and preoperative optimization to achieve optimal surgical outcomes.
The complication profile differed between the 2 groups, with no complications reported in the allograft group. In contrast, the autograft group experienced a range of complications, including peroneal tendinopathy, tendon adhesion, implant prominence, and nerve irritation. Reduced cases of tendinopathy, scarring, and nerve irritation in group B could be attributed to augmentation with BMAC, which is recognized for its antiinflammatory and immunomodulatory properties, thereby facilitating improved biological healing.13,27 Of note, there were no cases of donor site morbidity over the review period in group A, as this may be due to the donor site being grafted with chronOS, which is a beta-tricalcium phosphate filler. Dolan et al 6 reported that 2 of 18 patients had donor site chronic pain and Silber et al 20 who highlighted a considerable long-term impact on daily activities, with chronic pain affecting up to 26% of patients and more than 12% experiencing limitations in ambulation and recreational activities. Graft resorption was not observed in group B as has been reported by Boden et al. 4
There are several limitations in this study. First, its retrospective nature introduces potential biases related to data collection and analysis. These data were collected prospectively by our institution’s data collection center and analyzed retrospectively. Although the use of prospectively maintained registries mitigates this risk to some extent, a randomized controlled trial would provide a more robust evidence base. Second, the relatively small sample size, particularly in the allograft group, limits the statistical power and generalizability of the findings. Third, the study’s follow-up period, although sufficient to assess union rates and early functional outcomes, may not capture long-term complications like recurrence of deformity. Finally, the radiographic assessments, although performed independently, relied on subjective interpretations, which may introduce variability. Additionally, concomitant procedures performed alongside LCL were not controlled between groups, which may confound functional outcome comparisons despite similar distributions. Future studies should isolate LCL-specific outcomes more precisely. Moreover, standardized imaging protocols and objective measures of osteotomy healing would enhance the reliability of radiographic assessments in future studies.
Overall, the findings of this study have important implications for clinical practice. The comparable outcomes between autografts and allografts augmented with BMAC offer surgeons greater flexibility in graft selection, allowing for individualized treatment based on patient-specific factors. The absence of donor-site morbidity observed in the autograft group was an unexpected finding and may be attributable to the use of chronOS grafting material at the harvest site. However, the role of synthetic fillers in reducing donor site pain remains uncertain. Although the potential benefits of allograft use, including avoidance of a secondary surgical site, are well recognized, further prospective studies are needed to confirm these observations and fully assess their clinical impact.
Conclusion
This study demonstrates that allografts augmented with BMAC may be a viable alternative to autografts in LCL for PCFD, achieving comparable union rates, similar clinical improvements, and safety profiles. However, further research with larger, prospective cohorts and long-term follow-up is needed to validate these results and refine graft selection strategies in reconstructive foot and ankle surgery.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251342580 – Supplemental material for Autograft vs Allograft With Bone Marrow Aspirate Concentrate as an Osteotomy Gap Filler in Lateral Column Lengthening for Progressive Collapsing Flatfoot Deformity
Supplemental material, sj-pdf-1-fao-10.1177_24730114251342580 for Autograft vs Allograft With Bone Marrow Aspirate Concentrate as an Osteotomy Gap Filler in Lateral Column Lengthening for Progressive Collapsing Flatfoot Deformity by Ramesh Radhakrishnan, Don Thong Siang Koh, Eric Wei Liang Cher, Wenxian Png and Inderjeet Rikhraj Singh in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Centralised institutional review board approval (CIRB 2019/2776) was obtained for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.