
Abstract

Introduction
Chronic lateral ankle instability is a common cause of pain and disability in patients with lateral ankle sprains. 6 Previous arthroscopic techniques for lateral ligamentous complex repair are categorized as arthroscopic-assisted, all-arthroscopic, and all-inside. 2 The arthroscopic-assisted repair uses 1 or more accessory portals for suture passing and a mini-incision for ligament repair with sutures tied outside joint capsule. Suture irritation and superficial peroneal nerve injury are concerns with this technique. All-arthroscopic repairs rely on standard arthroscopy portals and an additional incision between percutaneous suture portals to tie over the capsular tissue and inferior extensor retinaculum. Again an additional small incision is required and there is percutaneous suture passage in this technique.1,7 All-inside techniques use standard arthroscopy portals with optional accessory portals with knotless intraarticular suture repair.7,9 Studies have reported complication rates of previous arthroscopic techniques. In a systematic review of arthroscopic repair, Alhaddad et al 4 reported complication rates of 2.3%, 1.5%, and 1.3% for superficial peroneal injury, persistent pain, and infection, respectively, in 1281 patients. Knot pain has not been captured frequently in studies but has been as high as 8%. 3
This technique article describes a new all-inside arthroscopic Brostrom lateral ligament reconstruction technique with SutureTape (Arthrex, Naples, FL) augmentation. In comparison with previously published techniques, this is an all-inside technique that does not require outside-in suture passage, knot tying, or any percutaneous suture passage. The technique also supplements direct native tissue repair with suture augmentation. Augmented repair may allow for earlier weightbearing and mobilization, potentially facilitating recovery. However, definitive evidence linking this approach to improved healing quality, faster return to sport, or better short-term functional scores remains limited and requires further study. 10
Indications and Contraindications
Indications for this arthroscopic procedure are almost the same as the open Brostrom repair. 1 Although suture augmentation may theoretically offer benefits in patients with hyperlaxity syndromes or collagen disorders, clinical outcomes in these populations have not been specifically studied and should be interpreted with caution. However, it is contraindicated in patients who have failed previous repair or have peroneal tendon pathology requiring concomitant open exposure for treatment.
Complications
Complications of this technique are similar to those previously reported for all-inside arthroscopic techniques including persistent lateral ankle pain, persistent laxity, wound complications, and infection. However, it does avoid issues related to subcutaneous suture passage or suture stack bulk and limits incisions to standard arthroscopic and at most accessory portals, potentially minimizing wound complication and infection risk.
Surgical Technique
The patient is supine. A 2.7-mm 30-degree arthroscope is used for diagnostic arthroscopy as typical for this procedure. Distraction of the ankle joint and tourniquet can be applied during the diagnostic portion of the arthroscopy, but should be removed to allow access to the lateral gutter during repair. If no distraction is used, the ankle can be placed in the distraction strap to maintain limb position.
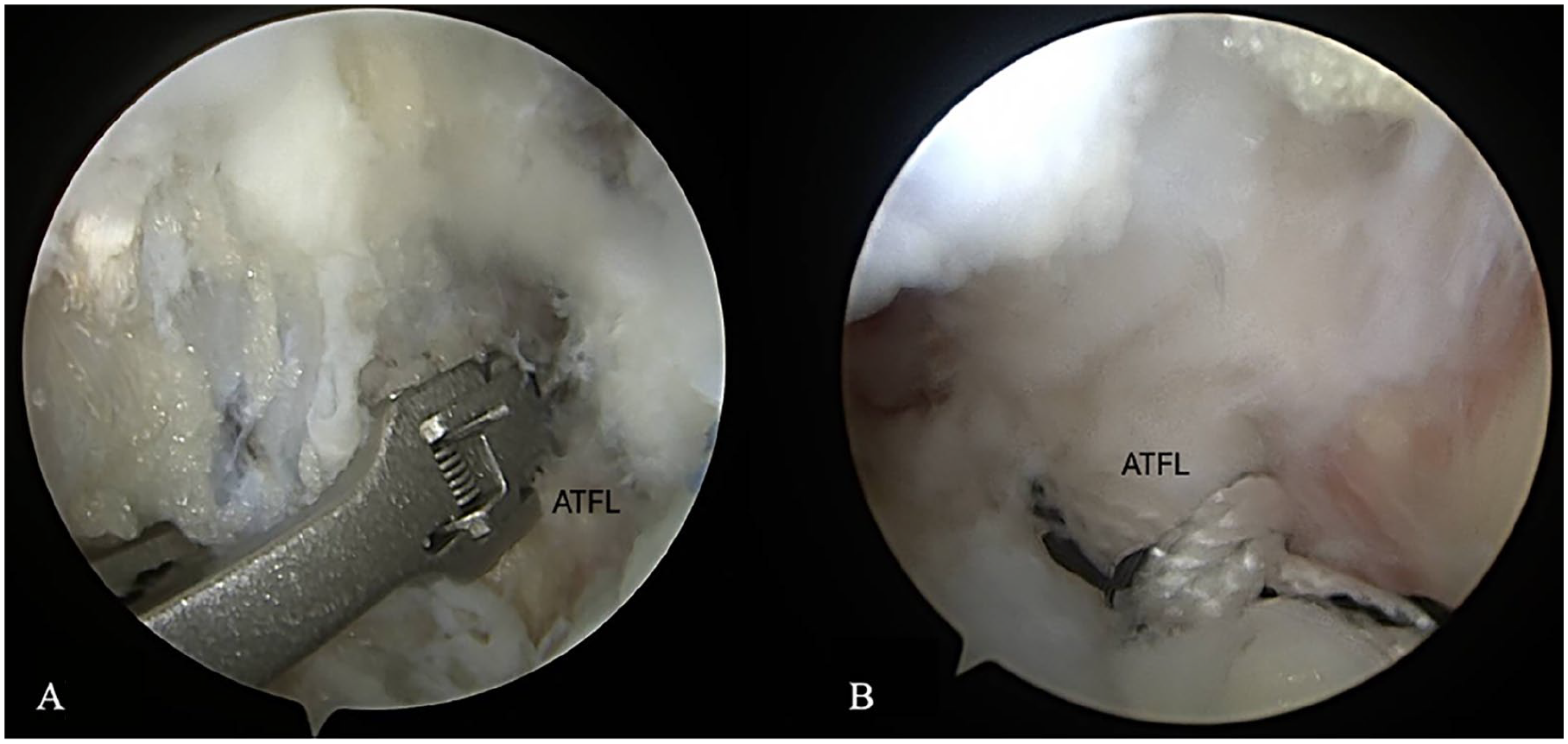
The joint is examined for intraarticular pathology such as osteochondral lesions, fibrosis, or scarring, which can be addressed concurrently. Debriding the fibrosis and soft tissue around the distal anterior fibula and lateral gutter is crucial for visualization; in particular, the Bassett ligament often must be excised (Figure 1).

(A) Bassett ligament usually needs to be debrided to visualize the anterior and distal fibula. (B) Preparation of the lateral gutter area for accessing the appropriate structures. ATFL, anterior talofibular ligament.
An arthroscopic biter, shaver, and cautery can assist with this process to clear tissue over the bone, but should be used with caution to preserve as much native lateral ligament tissue as possible.
The fibula is viewed through the anteromedial portal with the light source directed posteriorly, and the ankle dorsiflexed to open the lateral gutter. Through the anterolateral working portal, the fibular tunnel for the suture anchor can be prepared at 1.5 to 2 cm proximal to the fibular tip. This usually corresponds to the most distally visualized portion of the fibula on arthroscopy. The guidewire is placed anterior to posterior through the anterolateral portal, followed by drilling and then tapping over the guidewire. Care should be taken to protect the superficial peroneal nerve during this process (Figure 2).

(A) Wire trajectory into anterior face of the distal fibula at about 1.5 to 2 cm proximal to the fibular tip. (B) The wire is then overdrilled to an appropriate depth as marked on the drill. (C) The drill hole is then tapped to ensure later seating of the suture anchor.
The talar tunnel for inserting the SutureTape is then drilled into the talar insertion site of the ATFL. This is located on the lateral nonarticular surface of the talus, which is visualized through the anteromedial portal by directing the light source inferiorly and sometimes slightly anteriorly. Visualization of this landmark can be facilitated by dorsiflexion of the ankle (Figure 3).

(A) Drilling and (B) placement of the suture anchor into the lateral talus at the insertion site of the ATFL, as viewed through the anterolateral portal. (C) External appearance of the NanoNeedle high-flow sheath used as a soft tissue cannula to access the ATFL talus footprint. ATFL, anterior talofibular ligament.
If the trajectory for this tunnel is difficult, an accessory portal can be made about 0.5 cm distal and 0.5 cm lateral to the anterolateral portal. The Arthrex NanoNeedle (Arthrex) high-flow sheath cannula can then be positioned through the accessory portal to facilitate placement and drill trajectory (Figure 4).
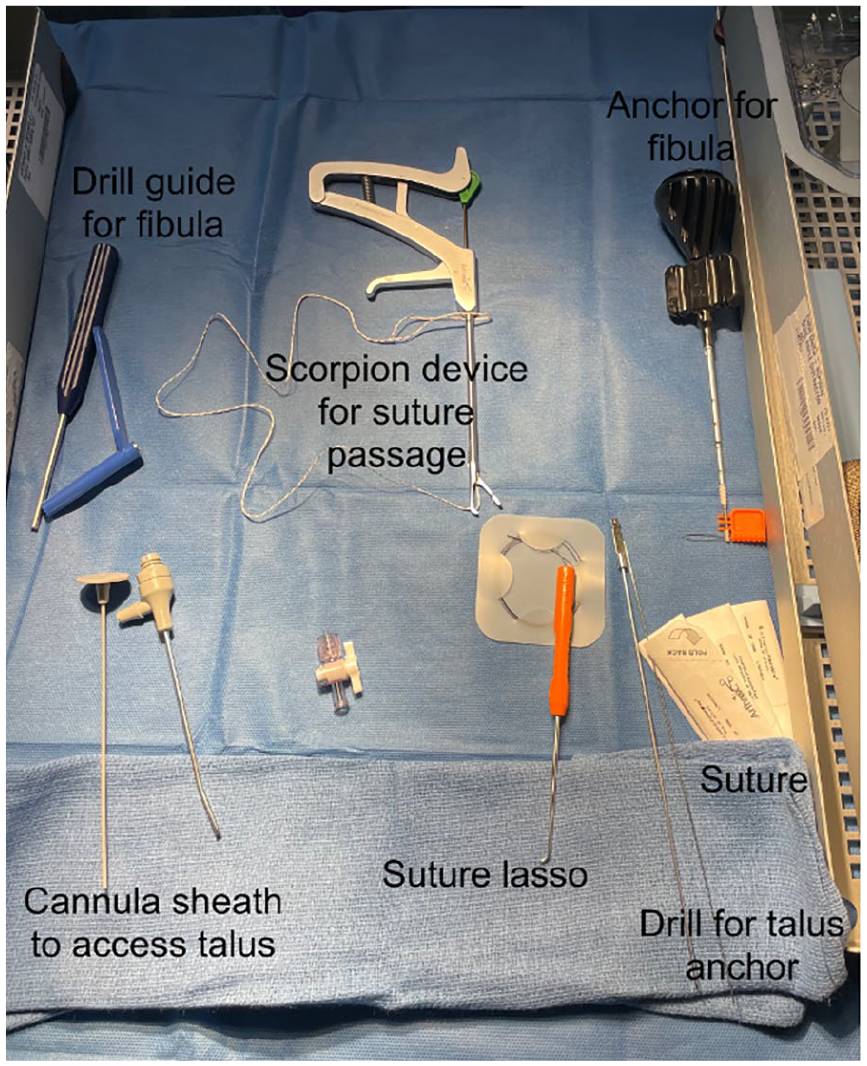
Equipment that is specific and helpful for performing the arthroscopic Brostrom technique.
The double-loaded suture anchor is then placed directly through the cannula into the talar tunnel. The sutures should be gently tugged to test secure placement. These sutures should then be retrieved through the anteromedial portal to provide working room. If the anchor was placed via the accessory portal, it is easier to pass the sutures out through the anterolateral then anteromedial portal.
An additional No. 0 FiberWire (Arthrex) luggage tag suture is then passed from lateral to medial through the remnant lateral ligament tissue distal to the fibula using a suture passer device (suture lasso or “mini scorpion”) via the anterolateral portal (Figure 5).
(A) Suture passer device that grabs and deploys suture through the native lateral ligament tissue to create the (B) luggage tag construct.
If the trajectory is difficult, suture passage can be performed through the accessory portal. The 3 sets of suture (2 from the talus anchor and 1 passed through the ligament tissue) are retrieved from the anterolateral portal, loaded into the eyelet, and inserted into the fibular tunnel (Figure 6).

(A) Placement of the suture anchor with the 3 sutures into the fibular tunnel. (B) Final construct after cutting the sutures flush to the anchor bone tunnel. (C) Another view of the repair with the ATFL remnant pulled with the SutureTape into the fibula anchor.
The ankle should be held in a neutral to 40 degrees plantarflexed position as this is the position of greatest length of the ATFL 8 and making sure to avoid dorsiflexion for anchor insertion to avoid overtightening. Caution must be used in this step as the native tissue repair and internal brace are attached back to the fibula with the same anchor placing them at the same tension. Although this technique departs from the lower-tension suture tape approach described by Coetzee et al, 5 the authors believe that equal tensioning of the native repair and internal brace can be performed safely without impairing ligament healing, provided that overtightening is carefully avoided. This theoretical rationale, however, has not yet been biomechanically validated. Ankle stability is then assessed after final insertion of the fibular anchor before the sutures are cut. Postoperatively the patient can be made nonweightbearing and immobilized in a short leg splint or weightbearing as tolerated immediately in a prefabricated boot. Minimal swelling is usually present as seen in Figure 7. At week 2, the patient can be transitioned to a boot or ankle brace and start physical therapy. They are instructed to advance passive plantarflexion or inversion as tolerated. An ankle brace is used for about 10-12 weeks, approximately when return to play for an athlete can be expected, which is similar to previously reported return to play using Brostrom repair with brace. 5

(A) Anteromedial and (B) anterolateral clinical photos 10 days status post left ankle all-inside arthroscopic Brostrom demonstrating minimal swelling.
Discussion
Overall, the authors believe the described technique incorporates the most beneficial aspects of an all-inside repair while avoiding the most common concerns with arthroscopic repair. The primary distinction from previously described arthroscopic techniques is the elimination of outside-in suture passage, subcutaneous knot stacks, and the need for additional mini-incisions. By incorporating suture tape augmentation, this approach theoretically strengthens the construct and may offer technical efficiency. However, clinical efficacy has not yet been evaluated in a comparative or prospective fashion.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251342576 – Supplemental material for All-Inside Arthroscopic Brostrom Repair with Suture Tape Augmentation: A Technical Description
Supplemental material, sj-pdf-1-fao-10.1177_24730114251342576 for All-Inside Arthroscopic Brostrom Repair with Suture Tape Augmentation: A Technical Description by Gerard F. Marciano, Sohil S. Desai, James R. McWilliam and Bonnie Y. Chien in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
This study was exempt from IRB approval as there were no study participants.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: James R. McWilliam, MD, reports disclosures of consulting, royalties from Arthrex, Inc. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.